
The Long-Term, Real-World Effects of Oxybutynin on Pressure Reservoir Function in the Neurogenic Bladder after Spinal Cord Injury: A Retrospective Cohort Study
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Setting
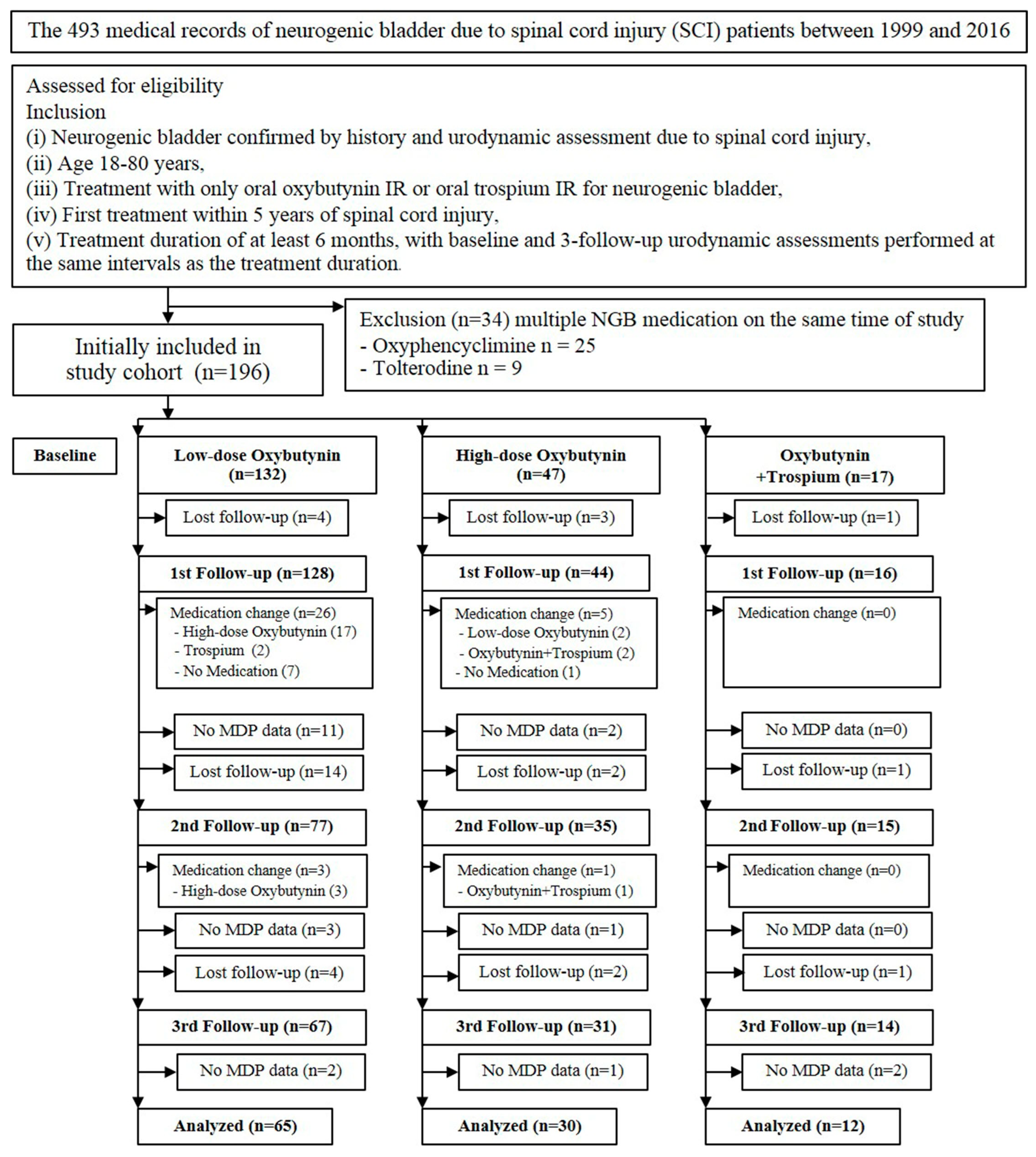
2.2. Patient Population
2.3. Urodynamic Study
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Spinal Cord Injury Statistical Center. Spinal cord injury facts and figures at a glance. J. Spinal Cord Med. 2013, 36, 1–2. [Google Scholar] [CrossRef]
- Cripps, R.A.; Lee, B.B.; Wing, P.; Weerts, E.; Mackay, J.; Brown, D. A global map for traumatic spinal cord injury epidemiology: Towards a living data repository for injury prevention. Spinal Cord 2011, 49, 493–501. [Google Scholar] [CrossRef]
- Lee, B.B.; Cripps, R.A.; Fitzharris, M.; Wing, P.C. The global map for traumatic spinal cord injury epidemiology: Update 2011, global incidence rate. Spinal Cord 2014, 52, 110–116. [Google Scholar] [CrossRef]
- Kovindha, A. People with Spinal Cord Injury in Thailand. Am. J. Phys. Med. Rehabil. 2017, 96, S120–S123. [Google Scholar] [CrossRef]
- Przydacz, M.; Denys, P.; Corcos, J. What do we know about neurogenic bladder prevalence and management in developing countries and emerging regions of the world? Ann. Phys. Rehabil. Med. 2017, 60, 341–346. [Google Scholar] [CrossRef]
- Dorsher, P.T.; McIntosh, P.M. Neurogenic bladder. Adv. Urol. 2012, 2012, 816274. [Google Scholar] [CrossRef]
- Manack, A.; Motsko, S.P.; Haag-Molkenteller, C.; Dmochowski, R.R.; Goehring, E.L., Jr.; Nguyen-Khoa, B.A.; Jones, J.K. Epidemiology and healthcare utilization of neurogenic bladder patients in a US claims database. Neurourol. Urodyn. 2011, 30, 395–401. [Google Scholar] [CrossRef]
- Simpson, L.A.; Eng, J.J.; Hsieh, J.T.; Wolfe, D.L.; Spinal Cord Injury Rehabilitation Evidence (SCIRE) Research Team. The health and life priorities of individuals with spinal cord injury: A systematic review. J. Neurotrauma 2012, 29, 1548–1555. [Google Scholar] [CrossRef]
- Agrawal, M.; Joshi, M. Urodynamic patterns after traumatic spinal cord injury. J. Spinal Cord Med. 2015, 38, 128–133. [Google Scholar] [CrossRef]
- Erol, B.; Kocak, T.; Kadioglu, A.; Muslumanoglu, L.; Karamehmetoglu, S.; Akinci, M.; Arikan, F. The relationship between level of injury and bladder behavior in patients with post-traumatic spinal cord injury. Ulus. Travma Acil. Cerrahi Derg. 2009, 15, 377–382. [Google Scholar]
