
Machine Learning and Statistical Shape Modelling Methodologies to Assess Vascular Morphology before and after Aortic Valve Replacement

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Segmentation and 3D Reconstruction
2.3. Statistical Shape Modelling
2.4. Cluster Analysis
2.5. Data Analysis
3. Results
3.1. Patients Characteristics
3.2. Pre-Operative SSM Analysis
3.3. Post-Operative SSM Analysis
3.4. Pre-Operative Cluster Analysis
3.5. Post-Operative Cluster Analysis
4. Discussion
4.1. Limitations
4.2. Future Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Preoperative PCA Shape Modes—Ascending Aorta
Appendix A.2. Postoperative PCA Shape Modes—Ascending Aorta

Appendix A.3. Preoperative PCA Shape Modes—Whole Aorta

Appendix A.4. Postoperative PCA Shape Modes—Whole Aorta

References
- Ambellan, F.; Lamecker, H.; von Tycowicz, C.; Zachow, S. Statistical Shape Models: Understanding and Mastering Variation in Anatomy. Adv. Exp. Med. Biol. 2019, 1156, 67–84. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Peterson, A.C.; Aubert, B.; Morris, A.; Atkins, P.R.; Lenz, A.L.; Anderson, A.E.; Elhabian, S.Y. Statistical Multi-Level Shape Models for Scalable Modeling of Multi-Organ Anatomies. Front Bioeng Biotechnol. 2023, 11, 1089113. [Google Scholar] [CrossRef] [PubMed]
- Lever, J.; Krzywinski, M.; Altman, N. Principal Component Analysis. Nat. Methods 2017, 14, 641–642. [Google Scholar] [CrossRef]
- Sarkalkan, N.; Weinans, H.; Zadpoor, A.A. Statistical Shape and Appearance Models of Bones. Bone 2014, 60, 129–140. [Google Scholar] [CrossRef] [PubMed]
- IJpma, F.F.A.; Meesters, A.M.L.; Merema, B.B.J.; Ten Duis, K.; de Vries, J.P.M.; Banierink, H.; Wendt, K.W.; Kraeima, J.; Witjes, M.J.H. Feasibility of Imaging-Based 3-Dimensional Models to Design Patient-Specific Osteosynthesis Plates and Drilling Guides. JAMA Netw. Open 2021, 4, e2037519. [Google Scholar] [CrossRef]
- Vaura, F.C.; Salomaa, V.V.; Kantola, I.M.; Kaaja, R.; Lahti, L.; Niiranen, T.J. Unsupervised hierarchical clustering identifies a metabolically challenged subgroup of hypertensive individuals. J. Clin. Hypertens. 2020, 22, 1546–1553. [Google Scholar] [CrossRef]
- Alzate, C.; Suykens, J.A. Hierarchical kernel spectral clustering. Neural Netw. 2012, 35, 21–30. [Google Scholar] [CrossRef]
