

The Usefulness of Coregistration with iFR in Tandem or Long Diffuse Coronary Lesions: The iLARDI Randomized Clinical Trial
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.4. Endpoints
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
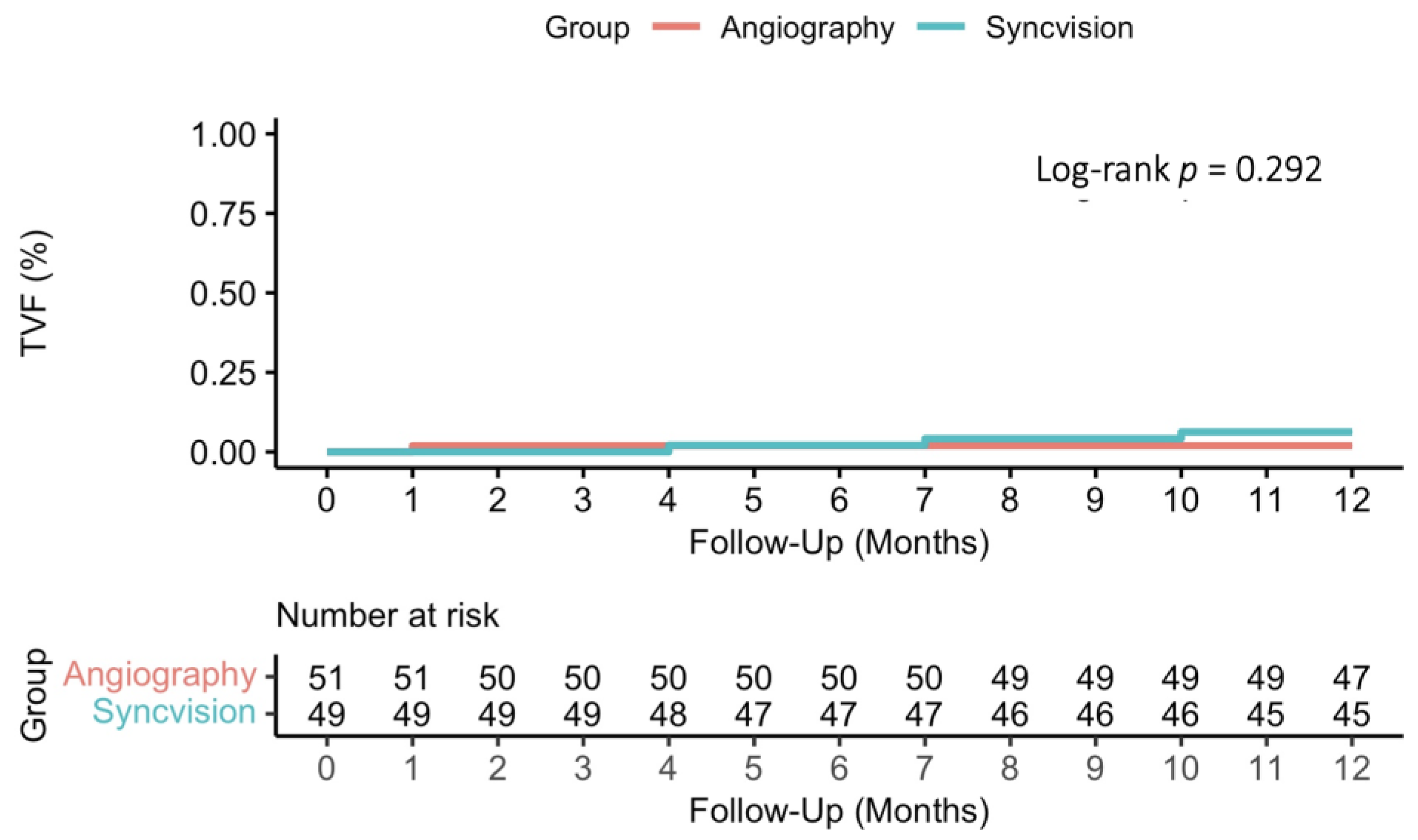
3.2. Primary and Secondary Endpoints
3.3. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Nijjer, S.S.; Sen, S.; Petraco, R.; Mayet, J.; Francis, D.P.; Davies, J.E.R. The Instantaneous Wave-Free Ratio (iFR) pullback: A novel innovation using baseline physiology to optimize coronary angioplasty in tandem lesions. Cardiovasc. Revasc. Med. 2015, 16, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Nijjer, S.S.; Sen, S.; Petraco, R.; Escaned, J.; Echavarria-Pinto, M.; Broyd, C.; Al-Lamee, R.; Foin, N.; Foale, R.A.; Malik, I.S.; et al. Pre-angioplasty instantaneous wave-free ratio pullback provides virtual intervention and predicts hemodynamic outcomes for serial lesions and diffuse coronary disease. JACC Cardiovasc. Interv. 2014, 7, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, Y.; Cook, C.M.; Sharp, A.S.; Salinas, P.; Kawase, Y.; Shiono, Y.; Giavarini, A.; Nakayama, M.; De Rosa, S.; Sen, S.; et al. Pre-Angioplasty instantaneous wave-free ratio pullback predicts hemodynamic outcome in human with coronary artery disease: Primary results of the international multicenter iFR GRADIENT registry. JACC Cardiovasc. Interv. 2018, 11, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Escaned, J.; Berry, C.; De Bruyne, B.; Shabbir, A.; Collet, C.; Lee, J.M.; Appelman, Y.; Barbato, E.; Biscaglia, S.; Buszman, P.P.; et al. Applied coronary physiology for planning and guidance of percutaneous coronary interventions. A clinical statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) of the European Society of Cardiology. Eurointervention 2023, 19, 464–481. [Google Scholar] [CrossRef] [PubMed]
- Collison, D.; Didagelos, M.; Aetesam-ur-Rahman, M.; Copt, S.; McDade, R.; McCartney, P.; Ford, T.J.; McClure, J.; Lindsay, M.; Shaukat, A.; et al. Post-stenting fractional flow reserve vs coronary angiography for optimization of percutaneous coronary intervention (TARGET-FFR). Eur. Heart J. 2021, 42, 4656–4668. [Google Scholar] [CrossRef] [PubMed]
- Jeremias, A.; Davies, J.E.; Maehara, A.; Matsumura, M.; Schneider, J.; Tang, K.; Talwar, S.; Marques, K.; Shammas, N.W.; Gruberg, L.; et al. Blinded physiological assessment of residual ischemia after successful angiographic percutaneous coronary intervention: The DEFINE PCI study. JACC Cardiovasc. Interv. 2019, 12, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.K.; Kasula, S.; Hacioglu, Y.; Ahmed, Z.; Uretsky, B.F.; Hakeem, A. Utilizing post-intervention Fractional Flow Reserve to optimize acute results and the relationship to long-term outcomes. JACC Cardiovasc. Interv. 2016, 9, 1022–1031. [Google Scholar] [CrossRef]