- Weld, K.J.; Dmochowski, R.R. Association of level of injury and bladder behavior in patients with post-traumatic spinal cord injury. Urology 2000, 55, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.C.; Park, C.I.; Kim, H.J.; Lee, I.Y. Significance of low compliance bladder in cauda equina injury. Spinal Cord 2002, 40, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Consortium for Spinal Cord Medicine. Bladder management for adults with spinal cord injury: A clinical practice guideline for health-care providers. J. Spinal Cord Med. 2006, 29, 527–573. [Google Scholar]
- Amarenco, G.; Sheikh Ismael, S.; Chesnel, C.; Charlanes, A.; Breton, F.L.E. Diagnosis and clinical evaluation of neurogenic bladder. Eur. J. Phys. Rehabil. Med. 2017, 53, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Samson, G.; Cardenas, D.D. Neurogenic bladder in spinal cord injury. Phys. Med. Rehabil. Clin. N. Am. 2007, 18, 255–274. [Google Scholar] [CrossRef] [PubMed]
- Taweel, W.A.; Seyam, R. Neurogenic bladder in spinal cord injury patients. Res. Rep. Urol. 2015, 7, 85–99. [Google Scholar] [CrossRef] [PubMed]
- Erdem, N.; Chu, F.M. Management of overactive bladder and urge urinary incontinence in the elderly patient. Am. J. Med. 2006, 119, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Stohrer, M.; Blok, B.; Castro-Diaz, D.; Chartier-Kastler, E.; Del Popolo, G.; Kramer, G.; Pannek, J.; Radziszewski, P.; Wyndaele, J.J. EAU guidelines on neurogenic lower urinary tract dysfunction. Eur. Urol. 2009, 56, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.; Hilas, O. Pharmacologic management of overactive bladder. Clin. Interv. Aging 2007, 2, 337–345. [Google Scholar] [PubMed]
- Andersson, K.E.; Chapple, C.R. Oxybutynin and the overactive bladder. World J. Urol. 2001, 19, 319–323. [Google Scholar] [CrossRef]
- Chapple, C. New once-daily formulation for trospium in overactive bladder. Int. J. Clin. Pract. 2010, 64, 1535–1540. [Google Scholar] [CrossRef]
- Diokno, A.; Sand, P.; Labasky, R.; Sieber, P.; Antoci, J.; Leach, G.; Atkinson, L.; Albrecht, D. Long-term safety of extended-release oxybutynin chloride in a community-dwelling population of participants with overactive bladder: A one-year study. Int. Urol. Nephrol. 2002, 34, 43–49. [Google Scholar] [CrossRef]
- Sonoda, T.; Sakurai, T.; Yamada, K.; Mizutani, S.; Tsujimoto, Y.; Ogawa, T. Effects of long-term administration of oxybutynin hydrochloride (KL007) for the treatment of neurogenic bladder and unstable bladder. Hinyokika Kiyo 1989, 35, 167–178. [Google Scholar] [PubMed]