- Bhattacharjee, A.; Richards, W.G.; Staunton, J.; Li, C.; Monti, S.; Vasa, P.; Ladd, C.; Beheshti, J.; Bueno, R.; Gillette, M.; et al. Classification of human lung carcinomas by mRNA expression profiling reveals distinct adenocarcinoma subclasses. Proc. Natl. Acad. Sci. USA 2001, 98, 13790–13795. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, M.Z.; Comin, C.H.; Casanova, D.; Bruno, O.M.; Amancio, D.R.; Costa, L.D.F.; Rodrigues, F.A. Clustering algorithms: A comparative approach. PLoS ONE 2019, 14, e0210236. [Google Scholar] [CrossRef]
- Sebastiani, P.; Perls, T. Detection of Significant Groups in Hierarchical Clustering by Resampling. Front. Genet. 2016, 7, 144. [Google Scholar] [CrossRef]
- Tokuda, E.K.; Comin, C.H.; Costa, L.D.F. Revisiting agglomerative clustering. Phys. A Stat. Mech. Appl. 2022, 585, 126433. [Google Scholar] [CrossRef]
- Bruse, J.L.; Zuluaga, M.A.; Khushnood, A.; McLeod, K.; Ntsinjana, H.N.; Hsia, T.Y.; Sermesant, M.; Pennec, X.; Taylor, A.M.; Schievano, S. Detecting Clinically Meaningful Shape Clusters in Medical Image Data: Metrics Analysis for Hierarchical Clustering Applied to Healthy and Pathological Aortic Arches. IEEE Trans. Biomed. Eng. 2017, 64, 2373–2383. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, Y.P.; Cavanaugh, S.M.; Sandhu, A.A. Surgical aortic valve replacement in small aortic annulus. J. Card. Surg. 2021, 36, 2502–2509. [Google Scholar] [CrossRef] [PubMed]
- Ervoort, D.; El-Hamamsy, I.; Chu, M.W.A.; Peterson, M.D.; Ouzounian, M. The Ross Procedure and Valve-sparing Root Replacement Procedures in the Adult Patient: Do Guidelines Follow the Evidence? Ann. Cardiothorac. Surg. 2021, 10, 433–443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Unai, S.; Ozaki, S.; Johnston, D.R.; Saito, T.; Rajeswaran, J.; Svensson, L.G.; Blackstone, E.H.; Pettersson, G.B. Aortic Valve Reconstruction with Autologous Pericardium Versus a Bioprosthesis: The Ozaki Procedure in Perspective. J. Am. Heart. Assoc. 2023, 12, e027391. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bilkhu, R.; Jahangiri, M.; Otto, C.M. Patient-prosthesis mismatch following aortic valve replacement. Heart 2019, 105 (Suppl. S2), s28–s33. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Magne, J.; Leipsic, J.; Côté, N.; Blanke, P.; Thourani, V.H.; Hahn, R. Imaging for Predicting and Assessing Prosthesis-Patient Mismatch After Aortic Valve Replacement. JACC Cardiovasc. Imaging 2019, 12, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Fallon, J.M.; DeSimone, J.P.; Brennan, J.M.; O’Brien, S.; Thibault, D.P.; DiScipio, A.W.; Pibarot, P.; Jacobs, J.P.; Malenka, D.J. The Incidence and Consequence of Prosthesis-Patient Mismatch After Surgical Aortic Valve Replacement. Ann. Thorac. Surg. 2018, 106, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Dumesnil, J.G. Valve prosthesis-patient mismatch, 1978 to 2011: From original concept to compelling evidence. J. Am. Coll. Cardiol. 2012, 60, 1136–1139. [Google Scholar] [CrossRef]
- Stoica, S.; Beard, C.; Takkenberg, J.J.M.; Mokhles, M.M.; Turner, M.; Pepper, J.; Hopewell-Kelly, N.; Benedetto, U.; Nashef, S.A.M.; El-Hamamsy, I.; et al. Formal Consensus Study on Surgery to Replace the Aortic Valve in Adults Aged 18–60 Years. Heart. 2023, 109, 857–865. [Google Scholar] [CrossRef]
- Bruse, J.L.; McLeod, K.; Biglino, G.; Ntsinjana, H.N.; Capelli, C.; Hsia, T.Y.; Sermesant, M.; Pennec, X.; Taylor, A.M. A statistical shape modelling framework to extract 3D shape biomarkers from medical imaging data: Assessing arch morphology of repaired coarctation of the aorta. BMC Med. Imaging 2016, 16, 40. [Google Scholar] [CrossRef] [PubMed]
- Mansi, T.; Voigt, I.; Leonardi, B.; Pennec, X.; Durrleman, S.; Sermesant, M.; Delingette, H.; Taylor, A.M.; Boudjemline, Y.; Pongiglione, G. A Statistical Model for Quantification and Prediction of Cardiac Remodelling: Application to Tetralogy of Fallot. IEEE Trans. Med. Imaging 2011, 30, 1605–1616. [Google Scholar] [CrossRef] [PubMed]
- Müllner, D. Modern hierarchical, agglomerative clustering algorithms. arXiv 2011, arXiv:1109.2378. [Google Scholar]
- Sasirekha, K.; Baby, P. Agglomerative Hierarchical Clustering Algorithm—A Review. Int. J. Sci. Res. Publ. 2013, 3, 3. [Google Scholar]
- Xu, R.; Wunsch, D. Survey of clustering algorithms. IEEE Trans. Neural Netw. 2005, 16, 645–678. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, F.; Contreras, P. Algorithms for hierarchical clustering: An overview, II. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2017, 7, e1219. [Google Scholar] [CrossRef]
