Vascular Endothelial Growth Factor Receptor 2 (VEGFR2) rs2071559 Gene Polymorphism and the Risk of Gliomas: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Selection and Characteristics
3.2. Quality of Study Assessment
3.3. Classical Model
3.3.1. Dominant (CC + CT vs. TT)
3.3.2. Recessive (CC vs. CT + TT)
3.3.3. Allele (C vs. T)
3.4. Additional Model
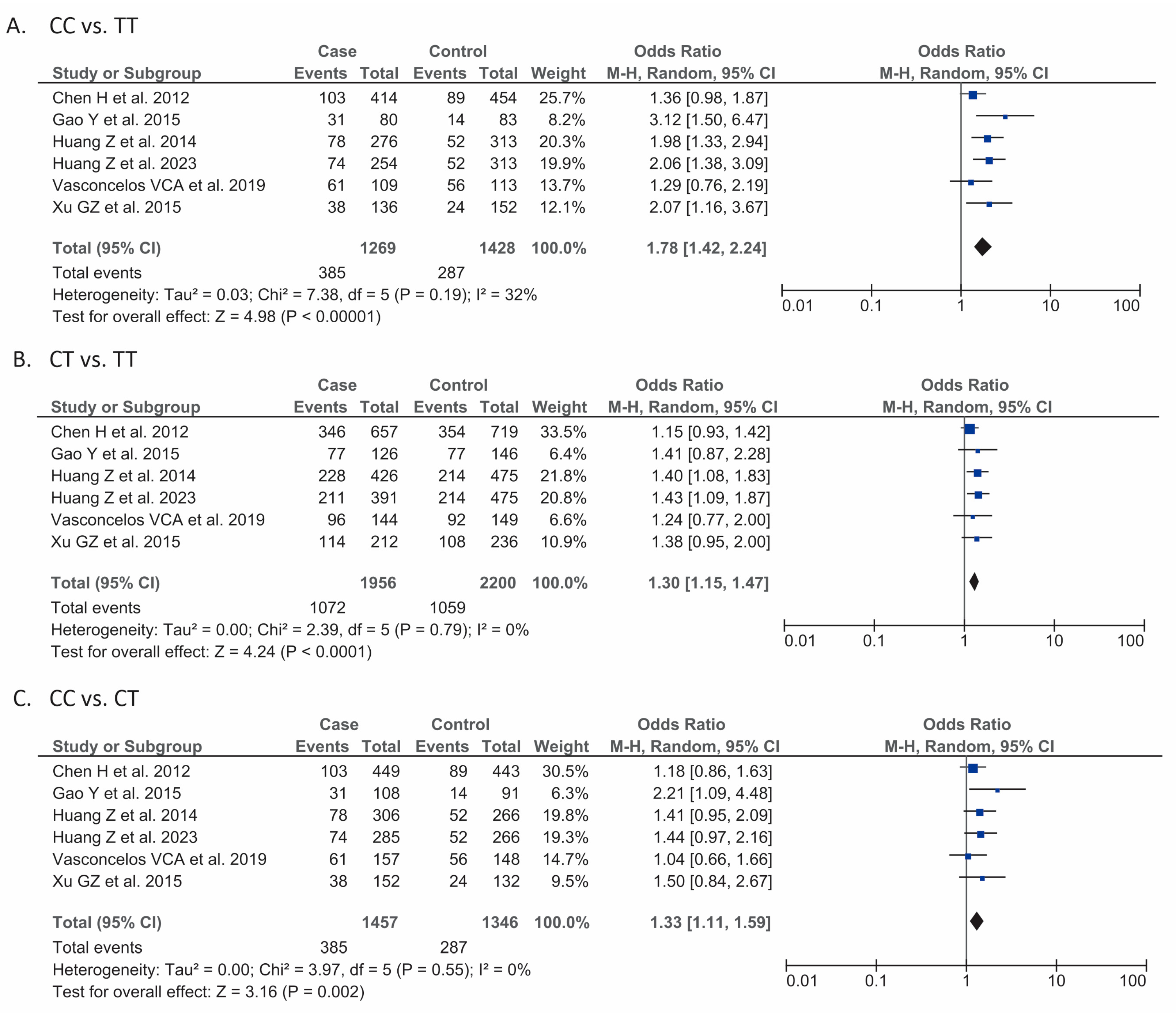
3.4.1. CC vs. TT
3.4.2. CT vs. TT
3.4.3. CC vs. CT
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weller, M.; Wick, W.; Aldape, K.; Brada, M.; Berger, M.; Pfister, S.M.; Nishikawa, R.; Rosenthal, M.; Wen, P.Y.; Stupp, R.; et al. Glioma. Nat. Rev. Dis. Primers 2015, 1, 15017. [Google Scholar] [CrossRef]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro Oncol. 2020, 22, 1073–1113. [Google Scholar] [CrossRef]
- Seker-Polat, F.; Pinarbasi Degirmenci, N.; Solaroglu, I.; Bagci-Onder, T. Tumor Cell Infiltration into the Brain in Glioblastoma: From Mechanisms to Clinical Perspectives. Cancers 2022, 14, 443. [Google Scholar] [CrossRef]
- Thon, N.; Tonn, J.C.; Kreth, F.W. The surgical perspective in precision treatment of diffuse gliomas. Onco Targets Ther. 2019, 12, 1497–1508. [Google Scholar] [CrossRef]
- Wang, Z.C. Wang Zhongcheng Neurosurgery, 2nd ed.; Wuhan Hubei Science and Technology Press: Wuhan, China, 2004; pp. 388–398. [Google Scholar]
- Tan, A.C.; Ashley, D.M.; López, G.Y.; Malinzak, M.; Friedman, H.S.; Khasraw, M. Management of glioblastoma: State of the art and future directions. CA Cancer J. Clin. 2020, 70, 299–312. [Google Scholar] [CrossRef]
- Molinaro, A.M.; Taylor, J.W.; Wiencke, J.K.; Wrensch, M.R. Genetic and molecular epidemiology of adult diffuse glioma. Nat. Rev. Neurol. 2019, 15, 405–417. [Google Scholar] [CrossRef]
- Yao, X.; Ping, Y.; Liu, Y.; Chen, K.; Yoshimura, T.; Liu, M.; Gong, W.; Chen, C.; Niu, Q.; Guo, D.; et al. Vascular endothelial growth factor receptor 2 (VEGFR-2) plays a key role in vasculogenic mimicry formation, neovascularization and tumor initiation by Glioma stem-like cells. PLoS ONE 2013, 8, e57188. [Google Scholar] [CrossRef]
- Xu, C.; Wu, X.; Zhu, J. VEGF promotes proliferation of human glioblastoma multiforme stem-like cells through VEGF receptor 2. Sci. World J. 2013, 2013, 417413. [Google Scholar] [CrossRef]