- Comperat, E.; Reitz, A.; Delcourt, A.; Capron, F.; Denys, P.; Chartier-Kastler, E. Histologic features in the urinary bladder wall affected from neurogenic overactivity—A comparison of inflammation, oedema and fibrosis with and without injection of botulinum toxin type A. Eur. Urol. 2006, 50, 1058–1064. [Google Scholar] [CrossRef] [PubMed]
- Sirasaporn, P.; Saengsuwan, J. Incidence and predictive factors for developing vesicoureteric reflux in individuals with suprasarcral spinal cord injury: A historical cohort study. Spinal Cord 2021, 59, 753–760. [Google Scholar] [CrossRef]
- Rupp, R.; Biering-Sorensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey-Md, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Pannek, J.; Kennelly, M.; Kessler, T.M.; Linsenmeyer, T.; Wyndaele, J.J.; Biering-Sorensen, F. International spinal cord injury urodynamic basic data set (version 2.0). Spinal Cord Ser. Cases 2018, 4, 98. [Google Scholar] [CrossRef]
- Musco, S.; Padilla-Fernandez, B.; Del Popolo, G.; Bonifazi, M.; Blok, B.F.M.; Groen, J.; Hoen, L.; Pannek, J.; Bonzon, J.; Kessler, T.M.; et al. Value of urodynamic findings in predicting upper urinary tract damage in neuro-urological patients: A systematic review. Neurourol. Urodyn. 2018, 37, 1522–1540. [Google Scholar] [CrossRef]
- Madersbacher, H.; Stohrer, M.; Richter, R.; Burgdorfer, H.; Hachen, H.J.; Murtz, G. Trospium chloride versus oxybutynin: A randomized, double-blind, multicentre trial in the treatment of detrusor hyper-reflexia. Br. J. Urol. 1995, 75, 452–456. [Google Scholar] [CrossRef]
- Hadiji, N.; Previnaire, J.G.; Benbouzid, R.; Robain, G.; Leblond, C.; Mieusset, R.; Enjalbert, M.; Soler, J.M. Are oxybutynin and trospium efficacious in the treatment of detrusor overactivity in spinal cord injury patients? Spinal Cord 2014, 52, 701–705. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Lo, S.-H.; Meng, E.; Shen, J.-D.; Chou, E.C.-L.; Chen, S.-F.; Lee, M.-H.; Hsu, C.-Y.; Ong, H.-L.; Chen, J.-T.; et al. Clinical Guidelines of Patient-centered Bladder Management of Neurogenic Lower Urinary Tract Dysfunction due to Chronic Spinal Cord Injury-Part 1: Pathophysiology, Treatment Strategy, and Priority. Urol. Sci. 2023, 34, 3–9. [Google Scholar]
- Van Kerrebroeck, P.E.; Amarenco, G.; Thuroff, J.W.; Madersbacher, H.G.; Lock, M.T.; Messelink, E.J.; Soler, J.M. Dose-ranging study of tolterodine in patients with detrusor hyperreflexia. Neurourol. Urodyn. 1998, 17, 499–512. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Mean or % Variable | Low-Dose | High-Dose | Oxybutynin + Trospium |