- Uretsky, B.F.; Agarwal, S.K.; Vallurupalli, S.; Al-Hawwas, M.; Hasan, R.; Miller, K.; Hakeem, A. Prospective evaluation of the strategy of functionally optimized coronary intervention. J. Am. Heart Assoc. 2020, 9, e015073. [Google Scholar] [CrossRef]
- Hidalgo, F.; Ojeda, S.; de Lezo, J.S.; Romero, M.; Lostalo, A.; González, R.; Pericet, C.; Paredes, N.; Elizalde, J.C.; Luque, A.; et al. Usefulness of a co-registration strategy with iFR in long and/or diffuse coronary lesions (iLARDI): Study protocol. REC Interv. Cardiol. 2021, 3, 190–195. [Google Scholar] [CrossRef]
- Garcia-Garcia, H.M.; McFadden, E.P.; Farb, A.; Mehran, R.; Stone, G.W.; Spertus, J.; Onuma, Y.; Morel, M.A.; van Es, G.A.; Zuckerman, B.; et al. Standardized End Point Definitions for Coronary Intervention Trials: The Academic Research Consortium-2 Consensus Document. Circulation 2018, 137, 2635–2650. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; vant Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional Flow Reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Xaplanteris, P.; Fournier, S.; Pijls, N.H.; Fearon, W.F.; Barbato, E.; Tonino, P.A.; Engstrøm, T.; Kääb, S.; Dambrink, J.H.; Rioufol, G.; et al. Five-year outcomes with PCI guided by Fractional Flow Reserve. N. Engl. J. Med. 2018, 379, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Götberg, M.; Christiansen, E.H.; Gudmundsdottir, I.J.; Sandhall, L.; Danielewicz, M.; Jakobsen, L.; Olsson, S.E.; Öhagen, P.; Olsson, H.; Omerovic, E.; et al. Instantaneous Wave-free Ratio versus Fractional Flow Reserve to guide PCI. N. Engl. J. Med. 2017, 376, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.E.; Sen, S.; Dehbi, H.M.; Al-Lamee, R.; Petraco, R.; Nijjer, S.S.; Bhindi, R.; Lehman, S.J.; Walters, D.; Sapontis, J.; et al. Use of the Instantaneous Wave-free Ratio or Fractional Flow Reserve in PCI. N. Engl. J. Med. 2017, 376, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Yang, L.F.; Zhai, J.L.; Li, J.; Wang, Q.M.; Zhang, R.J.; Wang, S.; Peng, Z.H.; Li, M.; Sun, G. SPECT myocardial perfusion versus fractional flow reserve for evaluation of functional ischemia: A meta analysis. Eur. J. Radiol. 2014, 83, 951–956. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Asrress, K.N.; Nijjer, S.; Petraco, R.; Malik, I.S.; Foale, R.A.; Mikhail, G.W.; Foin, N.; Broyd, C.; Hadjiloizou, N.; et al. Diagnostic classification of the instantaneous wave-free ratio is equivalent to fractional flow reserve and is not improved with adenosine administration. Results of CLARIFY (Classification Accuracy of Pressure-Only Ratios Against Indices Using Flow Study). J. Am. Coll. Cardiol. 2013, 61, 1409–1420. [Google Scholar] [CrossRef] [PubMed]