- Kaushik, M.; Mathur, B. Comparative Study of K-Means and Hierarchical Clustering Techniques. Int. J. Softw. Hardw. Res. Eng. 2014, 2, 93–98. [Google Scholar]
- Jayanti, S.; Kalyanaraman, Y.; Ramani, K. Shape-based clustering for 3D CAD objects: A comparative study of effectiveness. Comput.-Aided Des. 2009, 41, 999–1007. [Google Scholar] [CrossRef]
- Gundelwein, L.; Ramm, H.; Goubergrits, L.; Kelm, M.; Lamecker, H. 3D Shape Analysis for Coarctation of the Aorta. In Shape in Medical Imaging; Springer: Berlin/Heidelberg, Germany, 2018; pp. 111–119. [Google Scholar] [CrossRef]
- Cabezas, L.M.; Izbicki, R.; Stern, R.B. Hierarchical Clustering: Visualization, Feature Importance and Model Selection. Appl. Soft Comput. 2023, 141, 110303. Available online: https://www.sciencedirect.com/science/article/pii/S1568494623003216 (accessed on 20 November 2023). [CrossRef]
- Lance, G.N.; Williams, W.T. A General Theory of Classificatory Sorting Strategies: 1. Hierarchical Systems. Comput. J. 1967, 9, 373–380. [Google Scholar] [CrossRef]
- Sophocleous, F.; Bône, A.; Shearn, A.I.U.; Forte, M.N.V.; Bruse, J.L.; Caputo, M.; Biglino, G. Feasibility of a Longitudinal Statistical Atlas Model to Study Aortic Growth in Congenital Heart Disease. Comput. Biol. Med. 2022, 144, 105326. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Linkage Method | Description | Distance Metric | Description | Distance Equation |
|---|---|---|---|---|
| Single | The objects are grouped in one cluster depending on the two closest objects within the clusters. Produces long clusters. | Euclidean | Based on the Pythagoras theorem formula and is used when data are continuous and have normal distribution. High values will be clustered together, and low values will be clustered together. | |
| Complete | The opposite of single; the objects are grouped based on the furthest objects within the clusters. Produces compact spherical clusters. | Manhattan | It measures by summing the absolute differences of the coordinates of two objects. | |
| Average | This is based on the average distance of the objects within the clusters. | Correlation | Based on the correlation coefficient. Most common is the Pearson parametric correlation. Sensitive to outliers. | |