|---|---|---|---|
| Number of patients | 65 | 30 | 12 |
| Age at diagnosis, years | 44.9 ± 14.9 | 41.3 ± 13.8 | 33.0 ± 13.8 |
| Sex: women/men (%) | 35.4/64.6 | 36.7/63.3 | 41.7/58.3 |
| Duration after SCI, years | 1.2 ± 1.1 | 1.7 ± 1.5 | 1.2 ± 1.1 |
| Duration of treatment, years | 2.8 ± 0.8 | 2.8 ± 0.9 | 2.9 ± 0.9 |
| Suprasacral injury (%) | 89.2 | 90 | 100 |
| Complete injury (%) | 29.2 | 50.0 | 41.7 |
| Indwelling urinary catheter (%) | 41.5 | 33.3 | 25 |
| Baseline values | |||
| MDP (cmH2O) | 44.5 ± 21.8 | 57.9 ± 28.5 | 62.8 ± 25.0 |
| CBC (mL) | 253.4 ± 125.6 | 247.8 ± 116.9 | 278.2 ± 176.9 |
| MDP (cmH2O) | Low-Dose Oxybutynin | High-Dose Oxybutynin | Oxybutynin + Trospium |
|---|---|---|---|
| n | 65 | 30 | 12 |
| Baseline (BL) | 44.5 ± 21.8 | 57.9 ± 28.5 | 62.8 ± 25.0 |
| Follow-up 1 (FU1) | 35.2 ± 23.2 | 39.9 ± 22.6 | 40.7 ± 30.3 |
| Time from BL toFU1, year | 1.0 ± 0.4 | 0.9 ± 0.3 | 1.1 ± 0.5 |
| Mean difference (95% CI) | −9.5 (−16.6, −2.5) | −18.1 (−28.8, −7.3) | −22.1 (−38.2, −5.9) |
| p-value | 0.008 * | 0.001 * | 0.007 * |
| Adjusted mean difference (95% CI) | −9.4 (−16.5, −2.4) | −18.1 (−28.7, −7.4) | −22.1 (−38.3, −5.8) |
| p-value | 0.009 * | 0.001 * | 0.008 * |
| Follow-up 2 (FU2) | 38.5 ± 19.7 | 43.6 ± 22.1 | 38.6 ± 30.0 |
| Time from FU1 to FU 2, year | 1.1 ± 0.4 | 1.2 ± 0.5 | 1.0 ± 0.5 |
| Mean difference (95% CI) | −6.2 (−13.1, 0.8) | −14.5 (−25.3, −3.6) | −24.2 (−40.3, −8.0) |
| p-value | 0.081 | 0.009 * | 0.003 * |
| Adjusted mean difference (95% CI) | −6.0 (−13.0,0.9) | −14.4 (−25.1,−3.7) | −24.2 (−40.4,−8.0) |
| p-value | 0.089 | 0.009 * | 0.003 * |
| Follow-up 3 (FU3) | 41.8 ± 24.9 | 40.9 ± 22.4 | 40.1 ± 13.1 |
| Time from FU2 to FU3, year | 1.0 ± 0.4 | 1.1 ± 0.4 | 1.0 ± 0.5 |
| Mean difference (95% CI) | −2.0 (−9.8, 5.9) | −17.9 (−30.5, −5.2) | −21.9 (−39.6, −4.2) |
| p-value | 0.628 | 0.006 * | 0.015 * |
| Adjusted mean difference (95% CI) | −2.5 (−10.4, 5.4) | −16.9 (−29.4, −4.4) | −21.9 (−39.8, −4.1) |
| p-value | 0.540 | 0.008 * | 0.016 * |
| Overall changes | |||
| Mean difference (95% CI) | −0.8 (−3.2, 1.7) | −5.4 (−9.4, −1.4) | −7.4 (−13.2, −1.5) |
| p-value | 0.553 | 0.008 * | 0.014 * |
| Adjusted mean difference (95% CI) | −0.9 (−3.4, 1.6) | −5.2 (−9.1, −1.2) | −7.4 (−13.3, −1.5) |
| p-value | 0.492 | 0.011 * | 0.014 * |
| CBC (mL) | Low-Dose Oxybutynin | High-Dose Oxybutynin | Oxybutynin + Trospium |
|---|---|---|---|
| n | 65 | 30 | 12 |
| Baseline | 253.4 ± 125.6 | 247.8 ± 116.9 | 278.2 ± 176.9 |
