

The Relationship between Placental Shear Wave Elastography and Fetal Weight—A Prospective Study

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Study Population
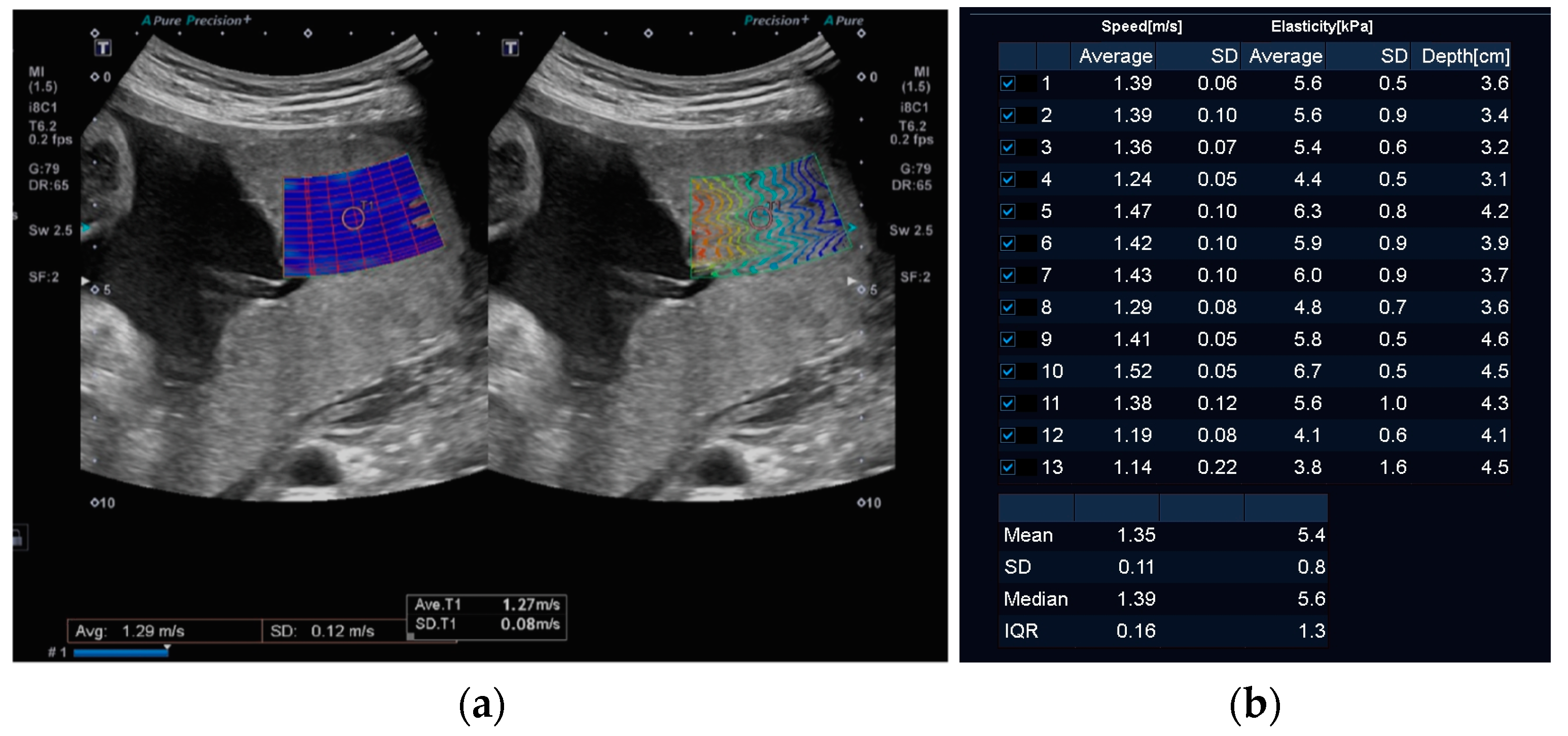
2.2. Equipment and Methods
2.3. Statistical Analysis
3. Results
Patient Demographics and Inclusion Criteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawn, J.E.; Ohuma, E.O.; Bradley, E.; Idueta, L.S.; Hazel, E.; Okwaraji, Y.B.; Erchick, D.J.; Yargawa, J.; Katz, J.; Lee, A.C.C.; et al. Small babies, big risks: Global estimates of prevalence and mortality for vulnerable newborns to accelerate change and improve counting. Lancet 2023, 401, 1707–1719. [Google Scholar] [CrossRef] [PubMed]
- Triggs, T.; Crawford, K.; Hong, J.; Clifton, V.; Kumar, S. The influence of birthweight on mortality and severe neonatal morbidity in late preterm and term infants: An Australian cohort study. Lancet Reg. Health West. Pac. 2024, 45, 101054. [Google Scholar] [CrossRef] [PubMed]
- Madden, J.V.; Flatley, C.J.; Kumar, S. Term small-for-gestational-age infants from low-risk women are at significantly greater risk of adverse neonatal outcomes. Am. J. Obs. Gynecol. 2018, 218, 525.e1–525.e9. [Google Scholar] [CrossRef]
- Martins, J.G.; Biggio, J.R.; Abuhamad, A. Society for Maternal-Fetal Medicine Consult Series #52: Diagnosis and management of fetal growth restriction: (Replaces Clinical Guideline Number 3, April 2012). Am. J. Obstet. Gynecol. 2020, 223, B2–B17. [Google Scholar] [CrossRef] [PubMed]
- de Mendonça, E.L.S.S.; de Lima Macêna, M.; Bueno, N.B.; de Oliveira, A.C.M.; Mello, C.S. Premature birth, low birth weight, small for gestational age and chronic non-communicable diseases in adult life: A systematic review with meta-analysis. Early Hum. Dev. 2020, 149, 105154. [Google Scholar] [CrossRef] [PubMed]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obs. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef] [PubMed]
- Levytska, K.; Higgins, M.; Keating, S.; Melamed, N.; Walker, M.; Sebire, N.J.; Kingdom, J.C. Placental Pathology in Relation to Uterine Artery Doppler Findings in Pregnancies with Severe Intrauterine Growth Restriction and Abnormal Umbilical Artery Doppler Changes. Am. J. Perinatol. 2017, 34, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Benton, S.J.; McCowan, L.M.; Heazell, A.E.; Grynspan, D.; Hutcheon, J.A.; Senger, C.; Burke, O.; Chan, Y.; Harding, J.E.; Yockell-Lelievre, J.; et al. Placental growth factor as a marker of fetal growth restriction caused by placental dysfunction. Placenta 2016, 42, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Kumar, S. Circulating biomarkers associated with placental dysfunction and their utility for predicting fetal growth restriction. Clin. Sci. 2023, 137, 579–595. [Google Scholar] [CrossRef]
