
Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis
 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection, Data Extraction and Quality Assessment
2.3. Outcome Definition
2.4. Statistical Analysis
3. Results
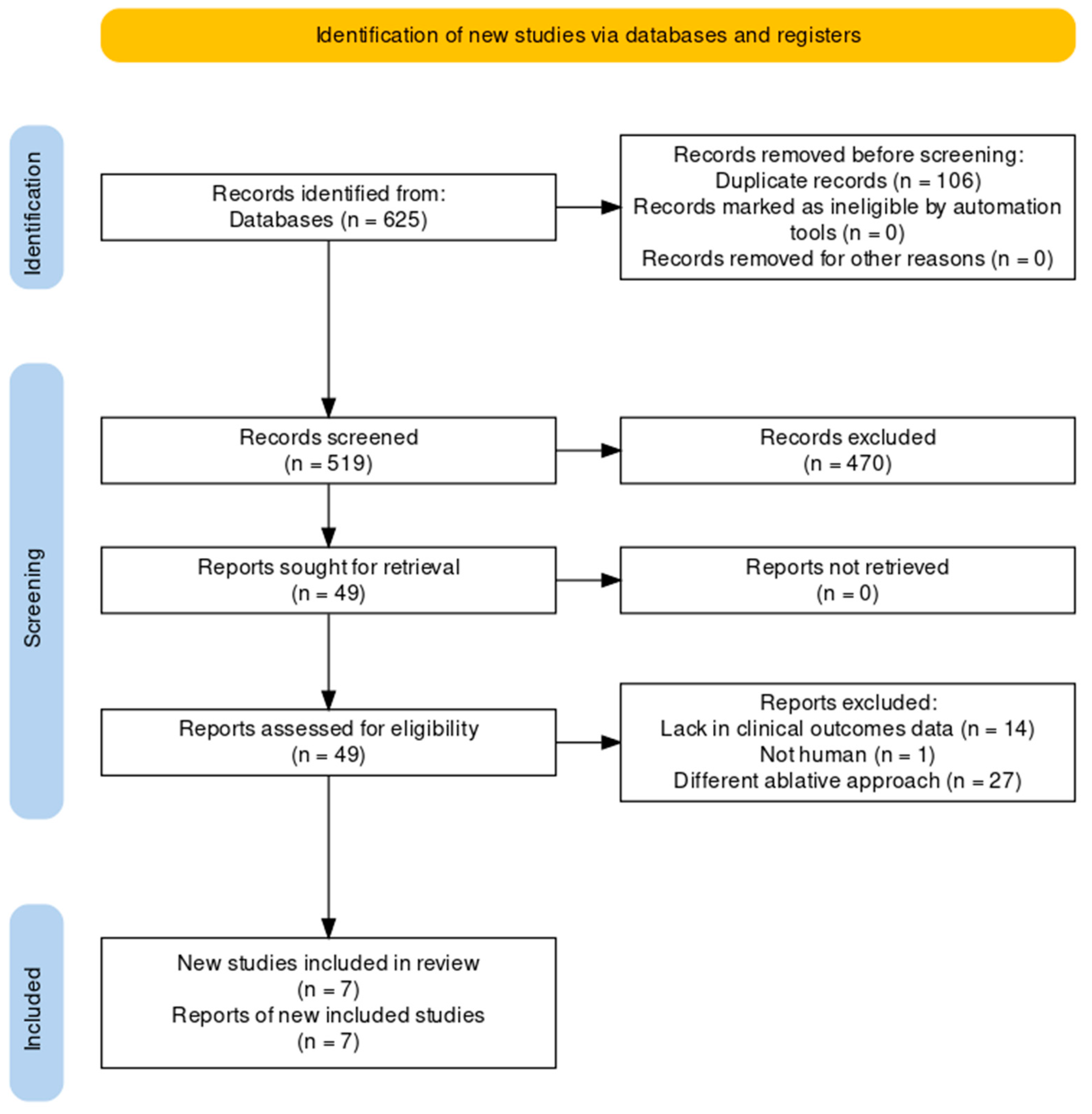
3.1. Search Results and Baseline Characteristics
3.2. Risk of Bias
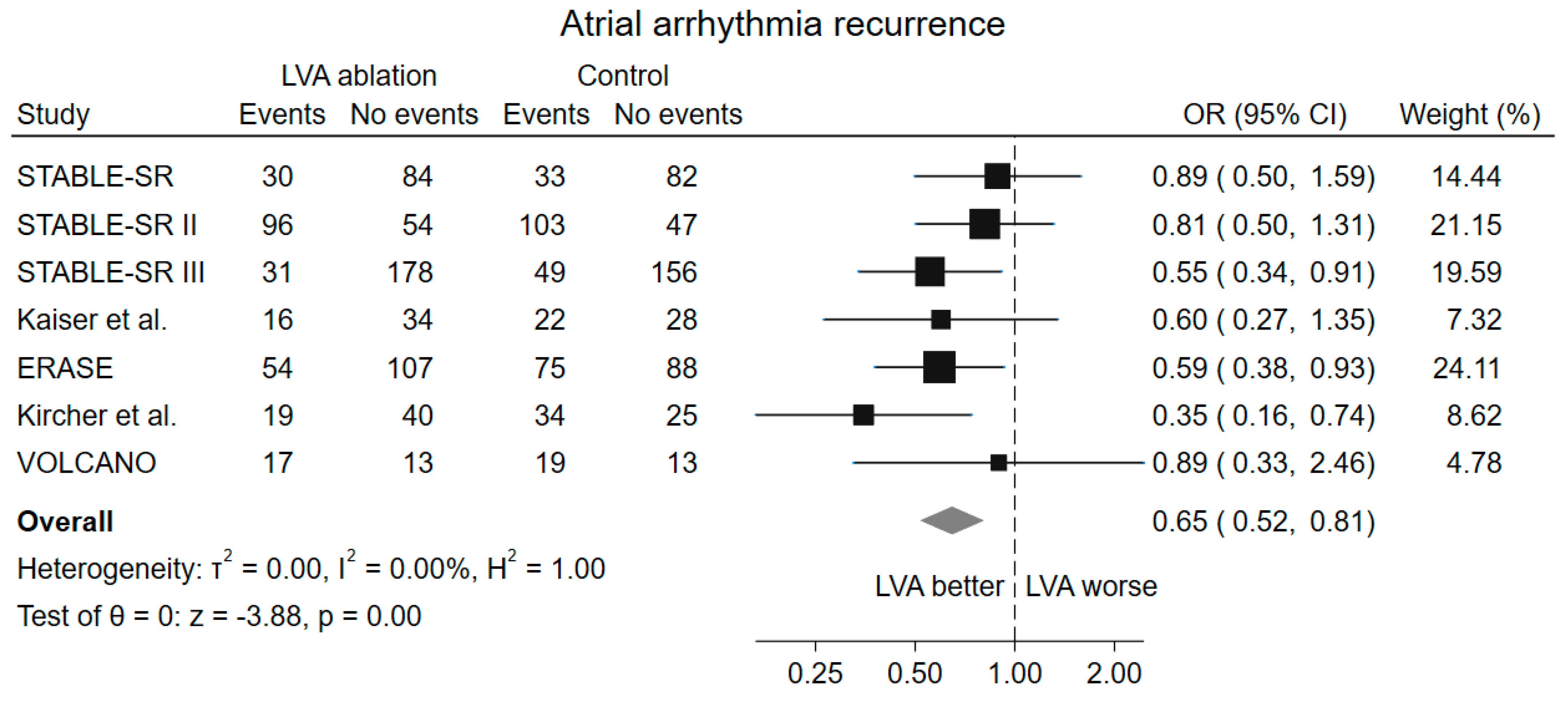
3.3. Primary Outcome
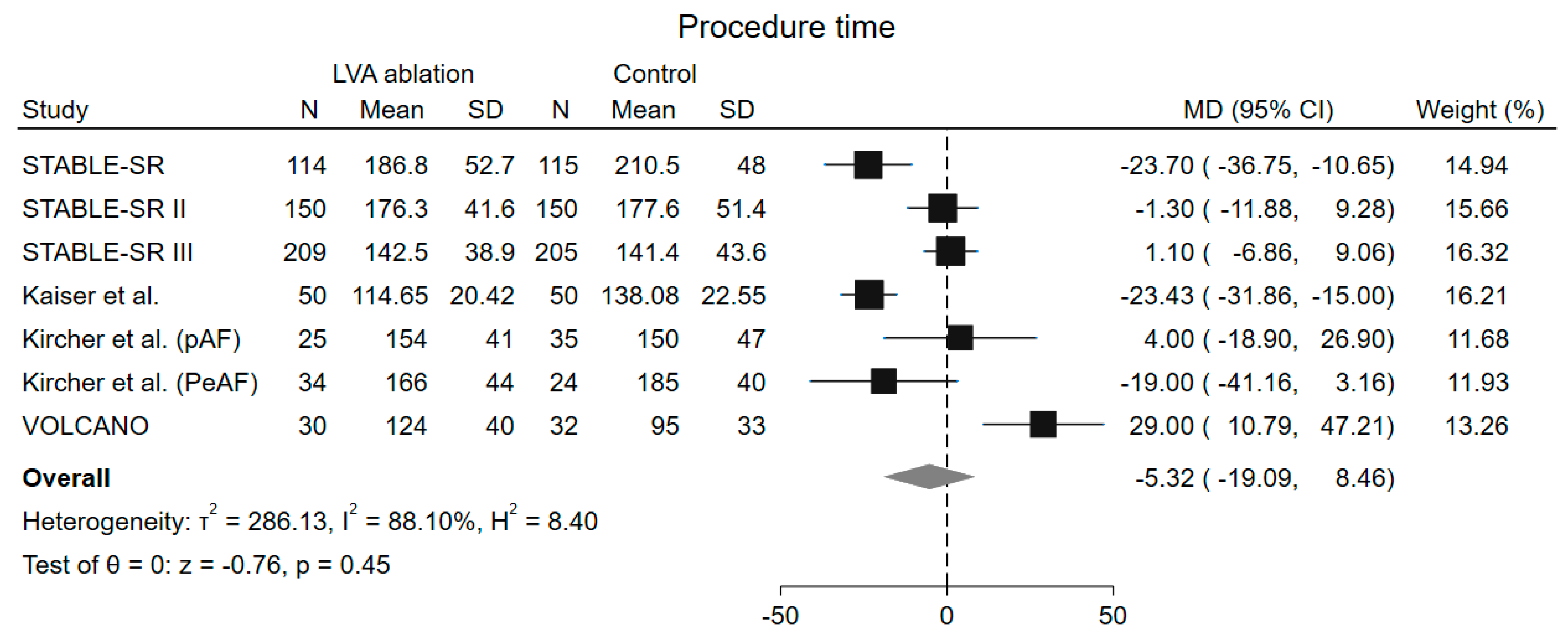
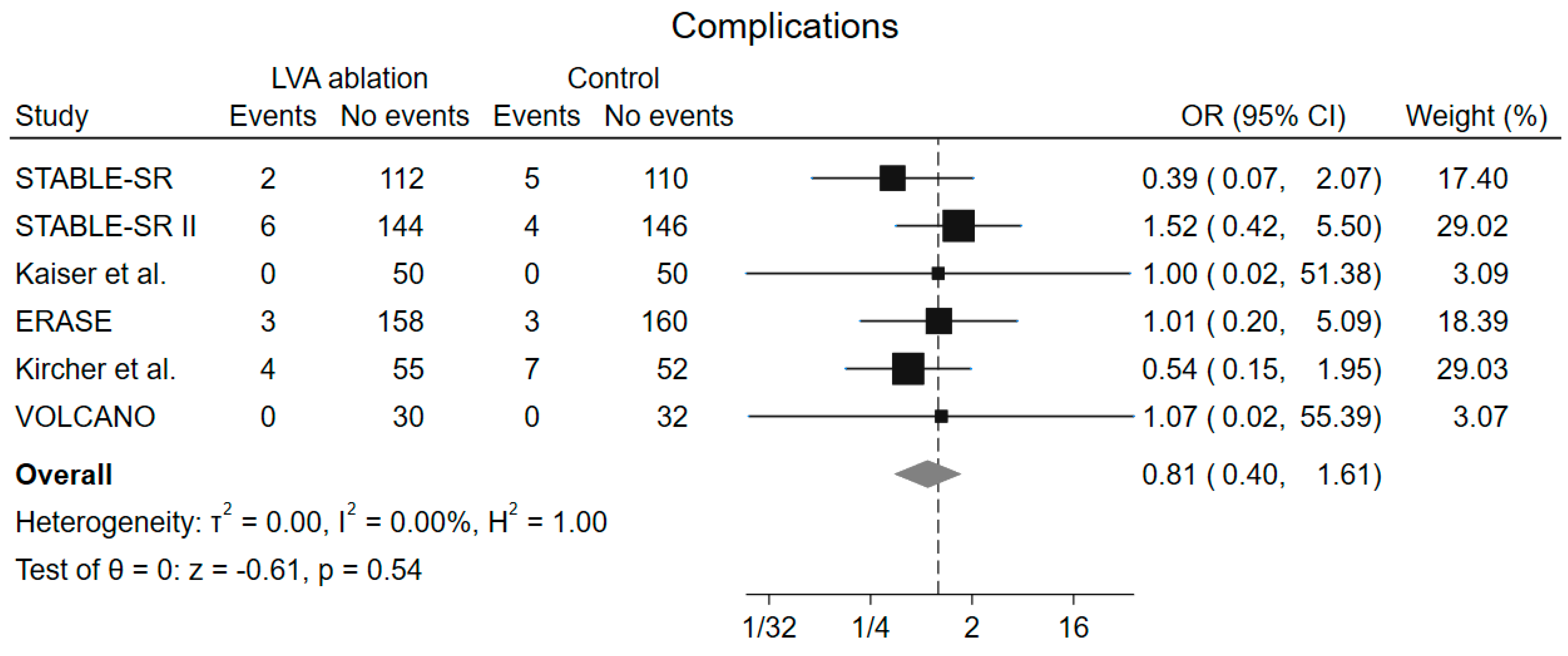
3.4. Secondary Outcomes
3.5. Subgroup and Metaregression Analysis
4. Discussion
4.1. Presence of Low Voltages Areas
4.2. Paroxysmal and Persistent Atrial Fibrillation
4.3. Relevance of the Ablation Strategy
4.4. Procedure and Fluoroscopy Time
4.5. Novelty of the Current Metanalysis and Clinical Implications
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| CFAE | Complex Fractionated Atrial Electrogram |
| EAM | Electroanatomical Mapping |
| LAD | Left Atrium Diameter |
| LVEF | Left Ventricular Ejection Fraction |
| LVA | Low-Voltage Area |
| MD | Mean Difference |
| MRI | Magnetic Resonance Imaging |
| OR | Odds Rratio |
| PAF | Paroxysmal Atrial Fibrillation |
| PeAF | Persistent Atrial Fibrillation |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | International Prospective Register of Systematic Reviews |
| PVI | Pulmonary Vein Isolation |
| RCTs | Randomized Clinical Trials |
| REML | Restricted Maximum Likelihood |
| ROB2 | Cochrane Risk of Bias Tool |
References
- Dong, X.J.; Wang, B.B.; Hou, F.F.; Jiao, Y.; Li, H.W.; Lv, S.P.; Li, F.H. Global Burden of Atrial Fibrillation/Atrial Flutter and Its Attributable Risk Factors from 1990 to 2019. Europace 2023, 25, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Arbelo, E.; Aktaa, S.; Bollmann, A.; D’Avila, A.; Drossart, I.; Dwight, J.; Hills, M.T.; Hindricks, G.; Kusumoto, F.M.; Lane, D.A.; et al. Quality Indicators for the Care and Outcomes of Adults with Atrial Fibrillation: Task Force for the Development of Quality Indicators in Atrial Fibrillation of the European Heart Rhythm Association (EHRA) of the European Society of Cardiology (ESC): Developed in Collaboration with the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), and the Latin-American Heart Rhythm Society (LAHRS). EP Eur. 2021, 23, 494–495. [Google Scholar] [CrossRef]