- Petraco, R.; Escaned, J.; Sen, S.; Nijjer, S.; Asrress, K.N.; Echavarria-Pinto, M.; Lockie, T.; Khawaja, M.Z.; Cuevas, C.; Foin, N.; et al. Classification performance of instantaneous wave-free ratio (iFR) and fractional flow reserve in a clinical population of intermediate coronary stenoses: Results of the ADVISE registry. Eurointervention 2013, 9, 91–101. [Google Scholar] [CrossRef]
- Sen, S.; Nijjer, S.; Petraco, R.; Malik, I.S.; Francis, D.P.; Davies, J. Instantaneous wave-free ratio: Numerically different, but diagnostically superior to FFR? Is lower always better? J. Am. Coll. Cardiol. 2013, 62, 566. [Google Scholar] [CrossRef]
- Sen, S.; Escaned, J.; Malik, I.S.; Mikhail, G.W.; Foale, R.A.; Mila, R.; Tarkin, J.; Petraco, R.; Broyd, C.; Jabbour, R.; et al. Development and validation of a new adenosine-independent index of stenosis severity from coronary wave-intensity analysis: Results of the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study. J. Am. Coll. Cardiol. 2012, 59, 1392–1402. [Google Scholar] [CrossRef] [PubMed]
- Sen, S.; Ahmad, Y.; Dehbi, H.M.; Howard, J.P.; Iglesias, J.F.; Al-Lamee, R.; Petraco, R.; Nijjer, S.; Bhindi, R.; Lehman, S.; et al. Clinical events after deferral of LAD revascularization following physiological coronary assessment. J. Am. Coll. Cardiol. 2019, 73, 444–453. [Google Scholar] [CrossRef]
- Matsuo, A.; Kasahara, T.; Ariyoshi, M.; Irie, D.; Isodono, K.; Tsubakimoto, Y.; Sakatani, T.; Inoue, K.; Fujita, H. Utility of angiography-physiology coregistration maps during percutaneous coronary intervention in clinical practice. Cardiovasc. Interv. Ther. 2021, 36, 208–218. [Google Scholar] [CrossRef]
- Pericet-Rodríguez, C.; Hidalgo-Lesmes, F.G.; González-Manzanares, R.; Ojeda-Pineda, S.; Luque-Moreno, A.; Suárez de Lezo, J. Usefulness of physiological coronary assessment with iFR in daily practice and all-comer patients: Immediate and follow-up results. REC Interv. Cardiol. 2021, 3, 182–189. [Google Scholar] [CrossRef]
- Costa, M.A.; Angiolillo, D.J.; Tannenbaum, M.; Driesman, M.; Chu, A.; Patterson, J.; Kuehl, W.; Battaglia, J.; Dabbons, S.; Shamoon, F.; et al. Impact of stent deployment procedural factors on long-term effectiveness and safety of sirolimus-eluting stents (final results of the multicenter prospective STLLR trial). Am. J. Cardiol. 2008, 101, 1704–1711. [Google Scholar]
- Coner, A.; Cicek, D.; Akinci, S.; Balcioglu, S.; Altin, C.; Muderrisoglu, H. Mid-term clinical outcomes of new generation drug-eluting stents for treatment of diffuse coronary artery disease. Turk. Kardiyol. Dern. Ars. 2018, 46, 659–666. [Google Scholar] [PubMed]