- Liu, G.; Fan, Y.P.; Zhao, X.J.; Han, C.Z. Correlation between the levels of vascular endothelial growth factor and its receptor Flt-1 and KDR in human brain glioma. Zhong Liu Yan Jiu Yu Lin Chuang 2006, 18, 812–814. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Chen, H.; Wang, W.; Zhao, X.; Song, X.; Fan, W.; Zhou, K.; Chen, G.; Zhao, Y.; Mao, Y.; Lu, D. Association between genetic variations of vascular endothelial growth factor receptor 2 and glioma in the Chinese Han population. J. Mol. Neurosci. 2012, 47, 448–457. [Google Scholar] [CrossRef]
- Gao, Y.; Ma, P.; He, Y.; Liu, Y.; Jiang, Y. Genetic Variations of Kinase Inserts Domain Receptor (KDR) Gene Are Associated with the Risk of Astrocytomas. Mol. Neurobiol. 2016, 53, 2541–2549. [Google Scholar] [CrossRef]
- Huang, Z.; Yao, X.; Yang, Y.; Chen, B.; Chen, H.; Lu, D.; Huang, H. Possible association between polymorphisms of VEGFR2 rs2071559 and glioma risk in Chinese population. Chin. J. Contemp. Neurol. Neurosurg. 2014, 14, 1007–1012. [Google Scholar]
- Huang, Z.F.; Zhu, W.; Wang, C.; Mo, L.D.; Huang, H.L.; Tong, X.G. Association of Kinase-Insert-Domain-Containing Receptor Polymorphisms with Glioma Susceptibility in a Chinese Population: A Hospital-Based Case-Control Study. Evid. Based Complement. Altern. Med. 2023, 2023, 8808422. [Google Scholar] [CrossRef]
- Vasconcelos, V.C.A.; Lourenço, G.J.; Brito, A.B.C.; Vasconcelos, V.L.; Maldaun, M.V.C.; Tedeschi, H.; Marie, S.K.N.; Shinjo, S.M.O.; Lima, C.S.P. Associations of VEGFA and KDR single-nucleotide polymorphisms and increased risk and aggressiveness of high-grade gliomas. Tumour Biol. 2019, 41, 1010428319872092. [Google Scholar] [CrossRef]
- Xu, G.Z.; Liu, Y.; Zhang, Y.; Yu, J.; Diao, B. Correlation between VEGFR2 rs2071559 polymorphism and glioma risk among Chinese population. Int. J. Clin. Exp. Med. 2015, 8, 16724–16728. [Google Scholar]
- Thornton, A.; Lee, P. Publication bias in meta-analysis: Its causes and consequences. J. Clin. Epidemiol. 2000, 53, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Terrin, N.; Schmid, C.H.; Lau, J.; Olkin, I. Adjusting for publication bias in the presence of heterogeneity. Stat. Med. 2003, 22, 2113–2126. [Google Scholar] [CrossRef] [PubMed]