| Centroid | The objects are grouped in a cluster based on the distance between the objects that are in the centre of the cluster. | Mahalanobois | Takes normalisation of data into account and is based on t-score. | where S is the covariance matrix of the distribution, µ is the mean of vector of the distribution, and is the transpose of the difference vector. |
| Ward | The objects are grouped based on the minimal increase in sum-of squares. Minimises the variance within each cluster. | Cosine | Measures cosine angle between two vectors. | where A and B are vectors and are the magnitudes of the vectors (sum of squares). |
| McQuitty/Weighted (WPGMA) | Based on the average distance between clusters but does not take number of points in the clusters into consideration. |
| Pre-Operative Patient Characteristics | ||||
|---|---|---|---|---|
| Variable | AVR (n = 15) | Ozaki (n = 15) | Ross (n = 13) | VS (n = 4) |
| Sex | 12 m; 3 f | 12 m; 3 f | 3 m; 10 f | 3 m; 1 f |
| Age (years; mean ± SD) | 46.0 ± 19.0 | 51.0 ± 12.0 | 31.0 ± 11.0 | 56.0 ± 7.0 |
| Height (cm) | 174.7 ± 6.4 | 176.3 ± 10.9 | 167.0 ± 9.5 | 174.3 ± 9.0 |
| Weight (kg) | 81.8 ± 16.6 | 88.0 ± 18.8 | 73.1 ± 15.9 | 78.3 ± 19.9 |
| BSA (m2) | 2.0 ± 0.2 | 2.0 ± 0.2 | 1.9 ± 0.2 | 1.9 ± 0.3 |
| BMI (kg/m2) | 26.9 ± 5.4 | 28.0 ± 5.6 | 26.2 ± 5.8 | 25.5 ± 3.9 |
| Valve Type | 8 BAV; 6 TAV | 10 BAV; 3 TAV | 10 BAV; 2 TAV | 2 TAV |
| Ascending Aorta Surface Area (mm2) | 10,989.0 ± 2711.0 | 13,421.0 ± 2726.0 | 9031.0 ± 2125.0 | 14,658.0 ± 3125.0 |
| Whole Aorta Surface Area (mm2) | 32,570.0 ± 7880.0 | 29,969.0 ± 6292.0 | 22,221.0 ± 4180.0 | 34,841.0 ± 6151.0 |
| Post-Operative Patient Characteristics | ||||
| Variable | AVR (n = 12) | Ozaki (n = 10) | Ross (n = 10) | VS (n = 3) |
| Sex (M, F) | 12 m; 0 f | 6 m; 4 f | 5 m; 5 f | 2 m; 1 f |
| Age (years, mean ± SD) | 49.5 ± 17.2 | 49.9 ± 10.8 | 31 ± 14.2 | 47.3 ± 27.3 |
| Height (cm) | 177.8 ± 4.7 | 173.4 ± 13.2 | 163.6 ± 10.1 | 184 ± 7.1 |
| Weight (kg) | 85.2 ± 16.7 | 85.8 ± 21.4 | 76.3 ± 15.9 | 75.5 ± 16.3 |
| BSA (m2) | 2.0 ± 0.2 | 2.0 ± 0.3 | 1.8 ± 0.2 | 2.0 ± 0.2 |
| BMI (kg/m2) | 26.8 ± 4.7 | 28.6 ± 7.1 | 29.2 ± 9.0 | 22.6 ± 6.6 |