- Giles, W.B.; Trudinger, B.J.; Baird, P.J. Fetal umbilical artery flow velocity waveforms and placental resistance: Pathological correlation. Br. J. Obs. Gynaecol. 1985, 92, 31–38. [Google Scholar] [CrossRef]
- Lees, C.C.; Romero, R.; Stampalija, T.; Dall’Asta, A.; DeVore, G.A.; Prefumo, F.; Frusca, T.; Visser, G.H.A.; Hobbins, J.C.; Baschat, A.A.; et al. Clinical Opinion: The diagnosis and management of suspected fetal growth restriction: An evidence-based approach. Am. J. Obs. Gynecol. 2022, 226, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Lees, C.C.; Stampalija, T.; Baschat, A.; da Silva Costa, F.; Ferrazzi, E.; Figueras, F.; Hecher, K.; Kingdom, J.; Poon, L.C.; Salomon, L.J.; et al. ISUOG Practice Guidelines: Diagnosis and management of small-for-gestational-age fetus and fetal growth restriction. Ultrasound Obs. Gynecol. 2020, 56, 298–312. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, V.; Hurst, C.; da Silva Costa, F.; Stoke, R.; Turner, J.; Kumar, S. Definitions matter: Detection rates and perinatal outcome for infants classified prenatally as having late fetal growth restriction using SMFM biometric vs ISUOG/Delphi consensus criteria. Ultrasound Obs. Gynecol. 2023, 61, 377–385. [Google Scholar] [CrossRef]
- Larsen, M.L.; Schreiber, V.; Krebs, L.; Hoei-Hansen, C.E.; Kumar, S. The magnitude rather than the rate of decline in fetal growth is a stronger risk factor for perinatal mortality in term infants. Am. J. Obs. Gynecol. MFM 2023, 5, 100780. [Google Scholar] [CrossRef] [PubMed]
- Özkaya, N.; Leger, D.; Goldsheyder, D.; Nordin, M. Mechanical Properties of Biological Tissues. In Fundamentals of Biomechanics: Equilibrium, Motion, and Deformation; Özkaya, N., Leger, D., Goldsheyder, D., Nordin, M., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 361–387. [Google Scholar]
- Akhtar, R.; Sherratt, M.J.; Cruickshank, J.K.; Derby, B. Characterizing the elastic properties of tissues. Mater. Today 2011, 14, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Ferraioli, G.; Parekh, P.; Levitov, A.B.; Filice, C. Shear wave elastography for evaluation of liver fibrosis. J. Ultrasound Med. 2014, 33, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, D.; Piscaglia, F.; Bamber, J.; Bojunga, J.; Correas, J.M.; Gilja, O.H.; Klauser, A.S.; Sporea, I.; Calliada, F.; Cantisani, V.; et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: Clinical applications. Ultraschall Med. 2013, 34, 238–253. [Google Scholar] [CrossRef]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef]
- Edwards, C.; Cavanagh, E.; Kumar, S.; Clifton, V.; Fontanarosa, D. The use of elastography in placental research—A literature review. Placenta 2020, 99, 78–88. [Google Scholar] [CrossRef]