- Nabauer, M.; Oeff, M.; Gerth, A.; Wegscheider, K.; Buchholz, A.; Haeusler, K.G.; Hanrath, P.; Meinertz, T.; Ravens, U.; Sprenger, C.; et al. Prognostic Markers of All-Cause Mortality in Patients with Atrial Fibrillation: Data from the Prospective Long-Term Registry of the German Atrial Fibrillation NETwork (AFNET). EP Eur. 2021, 23, 1903–1912. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Joglar, J.A.; Chung, M.K.; Armbruster, A.L.; Benjamin, E.J.; Chyou, J.Y.; Cronin, E.M.; Deswal, A.; Eckhardt, L.L.; Goldberger, Z.D.; Gopinathannair, R.; et al. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024, 149, e1–e156. [Google Scholar] [CrossRef]
- Berger, W.R.; Meulendijks, E.R.; Limpens, J.; van den Berg, N.W.E.; Neefs, J.; Driessen, A.H.G.; Krul, S.P.J.; van Boven, W.J.P.; de Groot, J.R. Persistent Atrial Fibrillation: A Systematic Review and Meta-Analysis of Invasive Strategies. Int. J. Cardiol. 2019, 278, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Voskoboinik, A.; Moskovitch, J.T.; Harel, N.; Sanders, P.; Kistler, P.M.; Kalman, J.M. Revisiting Pulmonary Vein Isolation Alone for Persistent Atrial Fibrillation: A Systematic Review and Meta-Analysis. Heart Rhythm 2017, 14, 661–667. [Google Scholar] [CrossRef]
- Wynn, G.J.; Panikker, S.; Morgan, M.; Hall, M.; Waktare, J.; Markides, V.; Hussain, W.; Salukhe, T.; Modi, S.; Jarman, J.; et al. Biatrial Linear Ablation in Sustained Nonpermanent AF: Results of the Substrate Modification with Ablation and Antiarrhythmic Drugs in Nonpermanent Atrial Fibrillation (SMAN-PAF) Trial. Heart Rhythm 2016, 13, 399–406. [Google Scholar] [CrossRef]
- Verma, A.; Jiang, C.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef]