- Stacker, S.A.; Caesar, C.; Baldwin, M.E.; Thornton, G.E.; Williams, R.A.; Prevo, R.; Jackson, D.G.; Nishikawa, S.I.; Kubo, H.; Achen, M.G. VEGF-D promotes the metastatic spread of tumor cells via the lymphatics. Nat. Med. 2001, 7, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, G.; Cohen, T.; Gengrinovitch, S.; Poltorak, Z. Vascular endothelial growth factor (VEGF) and its receptors. FASEB J. 1999, 13, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Ahir, B.K.; Engelhard, H.H.; Lakka, S.S. Tumor Development and Angiogenesis in Adult Brain Tumor: Glioblastoma. Mol. Neurobiol. 2020, 57, 2461–2478. [Google Scholar] [CrossRef] [PubMed]
- Orasanu, C.I.; Aschie, M.; Deacu, M.; Bosoteanu, M.; Vamesu, S.; Enciu, M.; Bălţătescu, G.I.; Cozaru, G.C.; Mitroi, A.F.; Voda, R.I. Implications of Cellular Immaturity in Necrosis and Microvascularization in Glioblastomas IDH-Wild-Type. Clin. Pract. 2022, 12, 1054–1068. [Google Scholar] [CrossRef] [PubMed]
- Tuettenberg, J.; Friedel, C.; Vajkoczy, P. Angiogenesis in malignant glioma—A target for antitumor therapy? Crit. Rev. Oncol. Hematol. 2006, 59, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Hou, W.T.; Zeng, L.; Li, Z.P.; Ge, W.; Yi, C.; Kang, J.P.; Li, W.M.; Wang, F.; Wu, D.B.; et al. Progress in the study of markers related to glioma prognosis. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7690–7697. [Google Scholar] [PubMed]
- Seyedmirzaei, H.; Shobeiri, P.; Turgut, M.; Hanaei, S.; Rezaei, N. VEGF levels in patients with glioma: A systematic review and meta-analysis. Rev. Neurosci. 2020, 32, 191–202. [Google Scholar] [CrossRef]
- Bruzaite, A.; Gedvilaite, G.; Kriauciuniene, L.; Liutkeviciene, R. Association of KDR (rs2071559, rs1870377), CFH (rs1061170, rs1410996) genes variants and serum levels with pituitary adenoma. Mol. Genet. Genom. Med. 2024, 12, e2289. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, K.; Zhen, Y.; Wang, D.; Wang, Y.; Chen, J.; Xu, J.; Hu, F.B.; Hui, R. VEGF receptor-2 variants are associated with susceptibility to stroke and recurrence. Stroke 2009, 40, 2720–2726. [Google Scholar] [CrossRef]
- Abdelgalil, A.A.; Monir, R.; Elmetwally, M.; Ghattas, M.H.; Bazeed, F.B.; Mesbah, N.M.; Abo-Elmatty, D.M.; Mehanna, E.T. The Relation of VEGFA, VEGFR2, VEGI, and HIF1A Genetic Variants and Their Serum Protein Levels with Breast Cancer in Egyptian Patients. Biochem. Genet. 2023, 62, 547–573. [Google Scholar] [CrossRef]
