
The Use of National Cancer Registry Data for Breast Cancer Family History Assessment in Premenopausal Women



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cancer Registry Data
2.3. Assessing BC/OC Risk Score
2.4. Statistical Analysis
3. Results
3.1. Personal History of Cancer in the Study Population
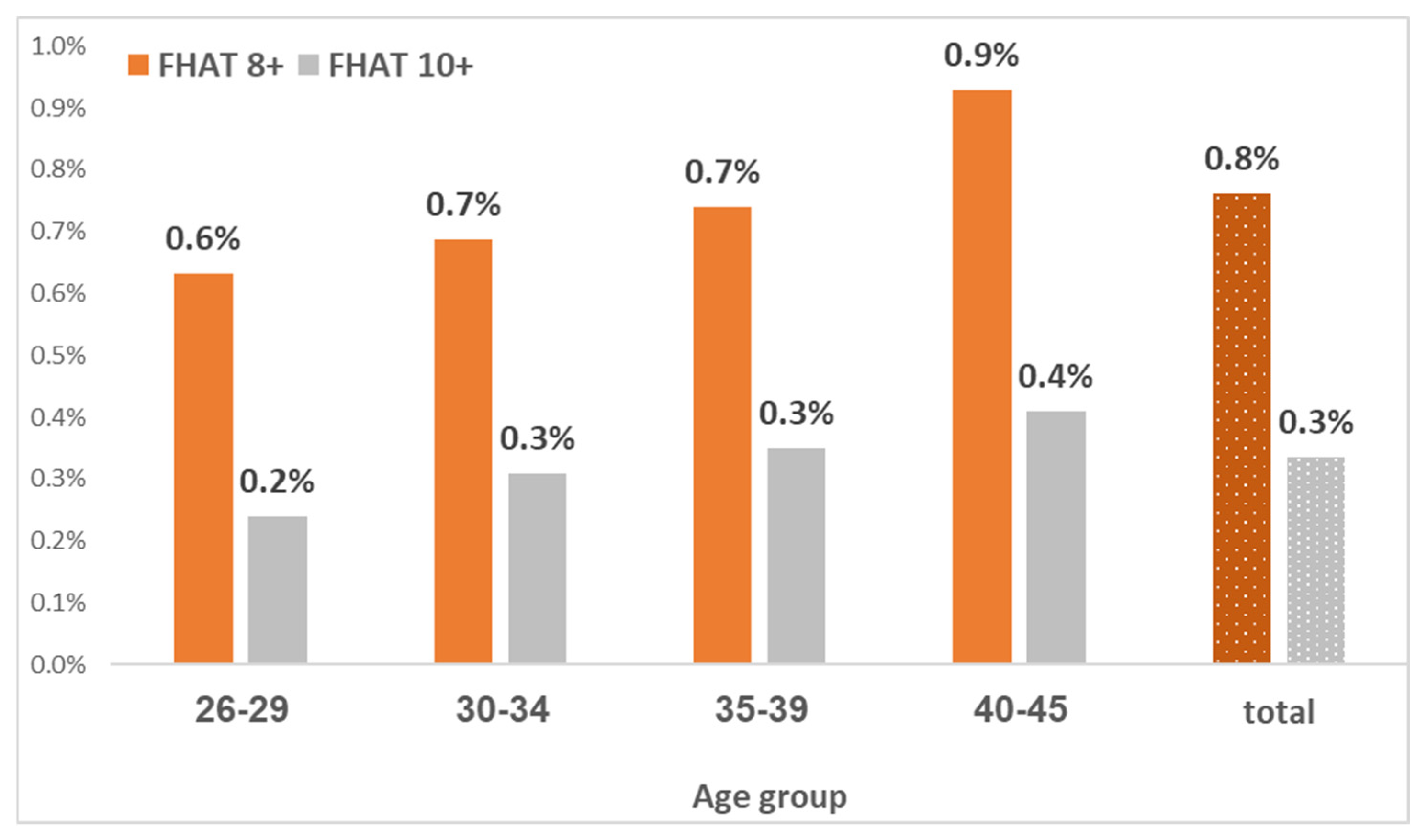