- Eftekhari, A.; Holck, E.N.; Westra, J.; Olsen, N.T.; Bruun, N.H.; Jensen, L.O.; Engstrøm, T.; Christiansen, E.H. Instantaneous wave-free ratio vs. fractional flow reserve and 5-year mortality: iFR SWEDHEART and DEFINE FLAIR. Eur. Heart J. 2023, 44, 4376–4384. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| S-iFR n = 49 | Angiography n = 51 | p | |
|---|---|---|---|
| Male sex | 37 (75.5) | 40 (78.4) | 0.729 |
| Age (years) | 69.0 ± 9.5 | 67.5 ± 10.0 | 0.435 |
| Hypertension | 35 (71.4) | 28 (54.9) | 0.087 |
| Diabetes mellitus | 22 (44.9) | 16 (31.4) | 0.164 |
| Dyslipidemia | 31 (63.3) | 29 (56.9) | 0.514 |
| Smoker | 8 (16.3) | 18 (35.3) | 0.031 |
| Prior coronary artery disease | 10 (20.4) | 9 (17.6) | 0.725 |
| Previous revascularization | 0.999 | ||
| Percutaneous | 13 (92.9) | 10 (100) | |
| Surgical | 1 (7.1) | 0 | |
| Atrial fibrillation | 2 (4.1) | 4 (7.8) | 0.678 |
| Heart failure | 7 (14.3) | 4 (7.8) | 0.303 |
| Prior stroke | 2 (4.1) | 4 (7.8) | 0.678 |
| Peripheral atherosclerosis | 5 (10.2) | 3 (5.9) | 0.483 |
| Previous major bleeding | 1 (2.0) | 0 | 0.490 |
| Hemoglobin (mg/dL) | 13.7 ± 1.7 | 14.1 ± 1.7 | 0.264 |
| Creatinine (mg/dL) | 0.9 (0.8–1.1) | 0.9 (0.8–1.1) | 0.894 |
| LVEF (%) | 59 (50–60) | 60 (49–65) | 0.591 |
| Clinical presentation | 0.837 | ||
| Stable angina | 22 (44.9) | 20 (39.2) | |
| Unstable angina-NSTEMI | 16 (32.7) | 19 (37.3) | |
| STEMI | 11 (22.4) | 12 (23.5) |
| S-iFR n = 49 | Angiography n = 51 | p | |
|---|---|---|---|
| Radial access | 49 (100) | 50 (98) | 0.999 |
| Multivessel disease | 27 (55) | 34 (67) | 0.236 |
| Syntax score | 15 (9.5–24) | 15 (10–21) | 0.858 |
| Number of vessels to revascularize | 1 (1–2) | 2 (1–2) | 0.090 |
| Randomized vessel | 0.117 | ||
| LAD | 34 (69) | 35 (69) | |
| LCx | 3 (6) | 9 (18) | |
| RCA | 12 (25) | 7 (14) | |
| Other | 0 (0) | 0 (0) | |
| Type of lesion | 0.491 | ||
| Tandem lesion | 42 (86) | 46 (90) | |
| Long diffuse | 7 (14) | 5 (10) | |
| Vessel reference diameter | 2.5 (2.5–3) | 3.0 (2.5–3) | 0.034 |
| Vessel stenosis | 80 (70–80) | 75 (70–80) | 0.399 |
| Vessel MLD (mm) | 0.6 (0.5–0.9) | 0.8 (0.5–0.9) | 0.055 |
| Vessel lesion length (mm) | 42.3 ± 12 | 39.8 ± 12 | 0.297 |
| Estimated stent length (mm) | 43.4 ± 13.5 | 41.0 ± 12.9 | 0.401 |
| Stent diameter (mm) | 2.5 (2.5–3.0) | 2.75 (2.5–3.0) | 0.029 |
| Baseline iFR | 0.71 ± 0.16 | 0.67 ± 0.19 | 0.279 |
| Procedural time (min) | 92 (70–105) | 87 (70–106) | 0.750 |
| Fluoroscopy time (min) | 20 (6–31) | 17 (9–25) | 0.442 |
| Radiation (Gy/cm2) | 155 ± 81 | 141 ± 81 | 0.440 |
| Contrast (mL) | 178 ± 56 | 177 ± 70 | 0.941 |
| Intraprocedural complications | 0 (0) | 1 (2) | 0.990 |
| Periprocedural myocardial infarction | 2 (4.2) | 4 (7.8) | 0.68 |
