

Etiology, Outcomes, and Complications of Total Hip Arthroplasty in Younger Patients: A Nationwide Big Data Analysis


Abstract
1. Introduction
Research Questions
2. Methods
2.1. Data Source
2.2. Study Population and Patient Variables
2.3. Outcome Measures
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
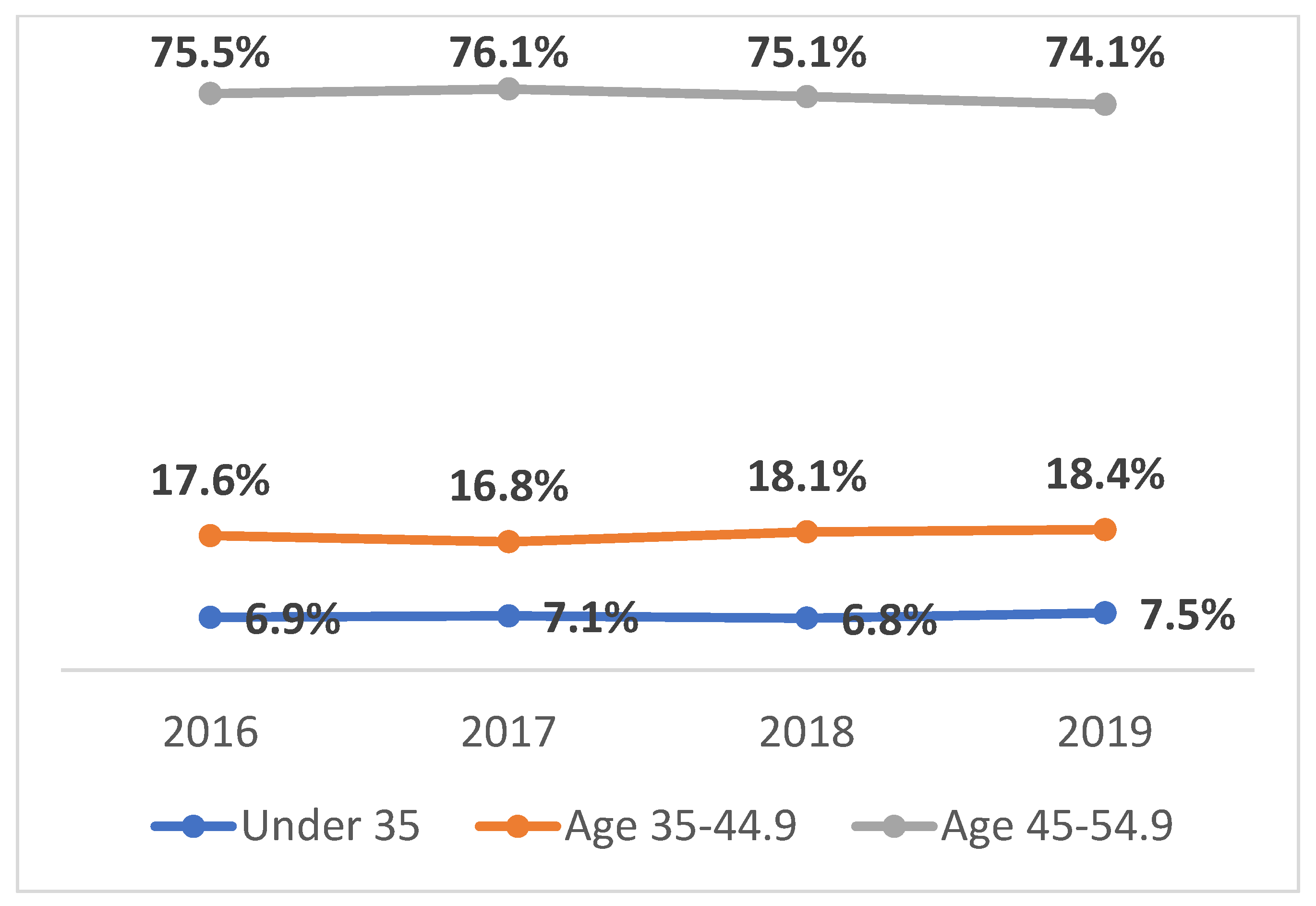
3.1. Proportion of THA Procedures across Age Groups
3.2. Etiologies of THA by Age Group
3.3. Demographics and Clinical Characteristics
3.4. Prevalence of Comorbidities in THA Patients by Age Group
3.5. Hospitalization Outcomes by Age Group
3.6. Postoperative Complications by Age Group
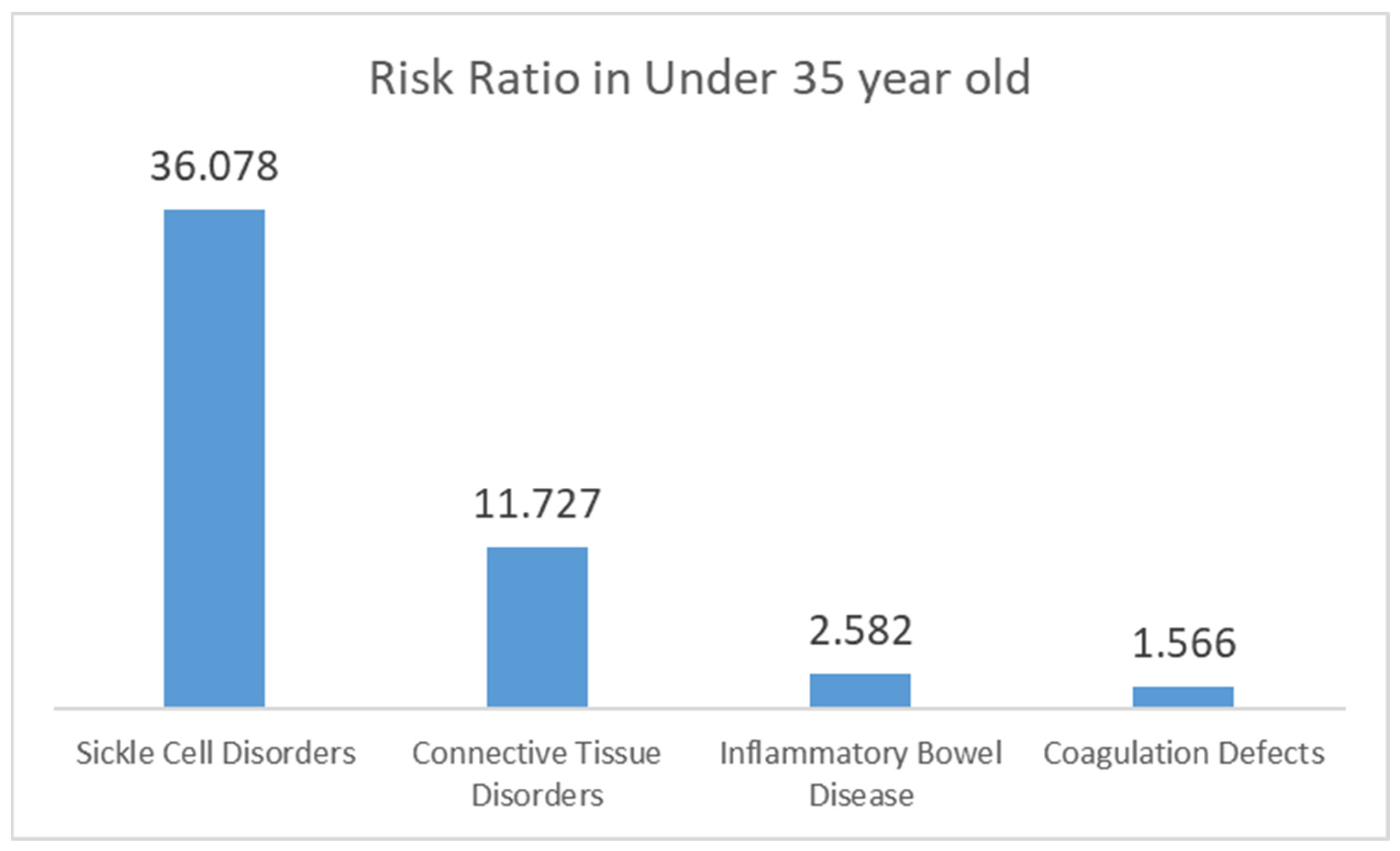
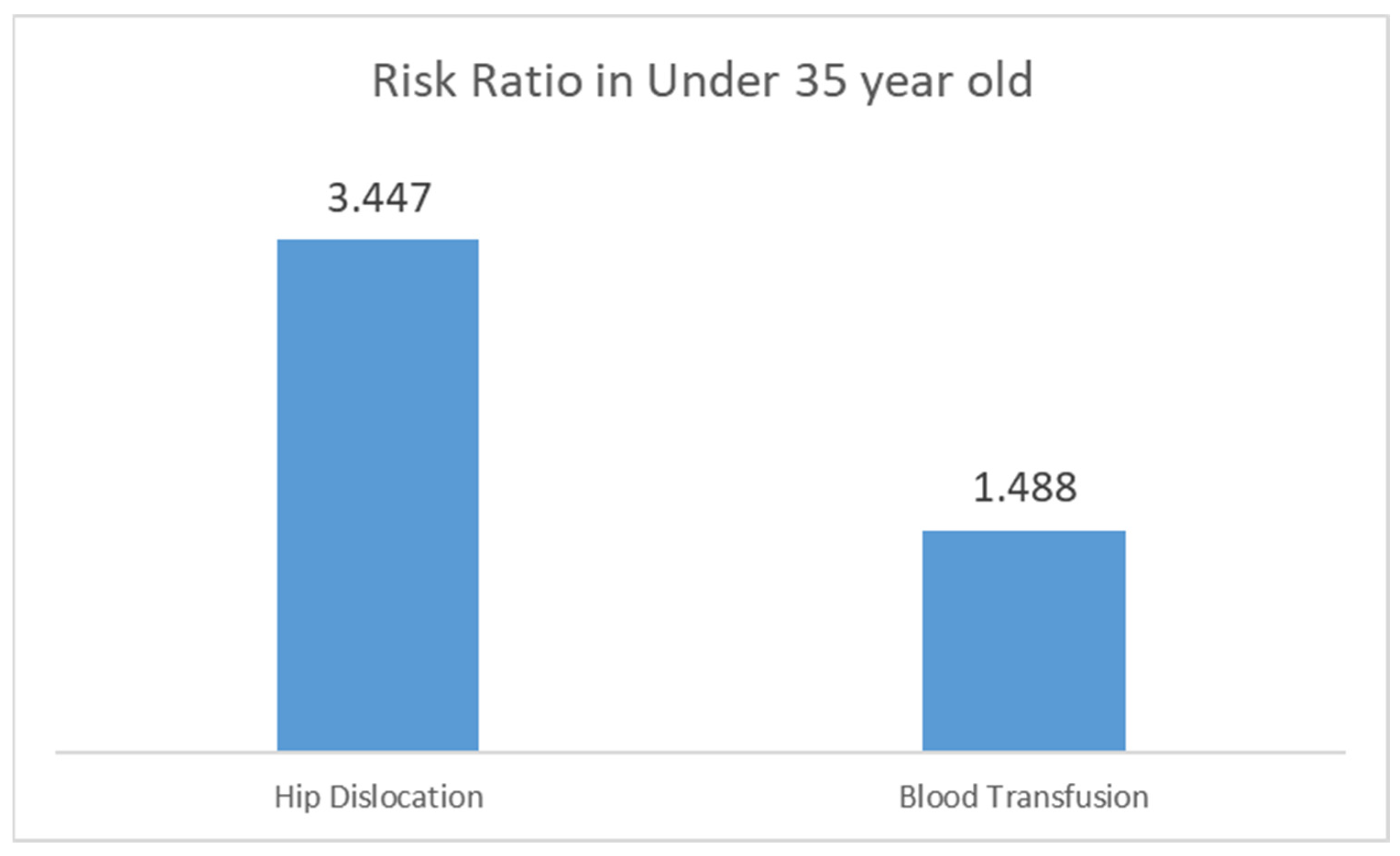
3.7. Risk Estimates of Etiologies, Comorbidities, and Postoperative Complications
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCUP | Healthcare Cost and Utilization Project |
| IBD | Inflammatory bowel disease |
| ICD-10 | International Classification of Diseases, 10th Revision |
| LOS | Length of stay |
| NIS | Nationwide Inpatient Sample |
| SPSS | Statistical Package for the Social Sciences |
| THA | Total hip arthroplasty |
References
- Gademan, M.G.J.; Hofstede, S.N.; Vlieland, T.P.M.V.; Nelissen, R.G.H.H.; De Mheen, P.J.M.-V. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet. Disord. 2016, 17, 463. [Google Scholar] [CrossRef]
- Amstutz, H.C.; Thomas, B.J.; Jinnah, R.; Kim, W.; Grogan, T.; Yale, C. Treatment of primary osteoarthritis of the hip. A comparison of total joint and surface replacement arthroplasty. J. Bone Jt. Surg. Am. 1984, 66, 228–241. [Google Scholar] [CrossRef]
- Mäkelä, K.T.; Eskelinen, A.; Pulkkinen, P.; Paavolainen, P.; Remes, V. Total hip arthroplasty for primary osteoarthritis in patients fifty-five years of age or older: An analysis of the Finnish arthroplasty registry. J. Bone Jt. Surg. Am. 2008, 90, 2160–2170. [Google Scholar] [CrossRef]