- Vogler, J.; Willems, S.; Sultan, A.; Schreiber, D.; Lüker, J.; Servatius, H.; Schäffer, B.; Moser, J.; Hoffmann, B.A.; Steven, D. Pulmonary Vein Isolation Versus Defragmentation: The CHASE-AF Clinical Trial. J. Am. Coll. Cardiol. 2015, 66, 2743–2752. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Kirchhof, P.; Kühne, M.; Ahlsson, A.; Balsam, P.; Bauersachs, J.; Benussi, S.; Brandes, A.; Braunschweig, F.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the Diagnosis and Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Developed with the Special Contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Blandino, A.; Bianchi, F.; Grossi, S.; Biondi-Zoccai, G.; Conte, M.R.; Gaido, L.; Gaita, F.; Scaglione, M.; Rametta, F. Left Atrial Substrate Modification Targeting Low-Voltage Areas for Catheter Ablation of Atrial Fibrillation: A Systematic Review and Meta-Analysis. Pacing Clin. Electrophysiol. 2017, 40, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Starek, Z.; Di Cori, A.; Betts, T.R.; Clerici, G.; Gras, D.; Lyan, E.; Della Bella, P.; Li, J.; Hack, B.; Verbick, L.Z.; et al. Baseline Left Atrial Low-Voltage Area Predicts Recurrence after Pulmonary Vein Isolation: WAVE-MAP AF Results. Europace 2023, 25, euad194. [Google Scholar] [CrossRef]
- Masuda, M.; Asai, M.; Iida, O.; Okamoto, S.; Ishihara, T.; Nanto, K.; Kanda, T.; Tsujimura, T.; Matsuda, Y.; Okuno, S.; et al. Additional Low-Voltage-Area Ablation in Patients with Paroxysmal Atrial Fibrillation: Results of the Randomized Controlled Volcano Trial. J. Am. Heart Assoc. 2020, 9, e015927. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, C.; Han, B.; Xiao, F.; Yi, F.; Wei, Y.; Jiang, C.; Zou, C.; Shi, L.; Ma, W.; et al. Circumferential Pulmonary Vein Isolation with vs without Additional Low-Voltage-Area Ablation in Older Patients with Paroxysmal Atrial Fibrillation: A Randomized Clinical Trial. JAMA Cardiol. 2023, 8, 765–772. [Google Scholar] [CrossRef]
- Yang, B.; Jiang, C.; Lin, Y.; Yang, G.; Chu, H.; Cai, H.; Lu, F.; Zhan, X.; Xu, J.; Wang, X.; et al. STABLE-SR (Electrophysiological Substrate Ablation in the Left Atrium during Sinus Rhythm) for the Treatment of Nonparoxysmal Atrial Fibrillation: A Prospective, Multicenter Randomized Clinical Trial. Circ. Arrhythmia Electrophysiol. 2017, 10, e005405. [Google Scholar] [CrossRef]