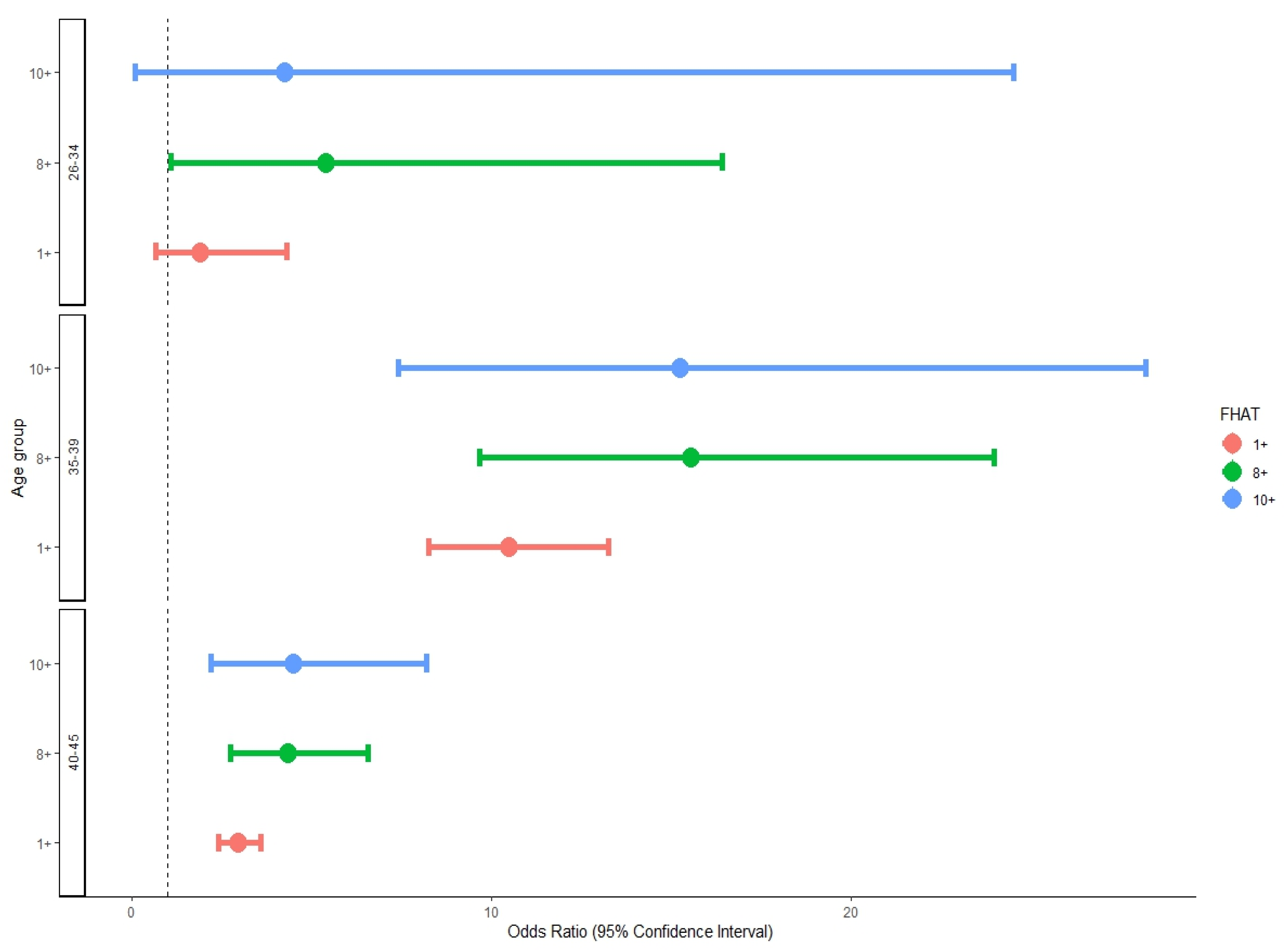
3.2. FHAT Score and Risk of BC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Israeli Ministy of Health. Ministry of Health’s Data on Breast Cancer in Israel for the Year 2020. 2023. Available online: https://www.gov.il/en/pages/01102023-01 (accessed on 30 July 2024).