- O’Hara, S.; Zelesco, M.; Sun, Z. Shear wave elastography of the maternal cervix: A transabdominal technique. Australas. J. Ultrasound Med. 2019, 22, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Alıcı Davutoglu, E.; Ariöz Habibi, H.; Ozel, A.; Yuksel, M.A.; Adaletli, I.; Madazlı, R. The role of shear wave elastography in the assessment of placenta previa-accreta. J. Matern. Fetal Neonatal Med. 2018, 31, 1660–1662. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Kuji, N.; Notake, F.; Tsukamoto, T.; Sasaki, T.; Shimizu, M.; Mukaida, K.; Ito, H.; Isaka, K.; Nishi, H. Ultrasound elastography can detect placental tissue abnormalities. Radiol. Oncol. 2018, 52, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Cimsit, C.; Yoldemir, T.; Akpinar, I.N. Strain elastography in placental dysfunction: Placental elasticity differences in normal and preeclamptic pregnancies in the second trimester. Arch. Gynecol. Obs. 2015, 291, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Ertekin, E.; Tunçyürek, Ö.; Kafkas, S.; Özsunar, Y. Does Placent. Strain Ratio Correl. Umbilical Artery Doppler Values? Clin. Exp. Obstet. Gynecol. 2019, 46, 227–230. [Google Scholar] [CrossRef]
- Akbas, M.; Koyuncu, F.M.; Artunç-Ulkumen, B. Placental elasticity assessment by point shear wave elastography in pregnancies with intrauterine growth restriction. J. Perinat. Med. 2019, 47, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Anuk, A.T.; Tanacan, A.; Erol, S.A.; Alkan, M.; Altinboga, O.; Celen, S.; Keskin, H.L.; Sahin, D. Value of shear-wave elastography and cerebral-placental-uterine ratio in women diagnosed with preeclampsia and fetal growth restriction in prediction of adverse perinatal outcomes. J. Matern. Fetal Neonatal Med. 2022, 35, 10001–10009. [Google Scholar] [CrossRef] [PubMed]
- Arioz Habibi, H.; Alici Davutoglu, E.; Kandemirli, S.G.; Aslan, M.; Ozel, A.; Kalyoncu Ucar, A.; Zeytun, P.; Madazli, R.; Adaletli, I. In vivo assessment of placental elasticity in intrauterine growth restriction by shear-wave elastography. Eur. J. Radiol. 2017, 97, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Deeba, F.; Hu, R.; Lessoway, V.; Terry, J.; Pugash, D.; Hutcheon, J.; Mayer, C.; Salcudean, S.; Rohling, R. SWAVE 2.0 Imaging of Placental Elasticity and Viscosity: Potential Biomarkers for Placenta-Mediated Disease Detection. Ultrasound Med. Biol. 2022, 48, 2486–2501. [Google Scholar] [CrossRef]
- Durhan, G.; Ünverdi, H.; Deveci, C.; Büyükşireci, M.; Karakaya, J.; Değirmenci, T.; Bayrak, A.; Koşar, P.; Hücümenoğlu, S.; Ergün, Y. Placental Elasticity and Histopathological Findings in Normal and Intra-Uterine Growth Restriction Pregnancies Assessed with Strain Elastography in Ex Vivo Placenta. Ultrasound Med. Biol. 2017, 43, 111–118. [Google Scholar] [CrossRef]