- Horlocker, T.T. Pain Management in total joint arthroplasty: A historical review. Orthopedics 2010, 33, 14–19. [Google Scholar] [CrossRef]
- Daras, M.; Macaulay, W. Total hip arthroplasty in young patients with osteoarthritis. Am. J. Orthop. 2009, 38, 125–129. [Google Scholar] [PubMed]
- McLaughlin, J.R.; Lee, K.R. Total Hip Arthroplasty in Young Patients: 8-to 13-Year Results Using an Uncemented Stem. Clin. Orthop. Relat. Res. 2000, 373, 153–163. [Google Scholar] [CrossRef]
- Deans, C.F.; Buckner, B.C.; Garvin, K.L. Wear, Osteolysis, and Aseptic Loosening Following Total Hip Arthroplasty in Young Patients with Highly Cross-Linked Polyethylene: A Review of Studies with a Follow-Up of over 15 Years. J. Clin. Med. 2023, 12, 6615. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.Y.; Yoon, T.-R. Recent updates for biomaterials used in total hip arthroplasty. Biomater. Res. 2018, 22, 33. [Google Scholar] [CrossRef]
- El-Desouky, I.I.; Helal, A.H.; Mansour, A.M.R. Ten-year survival of ceramic-on-ceramic total hip arthroplasty in patients younger than 60 years: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2021, 16, 679. [Google Scholar] [CrossRef]
- Patel, I.; Nham, F.; Zalikha, A.K.; El-Othmani, M.M. Epidemiology of total hip arthroplasty: Demographics, comorbidities and outcomes. Arthroplasty 2023, 5, 2. [Google Scholar] [CrossRef]
- Adeyemi, A.; Trueman, P. Economic burden of surgical site infections within the episode of care following joint replacement. J. Orthop. Surg. Res. 2019, 14, 196. [Google Scholar] [CrossRef] [PubMed]
- Zomar, B.O.; Marsh, J.D.; Lanting, B.A.; Bryant, D.M. A protocol for a randomized controlled trial investigating the safety and cost-effectiveness of outpatient total hip arthroplasty. BMC Musculoskelet. Disord. 2020, 21, 663. [Google Scholar] [CrossRef] [PubMed]