| Follow-up 1 | 265.5 ± 134.0 | 234.6 ± 122.6 | 267.1 ± 166.8 |
| Mean difference (95% CI) | 10.5 (−27.6, 48.7) | −13.2 (−59.7, 33.3) | −11.1 (−99.4, 77.2) |
| p-value | 0.589 | 0.578 | 0.806 |
| Adjusted mean difference (95% CI) | 10.9 (−27.3, 49.2) | −13.2 (−59.5, 33.1) | −11.1 (−98.1, 75.9) |
| p-value | 0.575 | 0.576 | 0.803 |
| Follow-up 2 | 260.3 ± 135.5 | 213.5 ± 92.0 | 248.0 ± 97.3 |
| Mean difference (95% CI) | 6.1 (−31.3, 43.5) | −34.3 (−81.8, 13.2) | −30.2 (−118.5, 58.2) |
| p-value | 0.749 | 0.157 | 0.503 |
| Adjusted mean difference (95 % CI) | 5.6 (−31.9, 43.1) | −34.0 (−81.4, 13.3) | −30.2 (−117.2, 56.8) |
| p-value | 0.769 | 0.158 | 0.497 |
| Follow-up 3 | 223.7 ± 142.7 | 242.9 ± 140.6 | 270.9 ± 186.2 |
| Mean difference (95% CI) | −29.8 (−72.7, 13.1) | −8.0 (−62.0, 46.1) | −4.2 (−101.2, 92.9) |
| p-value | 0.174 | 0.772 | 0.933 |
| Adjusted mean difference (95% CI) | −29.1 (−72.1, 14.0) | −6.9 (−60.8, 47.0) | −7.8 (−103.8, 88.1) |
| p-value | 0.186 | 0.801 | 0.873 |
| Overall changes | |||
| Mean difference (95% CI) | −7.3 (−20.5, 6.0) | −6.5 (−23.2, 10.2) | −4.5 (−34.8, 25.9) |
| p-value | 0.283 | 0.445 | 0.772 |
| Adjusted mean difference (95% CI) | −7.2 (−20.5, 6.1) | −6.2 (−22.9, 10.4) | −5.5 (−35.5, 24.4) |
| p-value | 0.29 | 0.465 | 0.718 |
| Success Rate (%) | Achievement of Baseline MDP ≤ 40 cmH2O | Achievement of Follow-up 3 MDP ≤ 40 cmH2O |
|---|---|---|
| Low-dose Oxybutynin | 44.6 | 54.8 |
| High-dose Oxybutynin | 36.7 | 66.7 |
| Oxybutynin + Trospium | 16.7 | 66.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boonjaraspinyo, S.; Saengsuwan, J.; Sirasaporn, P.; Thinkhamrop, B. The Long-Term, Real-World Effects of Oxybutynin on Pressure Reservoir Function in the Neurogenic Bladder after Spinal Cord Injury: A Retrospective Cohort Study. J. Clin. Med. 2024, 13, 4514. https://doi.org/10.3390/jcm13154514
Boonjaraspinyo S, Saengsuwan J, Sirasaporn P, Thinkhamrop B. The Long-Term, Real-World Effects of Oxybutynin on Pressure Reservoir Function in the Neurogenic Bladder after Spinal Cord Injury: A Retrospective Cohort Study. Journal of Clinical Medicine. 2024; 13(15):4514. https://doi.org/10.3390/jcm13154514
Chicago/Turabian StyleBoonjaraspinyo, Sirintip, Jittima Saengsuwan, Patpiya Sirasaporn, and Bandit Thinkhamrop. 2024. "The Long-Term, Real-World Effects of Oxybutynin on Pressure Reservoir Function in the Neurogenic Bladder after Spinal Cord Injury: A Retrospective Cohort Study" Journal of Clinical Medicine 13, no. 15: 4514. https://doi.org/10.3390/jcm13154514