- Yang, G.; Zheng, L.; Jiang, C.; Fan, J.; Liu, X.; Zhan, X.; Li, J.; Wang, L.; Yang, H.; Zhu, W.; et al. Circumferential Pulmonary Vein Isolation Plus Low-Voltage Area Modification in Persistent Atrial Fibrillation: The STABLE-SR-II Trial. JACC Clin. Electrophysiol. 2022, 8, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, B.; Huber, C.; Pirozzolo, G.; Maier, P.; Bekeredjian, R.; Theis, C. Persistent Atrial Fibrillation without the Evidence of Low-Voltage Areas: A Prospective Randomized Trial. J. Interv. Card. Electrophysiol. 2024, 67, 83–90. [Google Scholar] [CrossRef]
- Huo, Y.; Gaspar, T.; Schönbauer, R.; Wójcik, M.; Fiedler, L.; Roithinger, F.X.; Martinek, M.; Pürerfellner, H.; Kirstein, B.; Richter, U.; et al. Low-Voltage Myocardium-Guided Ablation Trial of Persistent Atrial Fibrillation. NEJM Evid. 2022, 1, EVIDoa2200141. [Google Scholar] [CrossRef]
- Kircher, S.; Arya, A.; Altmann, D.; Rolf, S.; Bollmann, A.; Sommer, P.; Dagres, N.; Richter, S.; Breithardt, O.A.; Dinov, B.; et al. Individually Tailored vs. Standardized Substrate Modification during Radiofrequency Catheter Ablation for Atrial Fibrillation: A Randomized Study. Europace 2018, 20, 1766–1775. [Google Scholar] [CrossRef]
- Mao, S.; Fan, H.; Wang, L.; Wang, Y.; Wang, X.; Zhao, J.; Yu, B.; Zhang, Y.; Zhang, W.; Liang, B. A Systematic Review and Meta-Analysis of the Safety and Efficacy of Left Atrial Substrate Modification in Atrial Fibrillation Patients with Low Voltage Areas. Front. Cardiovasc. Med. 2022, 9, 969475. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: Reconstruct Individual Patient Data from Published Kaplan-Meier Survival Curves. BMC Med. Res. Methodol. 2021, 21, 111. [Google Scholar] [CrossRef] [PubMed]
- Masuda, M.; Asai, M.; Iida, O.; Okamoto, S.; Ishihara, T.; Nanto, K.; Kanda, T.; Tsujimura, T.; Matsuda, Y.; Hata, Y.; et al. Low-Voltage-Area Ablation in Paroxysmal Atrial Fibrillation ― Extended Follow-up Results of the VOLCANO Trial. Circ. J. 2022, 86, 245–252. [Google Scholar] [CrossRef]