| Valve Type | 5 BAV; 2 TAV | 7 BAV; 2 TAV | 3 BAV; 4 TAV | 2 TAV |
| Ascending Aorta Surface Area (mm2) | 10,794.0 ± 1977.0 | 9695.0 ± 1640.0 | 8029.0 ± 2118.0 | 9212.0 ± 1761.0 |
| Whole Aorta Surface Area (mm2) | 27,336.0 ± 6239.0 | 27,011.0 ± 4747.0 | 20,409.0 ± 4460.0 | 30,233.0 ± 11,028.0 |
| Templates | Aortic Root Diameter | Mid-Ascending Aorta Diameter | Distal Ascending Aorta Diameter |
|---|---|---|---|
| Pre-operative Ascending Aorta | 36.19 mm | 39.48 mm | 36.57 mm |
| Pre-operative Whole Aorta | 36.19 mm | 39.53 mm | 35.68 mm |
| Post-operative Ascending Aorta | 34.85 mm | 32.19 mm | 32.80 mm |
| Post-operative Whole Aorta | 33.60 mm | 33.56 mm | 33.36 mm |
| Pre-Operative Analysis | ||||
|---|---|---|---|---|
| Scenario | Mode 1 | Mode 2 | Mode 3 | Mode 4 |
| Cumulative Inertia—Ascending Aorta (Contribution) | 24% (24%) | 36% (12%) | 47% (11%) | 57% (10%) |
| Cumulative Inertia—Whole Aorta (Contribution) | 27% (27%) | 38% (11%) | 47% (9%) | 55% (8%) |
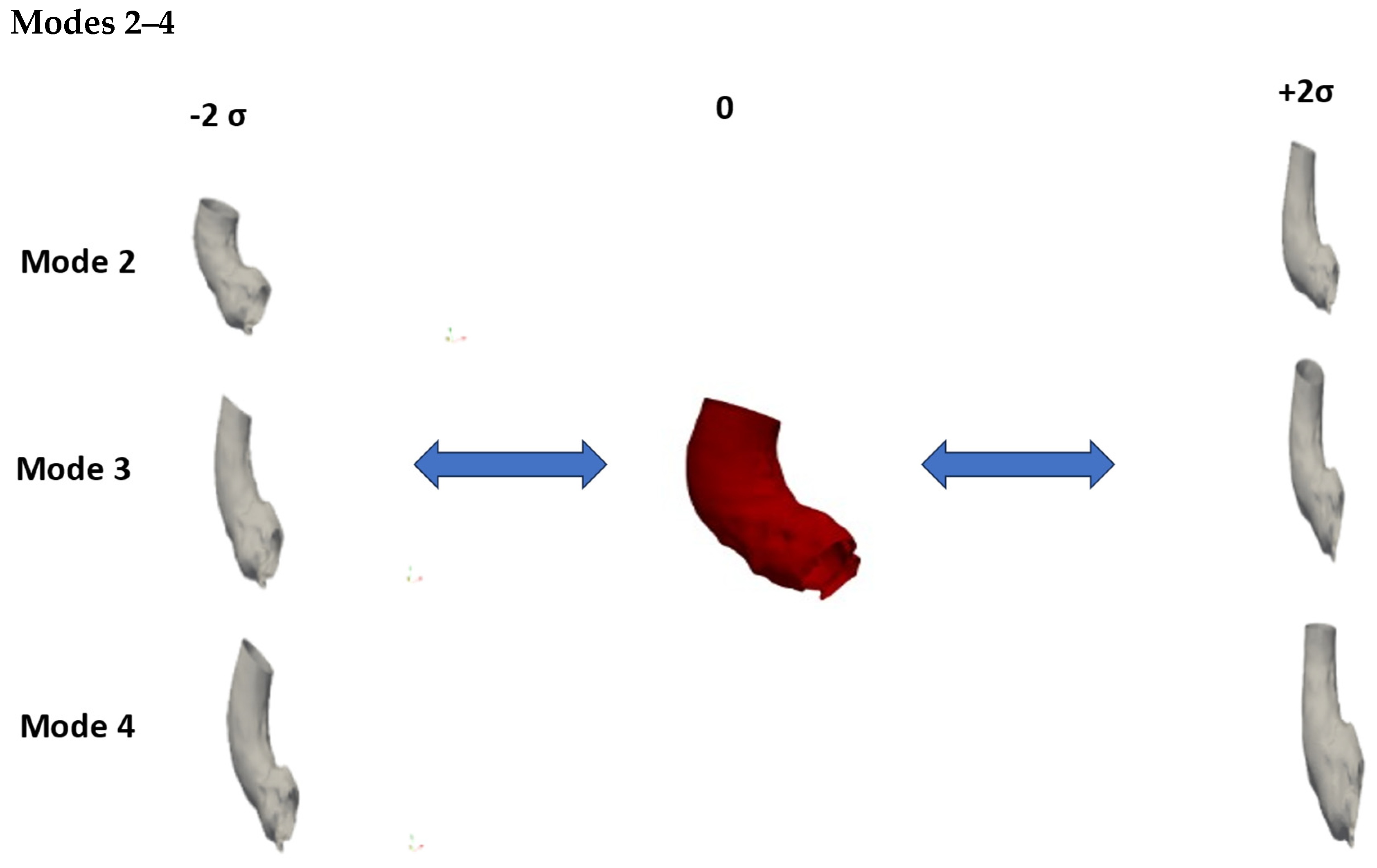
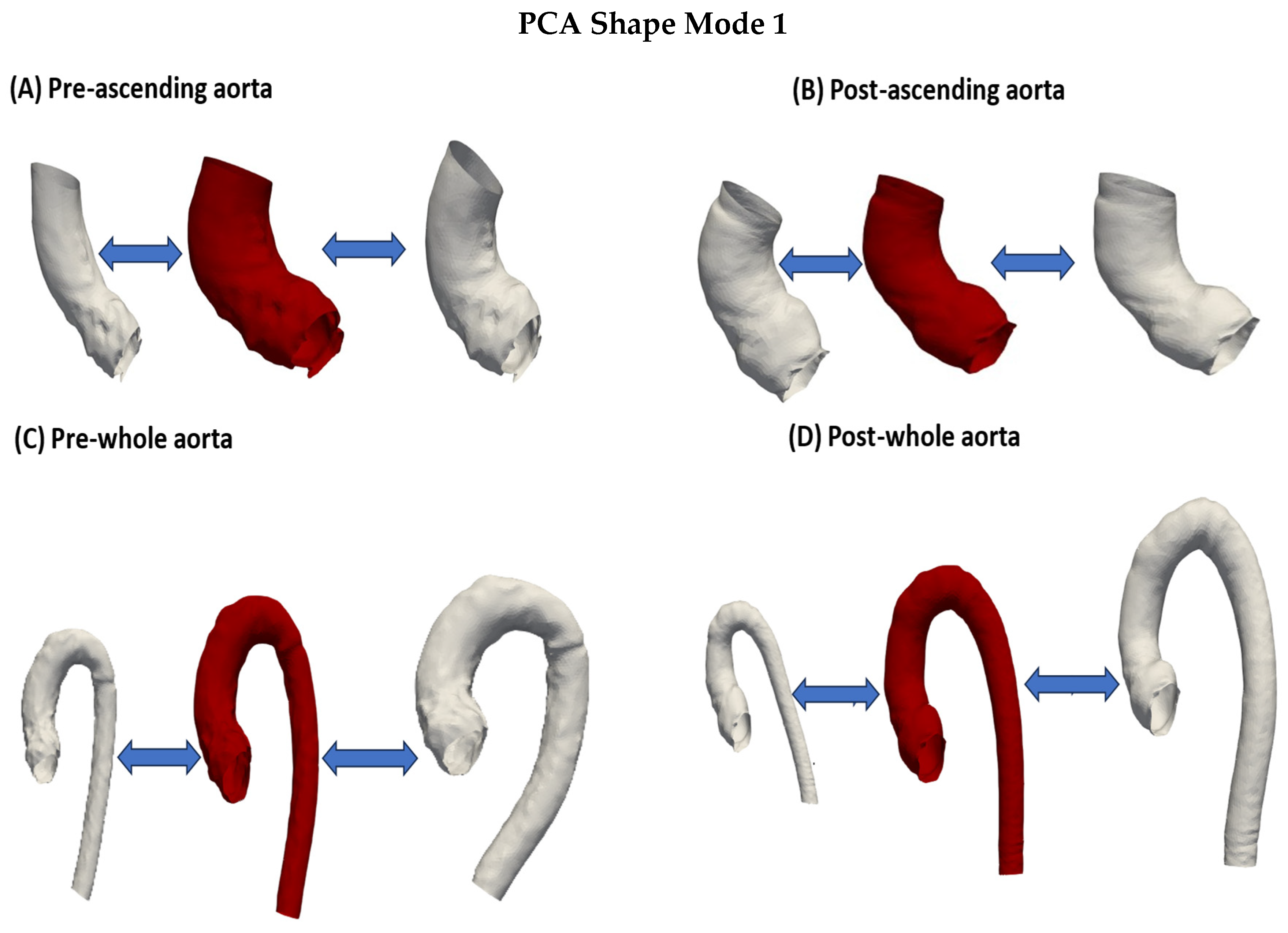
| Ascending Aorta Shape features | Small and thin > large and dilated | Wide aortic root > elongated segment proximal to aortic arch | Thin and long section proximal to aortic arch > wide and short aorta and narrow sinus | Narrow aortic root and long aorta > wide aortic root and short aorta |
| Whole Aorta Shape | Small > large and dilated, curved descending aorta | ‘Hook-like’ appearance > tortuous + dilated descending aorta | Dilated ascending > thin ascending aorta | Long and narrow aorta, gothic arch > short and dilated aorta, crenel arch |
| Post-Operative Analysis | ||||
| Scenario | Mode 1 | Mode 2 | Mode 3 | Mode 4 |
| Cumulative Inertia—Ascending Aorta (Contribution) | 24% (24%) | 36.3% (12.3%) | 46% (9.7%) | 54.6% (8.6%) |
| Cumulative Inertia—Whole Aorta (Contribution) | 25.6% (25.6%) | 36.6% (11%) | 46.6% (10%) | 54.6% (8%) |
| Ascending Aorta Shape | Small > large | Curved, slightly long > less curvature, short, dilated | Curved and dilated > slightly narrower | Dilated and curved > thinner |