- Dong, G.; Guo, X.; Fu, X.; Wan, S.; Zhou, F.; Myers, R.E.; Bao, G.; Burkart, A.; Yang, H.; Xing, J. Potentially functional genetic variants in KDR gene as prognostic markers in patients with resected colorectal cancer. Cancer Sci. 2012, 103, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.B.; Zhan, M.X.; Zhao, W.; Liu, B.; Huang, J.W.; He, X.; Fu, S.R.; Zhao, Y.; Li, Y.; Hu, B.S.; et al. The relationship of kinase insert domain receptor gene polymorphisms and clinical outcome in advanced hepatocellular carcinoma patients treated with sorafenib. Med. Oncol. 2014, 31, 209. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, I.; Riera, P.; Andrés, M.; Altés, A.; Majem, M.; Blanco, R.; Capdevila, L.; Barba, A.; Barnadas, A.; Salazar, J. Prognostic effect of VEGF gene variants in metastatic non-small-cell lung cancer patients. Angiogenesis 2019, 22, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Garrigós, C.; Espinosa, M.; Salinas, A.; Osman, I.; Medina, R.; Taron, M.; Molina-Pinelo, S.; Duran, I. Single nucleotide polymorphisms as prognostic and predictive biomarkers in renal cell carcinoma. Oncotarget 2017, 8, 106551–106564. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Study ID | HWE Test | Cases | Control | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Authors | Country | Sample Size | Age (Mean ± SD) | Male (%) | Histological Type | Tumor Grade | Sample Size | Age (Mean ± SD) | Male (%) | |
| Chen H et al. [14] 2012 | China | 0.880 | 766 | 42.2 ± 16 | 59.1% | Astrocytoma = 37% Glioblastoma = 31.5% Other glioma = 31.5% | Not reported | 824 | 41.5 ± 18.4 | 59.5% |
| Gao Y et al. [15] 2015 | China | 0.247 | 157 | 42.7 ± 10.2 | 61.8% | Astrocytoma = 100% | 1–2 = 62.4% 3–4 = 37.6% | 160 | 41.3 ± 12.9 | 59.4% |
| Huang Z et al. [16] 2014 | China | 0.451 | 504 | 42.3 ± 15.8 | 59.3% | Astrocytoma = 34.3% Glioblastoma = 31.5% Other glioma = 34.1% | 1 = 9.7% 2 = 31.9% 3 = 18.1% 4 = 40.2% | 527 | 40.2 ± 16.3 | 55.4% |
| Huang Z et al. [17] 2023 | China | 0.424 | 465 | 42.2 ± 15.4 | 58.5% | Astrocytoma = 37.2% Glioblastoma = 34.2% Oligodendroglioma = 10.1% Ependymoma = 14.4% Mixed glioma = 4.1% | 1 = 10.5% 2 = 34.6% 3 = 19.6% 4 = 35.3% | 527 | 40.2 ± 16.3 | 55.4% |
| Vasconcelos VCA et al. [18] 2019 | Brazil | 0.390 | 205 | 51 ± 15.3 | 65.8% | High grade glioma = 100% (type not specified) | 3 = 17.5% 4 = 81.9% | 205 | 48 ± 8.1 | 48.7% |
| Xu GZ et al. [19] 2015 | China | >0.05 | 250 | 40.4 ± 11.8 | 54% | Type not specified | Not reported | 260 | 40.6 ± 11.4 | 54.2% |