- Falasconi, G.; Penela, D.; Soto-Iglesias, D.; Francia, P.; Saglietto, A.; Turturiello, D.; Viveros, D.; Bellido, A.; Alderete, J.; Zaraket, F.; et al. Personalized Pulmonary Vein Isolation with Very High-Power Short-Duration Lesions Guided by Left Atrial Wall Thickness: The QDOT-by-LAWT Randomized Trial. Europace 2024, 26, euae087. [Google Scholar] [CrossRef] [PubMed]
- Saglietto, A.; Falasconi, G.; Soto-Iglesias, D.; Francia, P.; Penela, D.; Alderete, J.; Viveros, D.; Bellido, A.F.; Franco-Ocaña, P.; Zaraket, F.; et al. Assessing Left Atrial Intramyocardial Fat Infiltration from Computerized Tomography Angiography in Patients with Atrial Fibrillation. Europace 2023, 25, euad351. [Google Scholar] [CrossRef] [PubMed]
- Parameswaran, R.; Al-Kaisey, A.M.; Kalman, J.M. Catheter Ablation for Atrial Fibrillation: Current Indications and Evolving Technologies. Nat. Rev. Cardiol. 2021, 18, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Al-Kaisey, A.M.; Parameswaran, R.; Kalman, J.M. Atrial Fibrillation Structural Substrates: Aetiology, Identification and Implications. Arrhythmia Electrophysiol. Rev. 2020, 9, 113. [Google Scholar] [CrossRef]
- Tzeis, S.; Gerstenfeld, E.P.; Kalman, J.; Saad, E.B.; Sepehri Shamloo, A.; Andrade, J.G.; Barbhaiya, C.R.; Baykaner, T.; Boveda, S.; Calkins, H.; et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation. Europace 2024, 26, euae043. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Wazni, O.; McGann, C.; Greene, T.; Dean, J.M.; Dagher, L.; Kholmovski, E.; Mansour, M.; Marchlinski, F.; Wilber, D.; et al. Effect of MRI-Guided Fibrosis Ablation vs Conventional Catheter Ablation on Atrial Arrhythmia Recurrence in Patients with Persistent Atrial Fibrillation: The DECAAF II Randomized Clinical Trial. JAMA 2022, 327, 2296–2305. [Google Scholar] [CrossRef]
- Moustafa, A.; Karim, S.; Kahaly, O.; Elzanaty, A.; Meenakshisundaram, C.; Abi-Saleh, B.; Eltahawy, E.; Chacko, P. Low Voltage Area Guided Substrate Modification in Nonparoxysmal Atrial Fibrillation: A Systematic Review and Meta-Analysis. J. Cardiovasc. Electrophysiol. 2023, 34, 455–464. [Google Scholar] [CrossRef]