- Eroğlu, H.; Tolunay, H.E.; Tonyalı, N.V.; Orgul, G.; Şahin, D.; Yücel, A. Comparison of placental elasticity in normal and intrauterine growth retardation pregnancies by ex vivo strain elastography. Arch. Gynecol. Obs. 2020, 302, 109–115. [Google Scholar] [CrossRef]
- Ohmaru, T.; Fujita, Y.; Sugitani, M.; Shimokawa, M.; Fukushima, K.; Kato, K. Placental elasticity evaluation using virtual touch tissue quantification during pregnancy. Placenta 2015, 36, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.N.; Dai, Y.; Yap, C.H. A Review of Biomechanics Analysis of the Umbilical-Placenta System With Regards to Diseases. Front. Physiol. 2021, 12, 587635. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.S.; Saw, S.N.; Buist, M.L.; Biswas, A.; Zaini Mattar, C.N.; Yap, C.H. Mechanical testing and non-linear viscoelastic modelling of the human placenta in normal and growth restricted pregnancies. J. Biomech. 2016, 49, 173–184. [Google Scholar] [CrossRef]
- Sugitani, M.; Fujita, Y.; Yumoto, Y.; Fukushima, K.; Takeuchi, T.; Shimokawa, M.; Kato, K. A new method for measurement of placental elasticity: Acoustic radiation force impulse imaging. Placenta 2013, 34, 1009–1013. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Khalil, A.; Sotiriadis, A.; D’Antonio, F.; Da Silva Costa, F.; Odibo, A.; Prefumo, F.; Papageorghiou, A.T.; Salomon, L.J. ISUOG Practice Guidelines: Performance of third-trimester obstetric ultrasound scan. Ultrasound Obs. Gynecol. 2024, 63, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Hadlock, F.P.; Harrist, R.B.; Sharman, R.S.; Deter, R.L.; Park, S.K. Estimation of fetal weight with the use of head, body, and femur measurements—A prospective study. Am. J. Obs. Gynecol. 1985, 151, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.; Cavanagh, E.; Kumar, S.; Clifton, V.L.; Borg, D.J.; Priddle, J.; Wille, M.L.; Drovandi, C.; Fontanarosa, D. Changes in placental elastography in the third trimester—Analysis using a linear mixed effect model. Placenta 2021, 114, 83–89. [Google Scholar] [CrossRef]
- Weiher, M.; Richtering, F.G.; Dörffel, Y.; Müller, H.P. Simplification of 2D shear wave elastography by enlarged SWE box and multiple regions of interest in one acquisition. PLoS ONE 2022, 17, e0273769. [Google Scholar] [CrossRef]
- O’Hara, S.; Zelesco, M.; Rocke, K.; Stevenson, G.; Sun, Z. Reliability Indicators for 2-Dimensional Shear Wave Elastography. J. Ultrasound Med. 2019, 38, 3065–3071. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.; Cavanagh, E.; Kumar, S.; Clifton, V.; Fontanarosa, D. Intra-system reliability assessment of 2-dimensional shear wave elastography. Appl. Sci. 2021, 11, 2992. [Google Scholar] [CrossRef]