- Everatt, R.; Intaitė, B. Trends in Mortality Rates of Corpus Uteri and Ovarian Cancer in Lithuania, 1987–2016. Medicina 2020, 56, 347. [Google Scholar] [CrossRef] [PubMed]
- King, M.-C.; Marks, J.H.; Mandell, J.B. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science 2003, 302, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Struewing, J.P.; Hartge, P.; Wacholder, S.; Baker, S.M.; Berlin, M.; McAdams, M.; Timmerman, M.M.; Brody, L.C.; Tucker, M.A. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N. Engl. J. Med. 1997, 336, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; Jervis, S.; Van Leeuwen, F.E.; Milne, R.L.; Andrieu, N. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Sarig, K.; Oxley, S.; Kalra, A.; Sobocan, M.; Fierheller, C.T.; Sideris, M.; Gootzen, T.; Ferris, M.; Eeles, R.A.; Evans, D.G. BRCA awareness and testing experience in the UK Jewish population: A qualitative study. J. Med. Genet. 2024, 61, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, R.; Aharonov-Majar, E.; Isakov, O.; Hayek, S.; Elefant, N.; Balicer, R.D.; Senderey, A.B.; Ben-Shachar, S. Carrier screening program for BRCA1/BRCA2 pathogenic variants among Ashkenazi Jewish women in Israel: An observational study. Genet. Med. Open 2023, 1, 100824. [Google Scholar] [CrossRef]
- Del Fiol, G.; Kohlmann, W.; Bradshaw, R.L.; Weir, C.R.; Flynn, M.; Hess, R.; Schiffman, J.D.; Nanjo, C.; Kawamoto, K. Standards-based clinical decision support platform to manage patients who meet guideline-based criteria for genetic evaluation of familial cancer. JCO Clin. Cancer Inform. 2020, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.E.; Rehman, H.T.; Bedrosian, I. Importance of family history and indications for genetic testing. Breast J. 2020, 26, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Endevelt, R.; Goren, I.; Sela, T.; Shalev, V. Family history intake: A challenge to personalized approaches in health promotion and disease prevention. Isr. J. Health Policy Res. 2015, 4, 60. [Google Scholar] [CrossRef]
- Mai, P.L.; Garceau, A.O.; Graubard, B.I.; Dunn, M.; McNeel, T.S.; Gonsalves, L.; Gail, M.H.; Greene, M.H.; Willis, G.B.; Wideroff, L. Confirmation of family cancer history reported in a population-based survey. J. Natl. Cancer Inst. 2011, 103, 788–797. [Google Scholar] [CrossRef]
- Daly, M.B.; Rosenthal, E.; Cummings, S.; Bernhisel, R.; Kidd, J.; Hughes, E.; Gutin, A.; Meek, S.; Slavin, T.P.; Kurian, A.W. The association between age at breast cancer diagnosis and prevalence of pathogenic variants. Breast Cancer Res. Treat. 2023, 199, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Silverman, B.G.; Fishler, Y.; Ben-Adiva, E.; Davidov, O.; Dichtiar, R.; Edri, H.; Zatlawi, M.; Keinan-Boker, L. An assessment of the completeness and timeliness of the Israel national cancer registry. Isr. Med. Assoc. J. 2021, 23, 23–27. [Google Scholar] [PubMed]