- Junarta, J.; Siddiqui, M.U.; Riley, J.M.; Dikdan, S.J.; Patel, A.; Frisch, D.R. Low-Voltage Area Substrate Modification for Atrial Fibrillation Ablation: A Systematic Review and Meta-Analysis of Clinical Trials. Europace 2022, 24, 1585–1598. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Wang, W.; Yu, B. Efficacy and Safety of Low Voltage Area Ablation for Atrial Fibrillation: A Systematic Review and Meta-Analysis. J. Interv. Card. Electrophysiol. 2023, 66, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Rivera, A.; Gewehr, D.M.; Braga, M.A.P.; Carvalho, P.E.P.; Ternes, C.M.P.; Pantaleao, A.N.; Hincapie, D.; Serpa, F.; Romero, J.E.; d’Avila, A. Adjunctive Low-Voltage Area Ablation for Patients with Atrial Fibrillation: An Updated Meta-Analysis of Randomized Controlled Trials. J. Cardiovasc. Electrophysiol. 2024, 35, 1329–1339. [Google Scholar] [CrossRef]
- Hwang, J.; Park, H.S.; Han, S.; Lee, C.H.; Kim, I.C.; Cho, Y.K.; Yoon, H.J.; Chung, J.W.; Kim, H.; Nam, C.W.; et al. Ablation of Persistent Atrial Fibrillation Based on High Density Voltage Mapping and Complex Fractionated Atrial Electrograms: A Randomized Controlled Trial. Medicine 2021, 100, E26702. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, K.; Toyama, H.; Zhang, B. Effects of Additional Ablation of Low-Voltage Areas after Box Isolation for Persistent Atrial Fibrillation. J. Arrhythmia 2019, 35, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.H.; Li, Z.; Mao, J.L.; He, B. A Novel Individualized Substrate Modification Approach for the Treatment of Long-Standing Persistent Atrial Fibrillation: Preliminary Results. Int. J. Cardiol. 2014, 175, 162–168. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Design | Population | Experimental Arm | Control Arm | Energy Source | Endpoint | Follow Up |
|---|---|---|---|---|---|---|---|
| B. Yang et al. [16] (STABLE-SR) | Multicenter, single-blinded, randomized clinical trial | Non-paroxysmal AF | PVI + cavotricuspid isthmus ablation + LVA ablation | PVI + STEPWISE ablation | Radiofrequency | Freedom from documented atrial arrhythmias for >30 s without the use of antiarrhythmic drugs | 18 months |