- Chin, G.; Wright, D.J.; Snir, N.; Schwarzkopf, R. Primary vs. conversion total hip arthroplasty: A cost analysis. J. Arthroplast. 2016, 31, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Daigle, M.E.; Weinstein, A.M.; Katz, J.N.; Losina, E. The cost-effectiveness of total joint arthroplasty: A systematic review of published literature. Best Pract. Res. Clin. Rheumatol. 2012, 26, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Punzi, L.; Frigato, M.; Frallonardo, P.; Ramonda, R. Post-traumatic arthritis: Overview on pathogenic mechanisms and role of inflammation. RMD Open 2016, 2, e000279. [Google Scholar] [CrossRef] [PubMed]
- Negm, A.M.; Beaupre, L.A.; Goplen, C.M.; Weeks, C.; Jones, C.A. A scoping review of total hip arthroplasty survival and reoperation rates in patients of 55 years or younger: Health services implications for revision surgeries. Arthroplast. Today 2022, 16, 247–258. [Google Scholar] [CrossRef]
- Nasimuzzaman, M.; Malik, P. Role of the coagulation system in the pathogenesis of sickle cell disease. Blood Adv. 2019, 3, 3170–3180. [Google Scholar] [CrossRef]
- Kaur, D.; Kerlin, B.A. Bleeding associated with connective tissue disorders. In Management of Bleeding Patients; Springer: Cham, Switzerland, 2021; pp. 201–209. [Google Scholar]
- Jeong, G.K.; Cross, M.B.; Morin, R.L.; Rodriguez, E.K.; Zurakowski, D.; Thornhill, T.S. Total hip arthroplasty in sickle cell hemoglobinopathies. J. Am. Acad. Orthop. Surg. 2005, 13, 208–217. [Google Scholar] [CrossRef]
- Moran, M.M.; Wessman, P.; Rolfson, O.; Bohl, D.D.; Kärrholm, J.; Keshavarzian, A.; Sumner, D.R. The risk of revision following total hip arthroplasty in patients with inflammatory bowel disease, a registry based study. PLoS ONE 2021, 16, e0257310. [Google Scholar] [CrossRef]
- Korompilias, A.V.; Ortel, T.L.; Urbaniak, J.R. Coagulation abnormalities in patients with hip osteonecrosis. Orthop. Clin. N. Am. 2004, 35, 265–271. [Google Scholar] [CrossRef]