- Gilpin, C.; Carson, N.; Hunter, A. A preliminary validation of a family history assessment form to select women at risk for breast or ovarian cancer for referral to a genetics center. Clin. Genet. 2000, 58, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Parmigiani, G.; Chen, S.; Iversen, E.S., Jr.; Friebel, T.M.; Finkelstein, D.M.; Anton-Culver, H.; Ziogas, A.; Weber, B.L.; Eisen, A.; Malone, K.E. Validity of Models for Predicting BRCA1 and BRCA2 Mutations. Ann. Intern. Med. 2007, 147, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Allweis, T.M.; Hermann, N.; Berenstein-Molho, R.; Guindy, M. Personalized Screening for Breast Cancer: Rationale, Present Practices, and Future Directions. Ann. Surg. Oncol. 2021, 28, 4306–4317. [Google Scholar] [CrossRef] [PubMed]
- Keinan-Boker, L.; Baron-Epel, O.; Garty, N.; Green, M.S. Family history of breast cancer and compliance with mammography in Israel: Findings of the National Health Survey 2003–2004 (EUROHIS). Eur. J. Cancer Prev. 2007, 16, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Manchanda, R.; Burnell, M.; Gaba, F.; Desai, R.; Wardle, J.; Gessler, S.; Side, L.; Sanderson, S.; Loggenberg, K.; Brady, A.F. Randomised trial of population-based BRCA testing in Ashkenazi Jews: Long-term outcomes. BJOG Int. J. Obstet. Gynaecol. 2020, 127, 364–375. [Google Scholar] [CrossRef]
- Childers, C.P.; Childers, K.K.; Maggard-Gibbons, M.; Macinko, J. National Estimates of Genetic Testing in Women With a History of Breast or Ovarian Cancer. J. Clin. Oncol. 2017, 35, 3800–3806. [Google Scholar] [CrossRef]
- Manchanda, R.; Blyuss, O.; Gaba, F.; Gordeev, V.S.; Jacobs, C.; Burnell, M.; Gan, C.; Taylor, R.; Turnbull, C.; Legood, R. Current detection rates and time-to-detection of all identifiable BRCA carriers in the Greater London population. J. Med. Genet. 2018, 55, 538–545. [Google Scholar] [CrossRef]
- Gabai-Kapara, E.; Lahad, A.; Kaufman, B.; Friedman, E.; Segev, S.; Renbaum, P.; Beeri, R.; Gal, M.; Grinshpun-Cohen, J.; Djemal, K. Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2. Proc. Natl. Acad. Sci. USA 2014, 111, 14205–14210. [Google Scholar] [CrossRef]
- Manchanda, R.; Loggenberg, K.; Sanderson, S.; Burnell, M.; Wardle, J.; Gessler, S.; Side, L.; Balogun, N.; Desai, R.; Kumar, A. Population Testing for Cancer Predisposing BRCA1/BRCA2 Mutations in the Ashkenazi-Jewish Community: A Randomized Controlled Trial. JNCI J. Natl. Cancer Inst. 2014, 107, dju379. [Google Scholar] [CrossRef] [PubMed]
- Michaelson-Cohen, R.; Cohen, M.J.; Cohen, C.; Greenberg, D.; Shmueli, A.; Lieberman, S.; Tomer, A.; Levy-Lahad, E.; Lahad, A. Real World Cost-Effectiveness Analysis of Population Screening for BRCA Variants among Ashkenazi Jews Compared with Family History-Based Strategies. Cancers 2022, 14, 6113. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| 26–34 y | 35–39 y | 40–45 y | Total | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Total | 182 | 100% | 348 | 100% | 910 | 100% | 1440 | 100% |
| Breast | 88 | 48.4% | 243 | 69.8% | 699 | 76.8% | 1030 | 71.5% |