- AIUM. Recommended Maximum Scanning Times for Displayed Thermal Index (TI) Values. Available online: https://www.aium.org/resources/official-statements/view/recommended-maximum-scanning-times-for-displayed-thermal-index-(ti)-values (accessed on 4 August 2023).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Lv, Z.; Dong, Y.; Liu, W. Review of shear wave elastography in placental function evaluations. J. Matern. Fetal Neonatal Med. 2023, 36, 2203792. [Google Scholar] [CrossRef]
- Gupta, A.; Immanuel, J.; Ho, V.; Dalal, R.; Symons, P.; Simmons, D. Placental abnormalities in type 1 and type 2 diabetes mellitus: A systematic review and metaanalysis of shear wave elastography. Am. J. Obstet. Gynecol. MFM 2022, 4, 100736. [Google Scholar] [CrossRef] [PubMed]
- Menon, A.; Meena, J.; Manchanda, S.; Singhal, S.; Shivhare, S.; Kumar, S. Role of Placental Vascularization Indices and Shear Wave Elastography in Fetal Growth Restriction. J. Obs. Gynaecol. India 2023, 73, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Parker, K.J.; Ormachea, J.; Hah, Z. Group versus Phase Velocity of Shear Waves in Soft Tissues. Ultrason. Imaging 2018, 40, 343–356. [Google Scholar] [CrossRef]
- Altunkeser, A.; Alkan, E.; Günenç, O.; Tolu, İ.; Körez, M.K. Evaluation of a Healthy Pregnant Placenta with Shear Wave Elastography. Iran. J. Radiol. 2019, 16. [Google Scholar] [CrossRef]
- Meena, R.; Malik, A.; Jain, S.; Batra, A. Placental elastography in second trimester preeclampsia prediction: A prospective study. Ultrasound 2022, 30, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.; Cavanagh, E.; Kumar, S.; Clifton, V.L.; Borg, D.J.; Priddle, J.; Wille, M.L.; Drovandi, C.; Fontanarosa, D. Shear wave velocity measurement of the placenta is not limited by placental location. Placenta 2023, 131, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.; Cavanagh, E.; Kumar, S.; Clifton, V.L.; Borg, D.J.; Priddle, J.; Marie-Luise, W.; Drovandi, C.; Fontanarosa, D. Relationship between placental elastography, maternal pre-pregnancy body mass index and gestational weight gain. Placenta 2022, 121, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.Z.; Zheng, J.; Huang, Z.P.; Xiao, Y.; Song, D.; Zeng, J.; Zheng, H.R.; Zheng, R.Q. Influence of measurement depth on the stiffness assessment of healthy liver with real-time shear wave elastography. Ultrasound Med. Biol. 2014, 40, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Akbas, M.; Koyuncu, F.M.; Artunç-Ülkümen, B.; Akbas, G. The relation between second-trimester placental elasticity and poor obstetric outcomes in low-risk pregnancies. J. Perinat. Med. 2021, 49, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zhu, Y.M.; Zhang, Y.K.; Gui, L.P.; Fan, H.R.; Zhang, Y.; Chen, M. The role of shear wave elastography in the assessment of placentas in healthy pregnancy women during third-trimester: A preliminary study. J. Gynecol. Obs. Hum. Reprod. 