- Conroy, J.L.; Whitehouse, M.R.; Bolland, B.J.R.F.; Timperley, A.J.; Gie, G.A.; Howell, J.R. Risk factors for revision for early dislocation in total hip arthroplasty. J. Arthroplast. 2008, 23, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Lamb, J.N.; Baetz, J.; Messer-Hannemann, P.; Eastwick-Field, P.; Emerton, M.; Pandit, H.G. Risk factors for intraoperative periprosthetic femoral fractures during primary total hip arthroplasty. An analysis from the national joint registry for England and Wales and the Isle of Man. J. Arthroplast. 2019, 34, 3065–3073. [Google Scholar] [CrossRef] [PubMed]
- Ricioli, W.; Dall’Oca, C.; Andriolo, L.; Valenti, M.T.; Ortolani, S.; Samaila, E.M. Prevalence and risk factors for intra-operative periprosthetic fractures in one thousand eight hundred and seventy two patients undergoing total hip arthroplasty: A cross-sectional study. Int. Orthop. 2015, 39, 1939–1943. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.P.; Watts, C.D.; Houdek, M.T.; Lewallen, D.G.; Berry, D.J. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hip arthroplasties: A 40-year experience. Bone Jt. J. 2016, 98, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Busch, V. The young osteoarthritic hip: Clinical outcome of total hip arthroplasty and a cost-effectiveness analysis. Acta Orthop. 2015, 86 (Suppl. S360), S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Ashraf, A.; Singh, V.K.; Mehta, S.S.; Woodgate, I. Hospital costs of total hip arthroplasty for developmental dysplasia of the hip. Clin. Orthop. Relat. Res. 2014, 472, 2237–2244. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Mahamid, A.; Finkel, B.; Gan-Or, H.; Fournier, L.; Berkovich, Y.; Behrbalk, E. Comparative evaluation of postoperative outcomes and expenditure between robotic and conventional single-level lumbar fusion surgery: A comprehensive analysis of nationwide inpatient sample data. Eur. Spine J. 2024, 33, 2637–2645. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Laver, L.; Becker, R.; Mahamid, A.; Berkovich, Y. Robotic-assisted total knee arthroplasty reduces postoperative complications and length of stay without increased cost compared to navigation-guided techniques: A national analysis. Knee Surg. Sports Traumatol. Arthrosc. 2024. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Laver, L.; Becker, R.; Takrori, L.A.; Mahamid, A.; Finkel, B.; Gan-Or, H.; Yonai, Y.; Berkovich, Y. Trends and Epidemiology in Robotic-Assisted Total Knee Arthroplasty: Reduced Complications and Shorter Hospital Stays. Knee Surg. Sports Traumatol. Arthrosc. 2024. [Google Scholar] [CrossRef]
- Maman, D.; Mahamid, A.; Yonai, Y.; Berkovich, Y. Comparing Complication Rates, Costs, and Length of Stay between Unicompartmental and Total Knee Arthroplasty: Insights from a Big Data Analysis Using the National Inpatient Sample Dataset. J. Clin. Med. 2024, 13, 3888. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Etiologies | Under 35 | Age 35–44.9 | Age 45–54.9 | Significance |
|---|---|---|---|---|
| Primary osteoarthritis (%) | 56.15% | 77.30% | 91.32% | p < 0.0001 |
| Osteonecrosis (%) | 35.86% | 20.16% | 7.77% | |
| Congenital deformities of hip (%) | 2.69% | 1.14% | 0.31% | |
| Legg–Calvé–Perthes disease | 2.24% | 0.34% | 0.07% | |
| Rheumatoid arthritis (%) | 1.15% | 0.29% | 0.21% | |
| Juvenile rheumatoid arthritis (%) | 0.73% | 0.11% | 0.01% | |
| Post-traumatic arthritis (%) | 0.60% | 0.50% | 0.20% | |
| Acquired leg deformity (%) | 0.27% | 0.11% | 0.07% | |
| Arthropathic psoriasis (%) | 0.12% | 0.05% | 0.03% | |
| Systemic lupus erythematosus (%) | 0.18% | 0.00% | 0.01% |
| Parameter | Under 35 | Age 35–44.9 | Age 45–54.9 | Significance |
|---|---|---|---|---|
| Total surgeries (count) | 16,295 | 41,045 | 174,290 | - |
| Female (%) | 45.4% | 43.7% | 46.1% | p < 0.0001 |