| Whole Aorta Shape | Small > large, tortuous descending aorta | Dilated and long ascending, short descending, tortuous > short ascending, long descending aorta | Long ascending, short and wide descending > short ascending, long descending | Curved aorta, wide aortic root > long and straight descending, thin aortic root, wide ascending aorta |
| Ascending Aortas | ||||||
|---|---|---|---|---|---|---|
| Group | Cluster I | Cluster II | Cluster III | Cluster IV | Total | |
| AVR | 3 | 0 | 8 | 4 | 15 | |
| Ozaki | 2 | 5 | 4 | 4 | 15 | |
| Ross | 0 | 12 | 0 | 1 | 13 | |
| VS | 1 | 0 | 1 | 2 | 4 | |
| Total | 6 | 17 | 13 | 11 | 47 | |
| Whole Aortas | ||||||
| Group | Cluster I | Cluster II | Cluster III | Cluster IV | Cluster V | |
| AVR | 3 | 2 | 3 | 4 | 2 | 14 |
| Ozaki | 6 | 1 | 1 | 4 | 3 | 15 |
| Ross | 2 | 1 | 0 | 0 | 10 | 13 |
| VS | 1 | 0 | 1 | 2 | 0 | 4 |
| Total | 12 | 4 | 5 | 10 | 15 | 46 |
| Ascending Aortas | ||||||
|---|---|---|---|---|---|---|
| Group | Cluster I | Cluster II | Cluster III | Total | ||
| AVR | 4 | 5 | 3 | 12 | ||
| Ozaki | 2 | 2 | 6 | 10 | ||
| Ross | 3 | 1 | 6 | 10 | ||
| VS | 1 | 0 | 2 | 3 | ||
| Total | 10 | 8 | 17 | 35 | ||
| Whole Aortas | ||||||
| Group | Cluster I | Cluster II | Cluster III | Cluster IV | Cluster V | Total |
| AVR | 2 | 5 | 1 | 2 | 2 | 12 |
| Ozaki | 1 | 2 | 4 | 1 | 2 | 10 |
| Ross | 1 | 8 | 0 | 1 | 0 | 10 |
| VS | 0 | 2 | 1 | 0 | 0 | 3 |
| Total | 4 | 17 | 6 | 4 | 4 | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljassam, Y.; Sophocleous, F.; Bruse, J.L.; Schot, V.; Caputo, M.; Biglino, G. Machine Learning and Statistical Shape Modelling Methodologies to Assess Vascular Morphology before and after Aortic Valve Replacement. J. Clin. Med. 2024, 13, 4577. https://doi.org/10.3390/jcm13154577
Aljassam Y, Sophocleous F, Bruse JL, Schot V, Caputo M, Biglino G. Machine Learning and Statistical Shape Modelling Methodologies to Assess Vascular Morphology before and after Aortic Valve Replacement. Journal of Clinical Medicine. 2024; 13(15):4577. https://doi.org/10.3390/jcm13154577
Chicago/Turabian StyleAljassam, Yousef, Froso Sophocleous, Jan L. Bruse, Vico Schot, Massimo Caputo, and Giovanni Biglino. 2024. "Machine Learning and Statistical Shape Modelling Methodologies to Assess Vascular Morphology before and after Aortic Valve Replacement" Journal of Clinical Medicine 13, no. 15: 4577. https://doi.org/10.3390/jcm13154577