| First Author, Year | Study Design | Selection a | Comparability b | Outcome c | Total Score | Result |
|---|---|---|---|---|---|---|
| Chen H et al. [14] 2012 | Case–control | **** | ** | *** | 9 | Good |
| Gao Y et al. [15] 2015 | Case–control | **** | ** | *** | 9 | Good |
| Huang Z et al. [16] 2014 | Case–control | *** | ** | *** | 8 | Good |
| Huang Z et al. [17] 2023 | Case–control | **** | ** | *** | 9 | Good |
| Vasconcelos VCA et al. [18] 2019 | Case–control | **** | ** | *** | 9 | Good |
| Xu GZ et al. [19] 2015 | Case–control | **** | ** | *** | 9 | Good |
| Outcome | Intervention | Included Studies | Outcome (95% CI) | p-Value | I2 (%) |
|---|---|---|---|---|---|
| Dominant model (CC + CT vs. TT) | |||||
| Sample size | <500 | 2 | OR: 1.44 (1.05–1.99) | 0.02 | 0 |
| ≥500 | 4 | OR: 1.22 (1.22–1.61) | <0.001 | 20 | |
| Region | Asia | 5 | OR: 1.41 (1.24–1.60) | <0.001 | 7 |
| Outside of Asia | 1 | OR: 1.26 (0.81–1.97) | 0.31 | - | |
| Age | <42.3 | 3 | OR: 1.37 (1.14–1.65) | <0.001 | 35 |
| ≥42.3 | 3 | OR: 1.49 (1.22–1.81) | <0.001 | 0 | |
| Male sex prevalence | <57% | 2 | OR: 1.54 (1.25–1.89) | <0.001 | 0 |
| ≥57% | 4 | OR: 1.34 (1.15–1.56) | <0.001 | 8 | |
| Recessive model (CC vs. CT + TT) | |||||
| Sample size | <500 | 3 | OR: 1.63 (0.73–3.63) | 0.23 | 75 |
| ≥500 | 4 | OR: 1.52 (1.26–1.84) | <0.001 | 0 | |
| Region | Asia | 5 | OR: 1.60 (1.32–1.94) | <0.001 | 11 |
| Outside of Asia | 1 | OR: 1.13 (0.73–1.73) | 0.58 | - | |
| Age | <42.3 | 3 | OR: 1.48 (1.19–1.85) | <0.001 | 3 |
| ≥42.3 | 3 | OR: 1.60 (1.06–2.40) | 0.02 | 55 | |
| Male sex prevalence | <57% | 2 | OR: 1.74 (1.27–2.37) | <0.001 | 0 |
| ≥57% | 4 | OR: 1.46 (1.11–1.93) | 0.007 | 44 | |
| Homozygote model (CC vs. TT) | |||||
| Sample size | <500 | 2 | OR: 1.93 (0.82–4.57) | 0.13 | 73 |
| ≥500 | 4 | OR: 1.76 (1.41–2.20) | <0.001 | 19 | |
| Region | Asia | 5 | OR: 1.88 (1.47–2.40) | <0.001 | 33 |
| Outside of Asia | 1 | OR: 1.29 (0.76–2.19) | 0.34 | - | |
| Age | <42.3 | 3 | OR: 1.72 (1.27–2.32) | <0.001 | 37 |
| ≥42.3 | 3 | OR: 1.90 (1.24–2.91) | 0.003 | 48 | |
| Male sex prevalence | <57% | 2 | OR: 2.06 (1.49–2.87) | <0.001 | 0 |
| ≥57% | 4 | OR: 1.69 (1.22–2.34) | 0.002 | 49 | |
| Heterozygote model (CT vs. TT) | |||||
| Sample size | <500 | 2 | OR: 1.32 (0.94–1.86) | 0.11 | 0 |
| ≥500 | 4 | OR: 1.30 (1.14–1.48) | <0.001 | 0 | |
| Region | Asia | 5 | OR: 1.31 (1.15–1.49) | <0.001 | 0 |