| Payer—Medicare (%) | 8.1% | 9.2% | 9.6% | p < 0.0001 |
| Payer—Medicaid (%) | 28.0% | 19.1% | 13.8% | |
| Payer—private (%) | 56.8% | 65.2% | 71.0% | |
| Payer—other (including self-pay) (%) | 7.2% | 6.6% | 5.6% | |
| Race—White (%) | 62.5% | 71.0% | 78.2% | p < 0.0001 |
| Race—Black (%) | 18.7% | 16.0% | 13.0% | |
| Race—Hispanic (%) | 11.1% | 8.0% | 5.4% | |
| Race—Asian or Pacific Islander (%) | 2.9% | 1.8% | 1.0% | |
| Race—Native American (%) | 0.6% | 0.6% | 0.4% | |
| Race—Other (%) | 4.2% | 2.7% | 2.0% |
| Parameter | Under 35 | Age 35–44.9 | Age 45–54.9 | Significance |
|---|---|---|---|---|
| Hypertension diagnosis (%) | 12.64% | 28.15% | 41.31% | p < 0.0001 |
| Dyslipidemia diagnosis (%) | 3.99% | 13.03% | 24.23% | p < 0.0001 |
| Chronic anemia (%) | 5.58% | 4.98% | 4.95% | p = 0.002 |
| Osteoporosis (%) | 1.26% | 1.02% | 1.32% | p < 0.0001 |
| Alcohol abuse (%) | 2.70% | 3.16% | 2.47% | p < 0.0001 |
| Type 2 diabetes (%) | 2.33% | 6.42% | 10.45% | p < 0.0001 |
| Renal disease (%) | 2.49% | 1.89% | 2.11% | p < 0.0001 |
| CHF (%) | 0.25% | 0.32% | 0.63% | p = 0.004 |
| Chronic lung disease (%) | 0.61% | 2.07% | 4.37% | p < 0.0001 |
| Obesty (%) | 18.35% | 28.05% | 30.42% | p < 0.0001 |
| Morbid (severe) obesity (%) | 9.79% | 17.51% | 18.62% | p < 0.0001 |
| IBD | 1.4% | 1.1% | 0.6% | p < 0.0001 |
| Coagulation defects | 1.2% | 1.0% | 0.8% | p < 0.0001 |
| Connective tissues disorder | 0.6% | 0.3% | 0.1% | p < 0.0001 |
| Gout | 0.7% | 1.8% | 2.5% | p < 0.0001 |
| Use of anticoagulants | 2.30% | 2.05% | 2.61% | p < 0.0001 |
| Sickle cell disorder | 5.3% | 1.2% | 0.3% | p < 0.0001 |
| Parameter | Under 35 | Age 35–44.9 | Age 45–54.9 | Significance |
|---|---|---|---|---|
| Died during hospitalization (%) | 0.031 | 0.000 | 0.017 | p = 0.009 |
| Length of stay (mean in days) | 2.08 | 1.89 | 1.82 | p < 0.0001 |
| Total charges (mean in $) | 70,540 | 65,716 | 62,589 | p < 0.0001 |