| Peak of troponin (ng/mL) | 0.9 (0.1–16.3) | 3.1 (0.3–22.6) | 0.177 |
| In-hospital complications | N/A | ||
| Bleeding | 0 (0) | 0 (0) | |
| Death | 0 (0) | 0 (0) | |
| Stroke | 0 (0) | 0 (0) | |
| Stent thrombosis | 0 (0) | 0 (0) | |
| Intracoronary imaging | 1 (2.0) | 5 (9.8) | 0.205 |
| Rotablation | 0 (0) | 0 (0) | N/A |
| Angiographic success | 49 (100) | 51 (100) | N/A |
| S-iFR n = 49 | Angiography n = 51 | Difference (CI 95%) | p | |
|---|---|---|---|---|
| Primary endpoint | ||||
| Implanted stent length (mm) | 32.7 ± 17.2 | 43.1 ± 14.9 | −10.4 (−16.9 to −4.0) | 0.002 |
| Other endpoints | ||||
| Difference implanted—estimated (mm) | −10.7 ± 13.2 | 2.1 ± 7.7 | −12.8 (−17.2 to −8.5) | 0.001 |
| Final iFR | 0.91 ± 0.03 | - | - | - |
| Estimated stent length by Syncvision to achieve an iFR > 0.89 (mm) | 29.2 ± 14.0 | - | - | - |
| Dots accumulation to predict an iFR improvement | 47 (94) | - | - | - |
| S-iFR n = 49 | Angiography n = 51 | Hazard Ratio or Risk Difference (CI 95%) | p | |
|---|---|---|---|---|
| Clinical secondary endpoints | ||||
| Target vessel failure | 3 (6.1) * | 1 (1.9) | 3.16 (0.33 to 30.37) | 0.319 |
| Cardiovascular death | 0 (0) | 1 (1.9) | −1.9 (−5.9 to 1.9) | 0.322 |
| Myocardial infarction | 2 (4.1) | 0 (0) | 4.1 (−1.7 to 9.8) | 0.159 |
| Stent thrombosis (definite or probable) | 0 (0) | 0 (0) | - | - |
| Target vessel revascularization | 2 (4.1) | 0 (0) | 4.1 (−1.7 to 9.8) | 0.159 |
| Target lesion revascularization | 2 (4.1) | 0 (0) | 4.1 (−1.7 to 9.8) | 0.159 |
| Stroke | 1 (2.0) | 1 (1.9) | 0.0 (−5.5 to 5.7) | 0.977 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidalgo, F.; Gonzalez-Manzanares, R.; Suárez de Lezo, J.; Gallo, I.; Alvarado, M.; Perea, J.; Maestre-Luque, L.C.; Resúa, A.; Romero, M.; López-Benito, M.; et al. The Usefulness of Coregistration with iFR in Tandem or Long Diffuse Coronary Lesions: The iLARDI Randomized Clinical Trial. J. Clin. Med. 2024, 13, 4342. https://doi.org/10.3390/jcm13154342
Hidalgo F, Gonzalez-Manzanares R, Suárez de Lezo J, Gallo I, Alvarado M, Perea J, Maestre-Luque LC, Resúa A, Romero M, López-Benito M, et al. The Usefulness of Coregistration with iFR in Tandem or Long Diffuse Coronary Lesions: The iLARDI Randomized Clinical Trial. Journal of Clinical Medicine. 2024; 13(15):4342. https://doi.org/10.3390/jcm13154342
Chicago/Turabian StyleHidalgo, Francisco, Rafael Gonzalez-Manzanares, Javier Suárez de Lezo, Ignacio Gallo, Marco Alvarado, Jorge Perea, Luis Carlos Maestre-Luque, Adriana Resúa, Miguel Romero, María López-Benito, and et al. 2024. "The Usefulness of Coregistration with iFR in Tandem or Long Diffuse Coronary Lesions: The iLARDI Randomized Clinical Trial" Journal of Clinical Medicine 13, no. 15: 4342. https://doi.org/10.3390/jcm13154342