| Outside of Asia | 1 | OR: 1.24 (0.77–2.00) | 0.38 | - | |
| Age | <42.3 | 3 | OR: 1.27 (1.09–1.48) | 0.002 | 0 |
| ≥42.3 | 3 | OR: 1.37 (1.11–1.69) | 0.003 | 0 | |
| Male sex prevalence | <57% | 2 | OR: 1.41 (1.14–1.76) | 0.002 | 0 |
| ≥57% | 4 | OR: 1.26 (1.08–1.46) | 0.003 | 0 | |
| Heterozygote model (CC vs. CT) | |||||
| Sample size | <500 | 2 | OR: 1.45 (0.70–3.01) | 0.32 | 67 |
| ≥500 | 4 | OR: 1.33 (1.09–1.63) | 0.004 | 0 | |
| Region | Asia | 5 | OR: 1.39 (1.14–1.68) | <0.001 | 0 |
| Outside of Asia | 1 | OR: 1.04 (0.66–1.66) | 0.86 | - | |
| Age | <42.3 | 3 | OR: 1.31 (1.04–1.65) | 0.02 | 0 |
| ≥42.3 | 3 | OR: 1.38 (0.97–1.98) | 0.08 | 36 | |
| Male sex prevalence | <57% | 2 | OR: 1.46 (1.05–2.03) | 0.02 | 0 |
| ≥57% | 4 | OR: 1.29 (1.02–1.63) | 0.03 | 15 | |
| Allele model (C vs. T) | |||||
| Sample size | <500 | 2 | OR: 1.35 (0.96–1.90) | 0.08 | 62 |
| ≥500 | 3 | OR: 1.44 (1.27–1.63) | <0.001 | 0 | |
| Region | Asia | 4 | OR: 1.46 (1.30–1.64) | <0.001 | 0 |
| Outside of Asia | 1 | OR: 1.15 (0.87–1.51) | 0.33 | - | |
| Age | <42.3 | 2 | OR: 1.45 (1.23–1.71) | <0.001 | 0 |
| ≥42.3 | 3 | OR: 1.38 (1.16–1.64) | <0.001 | 30 | |
| Male sex prevalence | <57% | 2 | OR: 1.45 (1.23–1.71) | <0.001 | 0 |
| ≥57% | 3 | OR: 1.38 (1.16–1.64) | <0.001 | 30 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prasetiyo, P.D.; Wahjoepramono, E.J. Vascular Endothelial Growth Factor Receptor 2 (VEGFR2) rs2071559 Gene Polymorphism and the Risk of Gliomas: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 4332. https://doi.org/10.3390/jcm13154332
Prasetiyo PD, Wahjoepramono EJ. Vascular Endothelial Growth Factor Receptor 2 (VEGFR2) rs2071559 Gene Polymorphism and the Risk of Gliomas: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(15):4332. https://doi.org/10.3390/jcm13154332
Chicago/Turabian StylePrasetiyo, Patricia Diana, and Eka Julianta Wahjoepramono. 2024. "Vascular Endothelial Growth Factor Receptor 2 (VEGFR2) rs2071559 Gene Polymorphism and the Risk of Gliomas: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 15: 4332. https://doi.org/10.3390/jcm13154332
APA StylePrasetiyo, P. D., & Wahjoepramono, E. J. (2024). Vascular Endothelial Growth Factor Receptor 2 (VEGFR2) rs2071559 Gene Polymorphism and the Risk of Gliomas: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(15), 4332. https://doi.org/10.3390/jcm13154332