2022, 51, 102292. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obs. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | EFW ≥ 10th Centile | EFW < 10th Centile | p-Value | |
|---|---|---|---|---|
| n = 222 | n = 107 | n = 115 | ||
| Gestational age | 35 (32, 36) | 35 (31, 36) | 35 (33, 36) | 0.66 |
| Age | 31 ± 6 | 31 ± 6 | 32 ± 6 | 0.85 |
| Nulliparous | 86 (38.7%) | 32 (29.9%) | 54 (47.0%) | 0.009 |
| Body mass index at recruitment (kg/m2) | 25 (21, 31) | 25 (22, 31) | 25 (21, 30) | 0.10 |
| Mean arterial pressure at recruitment (mmHg) | 82 (77, 88) | 82 (77, 87) | 82 (77, 89) | 0.22 |
| Ethnicity | 0.008 | |||
| Nth and Sth American, Australia, NZ, and Europe | 105 (47.3%) | 52 (48.6%) | 53 (46.1%) | |
| NE, SE Asian, and Oceana 1 | 43 (19.4%) | 14 (13.1%) | 29 (25.2%) | |
| South Asian | 40 (18.0%) | 16 (15.0%) | 24 (20.9%) | |
| African | 29 (13.1%) | 20 (18.7%) | 9 (7.8%) | |
| Middle Eastern | 2 (0.9%) | 2 (1.9%) | 0 (0.0%) | |
| Other or mixed ethnicity | 3 (1.4%) | 3 (2.8%) | 0 (0.0%) | |
| Indigenous | 15 (6.8%) | 8 (7.5%) | 7 (6.1%) | 0.43 |
| Spontaneous conception | 205 (92.3%) | 101 (94.4%) | 104 (90.4%) | 0.16 |
| Smoking during pregnancy | 21 (9.5%) | 7 (6.5%) | 14 (12.2%) | 0.15 |
| Alcohol during pregnancy | 3 (1.4%) | 1 (0.9%) | 2 (1.7%) | 0.60 |
| History of SGA baby | 73 (32.9%) | 36 (33.6%) | 37 (32.2%) | 0.82 |
| Connective tissue disease in pregnancy | 4 (1.8%) | 2 (1.9%) | 2 (1.7%) | 0.94 |
| Renal disease in pregnancy | 3 (1.4%) | 2 (1.9%) | 1 (0.9%) | 0.52 |
| Diabetes in pregnancy | 65 (29.3%) | 30 (28.0%) | 35 (30.4%) | 0.69 |
| Hypertension in current pregnancy | 43 (19.4%) | 18 (16.8%) | 25 (21.7%) | 0.35 |
| Pre-eclampsia in current pregnancy | 36 (16.2%) | 9 (8.4%) | 27 (23.5%) | 0.002 |
| Low-dose aspirin use | 62 (27.9%) | 38 (35.5%) | 24 (20.9%) | 0.015 |
| Ultrasonographic Parameters | ||||
| Mean shear wave velocity—SWV (m/s) 2 | 1.30 (1.21, 1.41) | 1.33 (1.24, 1.41) | 1.27 (1.20, 1.40) | 0.05 |
| Standard deviation of SWV (m/s) 2 | 0.12 (0.11, 0.15) | 0.12 (0.11, 0.14) | 0.12 (0.10, 0.15) | 0.70 |
| Average depth (cm) 2 | 4.49 (3.75, 5.30) | 4.53 (3.73, 5.42) | 4.46 (3.90, 5.18) | 0.59 |
| Umbilical artery EDF 2 | 0.008 | |||
| Positive EDF | 300 (97.1%) | 158 (100.0%) | 142 (94.0%) | |
| Absent EDF | 6 (1.9%) | 0 (0.0%) | 6 (4.0%) | |
| Reversed EDF | 3 (1.0%) | 0 (0.0%) | 3 (2.0%) | |
| Umbilical artery pulsatility index 2 | 0.98 (0.85, 1.11) | 0.97 (0.86, 1.10) | 1.00 (0.85, 1.14) | 0.15 |