| Parameter | Under 35 | Age 35–44.9 | Age 45–54.9 | Significance |
|---|---|---|---|---|
| Blood loss anemia (%) | 16.69% | 16.10% | 15.25% | p < 0.0001 |
| Blood transfusion (%) | 3.80% | 2.63% | 2.04% | p < 0.0001 |
| Intraoperative fracture (%) | 0.83% | 0.74% | 0.66% | p < 0.0001 |
| Hip dislocation (%) | 0.49% | 0.33% | 0.30% | p < 0.0001 |
| Pneumonia (%) | 0.15% | 0.05% | 0.09% | p < 0.0001 |
| Venous thromboembolism (%) | 0.12% | 0.16% | 0.07% | p < 0.0001 |
| Pulmonary embolism (%) | 0.09% | 0.11% | 0.06% | p = 0.005 |
| Acute kidney injury (%) | 0.61% | 0.69% | 0.81% | p = 0.002 |
| Acute coronary artery disease (%) | 0.00% | 0.00% | 0.02% | p = 0.003 |
| Pulmonary edema (%) | 0.00% | 0.00% | 0.02% | p = 0.001 |
| Heart failure (%) | 0.00% | 0.01% | 0.01% | p = 0.301 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maman, D.; Fournier, L.; Steinfeld, Y.; Berkovich, Y. Etiology, Outcomes, and Complications of Total Hip Arthroplasty in Younger Patients: A Nationwide Big Data Analysis. J. Clin. Med. 2024, 13, 4535. https://doi.org/10.3390/jcm13154535
Maman D, Fournier L, Steinfeld Y, Berkovich Y. Etiology, Outcomes, and Complications of Total Hip Arthroplasty in Younger Patients: A Nationwide Big Data Analysis. Journal of Clinical Medicine. 2024; 13(15):4535. https://doi.org/10.3390/jcm13154535
Chicago/Turabian StyleMaman, David, Linor Fournier, Yaniv Steinfeld, and Yaron Berkovich. 2024. "Etiology, Outcomes, and Complications of Total Hip Arthroplasty in Younger Patients: A Nationwide Big Data Analysis" Journal of Clinical Medicine 13, no. 15: 4535. https://doi.org/10.3390/jcm13154535
APA StyleMaman, D., Fournier, L., Steinfeld, Y., & Berkovich, Y. (2024). Etiology, Outcomes, and Complications of Total Hip Arthroplasty in Younger Patients: A Nationwide Big Data Analysis. Journal of Clinical Medicine, 13(15), 4535. https://doi.org/10.3390/jcm13154535