| G. Yang et al. [17] (STABLE-SR II) | Multicenter, single-blinded, randomized clinical trial | Non-paroxysmal AF | PVI + LVA ablation | PVI | Radiofrequency | Freedom from documented atrial arrhythmias for >30 s without the use of antiarrhythmic drugs | 18 months |
| H. Chen et al. [15] (STABLE-SR III) | Multicenter, single-blind, randomized clinical trial | Paroxysmal AF, 65 to 80 years | PVI + LVA ablation | PVI | Radiofrequency | Freedom from documented atrial arrhythmias for >30 s without the use of antiarrhythmic drugs | 23 months |
| Y. Huo et al. [19] (ERASE) | Multicenter, single-blinded, randomized clinical trial | Persistent AF | PVI + LVA ablation | PVI | Radiofrequency | Freedom from documented atrial arrhythmias for >30 s | 12 months |
| S. Kircher et al. [20] | Single-center, single-blinded, randomized clinical trial | Paroxysmal and Persistent AF | PVI + LVA ablation | PVI (+ posterior wall box and posterior mitral annulus line in persistent AF) | Radiofrequency | Freedom from documented atrial arrhythmias for >30 s | 12 months |
| B. Kaiser et al. [18] | Single-center, single-blinded, randomized clinical trial. | Persistent AF | PVI + LVA ablation | PVI + linear lesions + CFAE ablation | Radiofrequency | Freedom from any atrial arrhythmia after the 90 days blanking period without the use of antiarrhythmic drugs | 12 months |
| M. Masuda et al. [23] (VOLCANO) | Multicenter, single-blinded, randomized clinical trial. | Paroxysmal AF | PVI + LVA ablation | PVI alone | Radiofrequency or Cryoballoon | Freedom from any atrial arrhythmia after the 90 days blanking period without the use of antiarrhythmic drugs | 24 months |
| Study | Patients, No. | Age, Mean | Male, % | AF Duration (Months), Mean | CHA2DS2-VASc Score, Mean or Median | LVEF, % | LAD, mm | |
|---|---|---|---|---|---|---|---|---|
| STABLE-SR [16] | LVA ablation | 114 | 57.1 ± 9.5 | 81 | 18.9 ± 29 | - | 61.8 ± 7.7 | 41.1 ± 5.3 |