| Estimated fetal weight 2 | 1808 (1223, 2347) | 2003 (1212, 2582) | 1707.50 (1231, 2206) | <0.001 |
| Model | Univariable OR (95% CI) | p-Value | Multivariable a OR (95% CI) | p-Value | |
|---|---|---|---|---|---|
| 1 | MoM SWV b Quartiles | ||||
| 1 (Lowest) | referent | referent | |||
| 2 | 1.07 (0.59, 1.96) | 0.82 | 1.06 (0.58, 1.94) | 0.85 | |
| 3 | 0.77 (0.42, 1.39) | 0.38 | 0.78 (0.43, 1.43) | 0.43 | |
| 4 | 0.64 (0.34, 1.22) | 0.18 | 0.67 (0.35, 1.29) | 0.23 | |
| 2 | MoM SWV b Deciles | ||||
| 1 (Lowest) | referent | referent | |||
| 2 | 1.50 (0.52, 4.31) | 0.45 | 1.50 (0.53, 4.27) | 0.44 | |
| 3 | 1.50 (0.55, 4.08) | 0.43 | 1.45 (0.53, 3.94) | 0.47 | |
| 4 | 1.36 (0.51, 3.62) | 0.54 | 1.41 (0.52, 3.79) | 0.50 | |
| 5 | 1.00 (0.35, 2.82) | 1.00 | 1.00 (0.36, 2.77) | 0.99 | |
| 6 | 1.05 (0.41, 2.68) | 0.92 | 1.06 (0.42, 2.71) | 0.90 | |
| 7 | 1.20 (0.45, 3.23) | 0.72 | 1.25 (0.46, 3.42) | 0.66 | |
| 8 | 0.60 (0.22, 1.61) | 0.31 | 0.62 (0.23, 1.66) | 0.35 | |
| 9 | 0.79 (0.3, 2.08) | 0.63 | 0.84 (0.32, 2.24) | 0.73 | |
| 10 | 0.74 (0.27, 2.03) | 0.56 | 0.77 (0.28, 2.11) | 0.61 | |
| 3 | MoM SWV b Highest Quartile | ||||
| Quartiles 1–3 | referent | referent | |||
| Highest Quartile | 0.69 (0.41, 1.17) | 0.17 | 0.73 (0.43, 1.23) | 0.24 | |
| 4 | MoM SWV b Highest Decile | ||||
| Deciles 1–9 | referent | referent | |||
| Highest Decile | 0.69 (0.32, 1.48) | 0.34 | 0.71 (0.33, 1.52) | 0.38 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavanagh, E.; Crawford, K.; Hong, J.G.S.; Fontanarosa, D.; Edwards, C.; Wille, M.-L.; Hong, J.; Clifton, V.L.; Kumar, S. The Relationship between Placental Shear Wave Elastography and Fetal Weight—A Prospective Study. J. Clin. Med. 2024, 13, 4432. https://doi.org/10.3390/jcm13154432
Cavanagh E, Crawford K, Hong JGS, Fontanarosa D, Edwards C, Wille M-L, Hong J, Clifton VL, Kumar S. The Relationship between Placental Shear Wave Elastography and Fetal Weight—A Prospective Study. Journal of Clinical Medicine. 2024; 13(15):4432. https://doi.org/10.3390/jcm13154432
Chicago/Turabian StyleCavanagh, Erika, Kylie Crawford, Jesrine Gek Shan Hong, Davide Fontanarosa, Christopher Edwards, Marie-Luise Wille, Jennifer Hong, Vicki L. Clifton, and Sailesh Kumar. 2024. "The Relationship between Placental Shear Wave Elastography and Fetal Weight—A Prospective Study" Journal of Clinical Medicine 13, no. 15: 4432. https://doi.org/10.3390/jcm13154432
APA StyleCavanagh, E., Crawford, K., Hong, J. G. S., Fontanarosa, D., Edwards, C., Wille, M.-L., Hong, J., Clifton, V. L., & Kumar, S. (2024). The Relationship between Placental Shear Wave Elastography and Fetal Weight—A Prospective Study. Journal of Clinical Medicine, 13(15), 4432. https://doi.org/10.3390/jcm13154432