| Ovary | 52 | 28.6% | 55 | 15.8% | 113 | 12.4% | 220 | 15.3% |
| Colon | 19 | 10.4% | 19 | 5.5% | 50 | 5.5% | 88 | 6.1% |
| Stomach, intestines, rectum | 13 | 7.1% | 10 | 2.9% | 22 | 2.4% | 45 | 3.1% |
| Pancreas | 2 | 1.1% | 8 | 2.3% | 13 | 1.4% | 23 | 1.6% |
| Digestive organs, uns. | 4 | 2.2% | 4 | 1.1% | 2 | 0.2% | 10 | 0.7% |
| Lymphoma | 1 | 0.5% | 1 | 0.3% | 3 | 0.3% | 5 | 0.3% |
| Reticulosarcoma | 0 | 0.0% | 2 | 0.6% | 2 | 0.2% | 4 | 0.3% |
| Oral cavity | 1 | 0.5% | 0 | 0.0% | 3 | 0.3% | 4 | 0.3% |
| Carcinoid | 1 | 0.5% | 1 | 0.3% | 2 | 0.2% | 4 | 0.3% |
| Hepatic flexure | 0 | 0.0% | 2 | 0.6% | 1 | 0.1% | 3 | 0.2% |
| Skin of trunk, in situ | 0 | 0.0% | 2 | 0.6% | 0 | 0.0% | 2 | 0.1% |
| Female genital organs | 1 | 0.5% | 1 | 0.3% | 0 | 0.0% | 2 | 0.1% |
| None | Breast Cancer | Ovarian Cancer | Either | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | % | % | % | ||||
| Age 40–45 | ||||||||
| FHAT 10+ | 434 | 0.40% | 11 | 1.60% | 1 | 0.90% | 12 | 1.50% |
| FHAT 8+ | 984 | 0.90% | 24 | 3.50% | 2 | 1.90% | 26 | 3.30% |
| FHAT 1+ | 7758 | 7.20% | 129 | 18.60% | 8 | 7.50% | 137 | 17.10% |
| FHAT = 0 | 100,112 | 92.80% | 563 | 81.40% | 99 | 92.50% | 662 | 82.90% |
| Total | 107,898 | 100% | 692 | 100% | 107 | 100% | 799 | 100% |
| Age 35–39 | ||||||||
| FHAT 10+ | 328 | 0.30% | 11 | 4.50% | 1 | 1.80% | 12 | 4.00% |
| FHAT 8+ | 701 | 0.70% | 24 | 9.90% | 2 | 3.60% | 17 | 5.70% |
| FHAT 1+ | 5440 | 5.60% | 41 | 16.90% | 8 | 14.50% | 47 | 15.80% |
| FHAT = 0 | 91,289 | 94.40% | 201 | 83.10% | 49 | 89.10% | 250 | 84.20% |
| Total | 96,729 | 100% | 242 | 100% | 55 | 100% | 297 | 100% |
| Age 26–34 | ||||||||
| FHAT 10+ | 485 | 0.3% | 1 | 1.1% | 0 | 0.0% | 1 | 0.7% |
| FHAT 8+ | 1145 | 0.7% | 3 | 3.4% | 0 | 0.0% | 3 | 2.2% |
| FHAT 1+ | 7002 | 4.1% | 7 | 8.0% | 1 | 2.0% | 8 | 5.8% |
| FHAT = 0 | 165,103 | 95.9% | 80 | 92.0% | 49 | 98.0% | 129 | 94.2% |
| Total | 172,105 | 100% | 87 | 100% | 50 | 100% | 137 | 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chodick, G.; Silverman, B.G.; Keinan-Boker, L. The Use of National Cancer Registry Data for Breast Cancer Family History Assessment in Premenopausal Women. J. Clin. Med. 2024, 13, 4473. https://doi.org/10.3390/jcm13154473
Chodick G, Silverman BG, Keinan-Boker L. The Use of National Cancer Registry Data for Breast Cancer Family History Assessment in Premenopausal Women. Journal of Clinical Medicine. 2024; 13(15):4473. https://doi.org/10.3390/jcm13154473
Chicago/Turabian StyleChodick, Gabriel, Barbara G. Silverman, and Lital Keinan-Boker. 2024. "The Use of National Cancer Registry Data for Breast Cancer Family History Assessment in Premenopausal Women" Journal of Clinical Medicine 13, no. 15: 4473. https://doi.org/10.3390/jcm13154473
APA StyleChodick, G., Silverman, B. G., & Keinan-Boker, L. (2024). The Use of National Cancer Registry Data for Breast Cancer Family History Assessment in Premenopausal Women. Journal of Clinical Medicine, 13(15), 4473. https://doi.org/10.3390/jcm13154473