| Non-LVA ablation | 115 | 57.6 ± 8.4 | 74 | 15.9 ± 33 | - | 62.0 ± 6.6 | 40.7 ± 4.8 | |
| STABLE-SR II [17] | LVA ablation | 134 | 60.6 ± 9.4 | 67 | 6.0 (2.0–15.5) | - | 61.3 ± 9.2 | 41.4 ± 5.9 |
| Non-LVA ablation | 142 | 60.4 ± 9.6 | 70 | 6.0 (1.0–12.0) | - | 62.1 ± 6.8 | 42.5 ± 5.3 | |
| STABLE-SR III [15] | LVA ablation | 219 | 70.2 ± 4.7 | 51 | 24.0 (6.0–48.0) | 2.3 ± 0.8 | 62.4 ± 5.3 | 38.8 ± 5.4 |
| Non-LVA ablation | 219 | 70.7 ± 4.1 | 49 | 14 (4.0–48.0) | 2.5 ± 1.0 | 62.4 ± 5.4 | 38.8 ± 5.4 | |
| ERASE [19] | LVA ablation | 161 | 65 ± 10 | 70 | 31 (8–77) | 3 (2–4) | 53 ± 12 | 45 ± 7 |
| Non-LVA ablation | 163 | 66 ± 10 | 64 | 31 (12–77) | 3 (2–4) | 54 ± 11 | 45 ± 6 | |
| Kircher et al. [20] | LVA ablation | 62 | 62 ± 10 | 58 | 54 (24–87) | 2 (1–3) | 59 ± 9 | 43 ± 6 |
| Non-LVA ablation | 62 | 63 ± 9 | 66 | 60 (36–111) | 2 (1–3) | 61 ± 7 | 42 ± 6 | |
| Kaiser et al. [18] | LVA ablation | 50 | 65.20 ± 8.94 | 66 | - | 2.67 ± 1.58 | 53.35 ± 5.23 | - |
| Non-LVA ablation | 50 | 67.53 ± 10.83 | 72 | - | 2.55 ± 1.74 | 50.29 ± 9.61 | - | |
| VOLCANO [23] | LVA ablation | 30 | 75.3 ± 7.2 | 30 | 4 (2–14) | 3.6 ± 1.2 | 64 ± 14 | 40 ± 6 |
| Non-LVA ablation | 32 | 74.7 ± 8.0 | 28 | 5 (2–23) | 3.3 ± 1.3 | 65 ± 10 | 38 ± 5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valcher, S.; Villaschi, A.; Falasconi, G.; Chiarito, M.; Giunti, F.; Novelli, L.; Addeo, L.; Taormina, A.; Panico, C.; Francia, P.; et al. Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 4541. https://doi.org/10.3390/jcm13154541
Valcher S, Villaschi A, Falasconi G, Chiarito M, Giunti F, Novelli L, Addeo L, Taormina A, Panico C, Francia P, et al. Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(15):4541. https://doi.org/10.3390/jcm13154541
Chicago/Turabian StyleValcher, Stefano, Alessandro Villaschi, Giulio Falasconi, Mauro Chiarito, Filippo Giunti, Laura Novelli, Lucio Addeo, Antonio Taormina, Cristina Panico, Pietro Francia, and et al. 2024. "Low-Voltage Area Ablation in Addition to Pulmonary Vein Isolation in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 15: 4541. https://doi.org/10.3390/jcm13154541