
Symptoms, Course, and Factors Related to Long-Term Morbidity, Including Differences between Infection Strains, in Patients with Long COVID in a Primary Care Clinic in Japan: An Observational Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Subjects
2.3. Clinical Parameters
2.4. Symptoms
2.5. Assessment of Patients Who Achieved Remission of Symptoms
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Patients
3.2. Long COVID Symptom Distribution
3.3. Outcomes in the Long COVID Patients Who Visited Our Clinic
3.4. Analysis of Patients Who Achieved Remission of Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Institute for Health and Care Excellence (NICE). COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. 2020 (published_guideline_6038-1_14). Available online: http://www.nice.org.uk/guidance/NG188 (accessed on 20 February 2021).
- World Health Organization. Post COVID-19 Condition (Long COVID). 2021. Reference Number: WHO/2019-nCoV/Post COVID-19 Condition/Clinical Case Definition/2021.1. Available online: http://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 31 October 2021).
- Antonelli, M.; Pujol, J.C.; Spector, T.D.; Ourselin, S.; Steves, C.J. Risk of long COVID associated with delta versus omicron variants of SARS-CoV-2. Lancet 2022, 399, 2263–2264. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 8, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-term sequelae of COVID-19: A systematic review and meta-analysis of one-year follow-up studies on post-COVID symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major findings, mechanisms and recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Choi, T.; Al-Aly, Z. Postacute sequelae of SARS-CoV-2 infection in the pre-Delta, Delta, and Omicron eras. New Engl. J. Med. 2024, 391, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Bahmer, T.; Borzikowsky, C.; Lieb, W.; Horn, A.; Krist, L.; Fricke, J.; Scheibenbogen, C.; Rabe, K.F.; Maetzler, W.; Maetzler, C.; et al. Severity, predictors and clinical correlates of Post-COVID syndrome (PCS) in Germany: A prospective, multi-centre, population-based cohort study. EClinicalMedicine 2022, 51, 101549. [Google Scholar] [CrossRef] [PubMed]
- van Kessel, S.A.M.; Olde Hartman, T.C.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–567. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, T.; Yoshimura, N.; Ishizuka, K.; Katayama, K.; Inoue, Y.; Hirose, M.; Nakagama, Y.; Kido, Y.; Sugimori, H.; Matsuda, T.; et al. Five cluster classifications of long COVID and their background factors: A cross-sectional study in Japan. Clin. Exp. Med. 2023, 23, 3663–3670. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan. Japanese Outbreak Trend of COVID-19. 2023. Available online: http://www.mhlw.go.jp/content/10906000/001094012.pdf (accessed on 1 September 2023).
- National Institute of Infectious Diseases, Japan. Detection of New Coronaviruses by Strain through Genome Surveillance. Available online: http://www.niid.go.jp/niid/images/cepr/covid-19/20221228_genome_surveillance.pdf (accessed on 1 September 2023).
- Ministry of Health, Labour and Welfare, Japan. Manual of Medical Treatment for COVID-19 Ver.10.0. Available online: https://www.mhlw.go.jp/content/001136687.pdf (accessed on 31 August 2023). (In Japanese)
- Ministry of Health, Labour and Welfare, Japan. Management of Post-COVID Condition Ver. 3.0. Available online: https://www.mhlw.go.jp/content/10900000/001159305.pdf (accessed on 31 October 2023). (In Japanese)
- Fukuda, S.; Takashima, S.; Iwase, M.; Yamaguti, K.; Kuratsune, H.; Watanabe, Y. Development and validation of a new fatigue scale for fatigued subjects with and without chronic fatigue syndrome. In Fatigue Science for Human Health; Watanabe, Y., Evengård, B., Natelson, B.H., Jason, L.A., Kuratsune, H., Eds.; Springer: Tokyo, Japan, 2008; pp. 89–102. [Google Scholar]
- Du, M.; Ma, Y.; Deng, J.; Liu, M.; Liu, J. Comparison of long COVID-19 caused by different SARS-CoV-2 strains: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2022, 19, 16010. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, K.; Kristoffersen, D.T.; Dell’Isola, A.; Kiadaliri, A.; Turkiewicz, A.; Runhaar, J.; Bierma-Zeinstra, S.; Englund, M.; Magnus, P.M.; Kinge, J.M.; et al. Post-COVID medical complaints following infection with SARS-CoV-2 Omicron vs Delta variants. Nat Commun. 2022, 13, 7363. [Google Scholar] [CrossRef] [PubMed]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and outcomes of hospitalized patients in South Africa during the COVID-19 Omicron wave compared with previous waves. JAMA 2022, 327, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Stehlik, P.; Clark, J.; Alcorn, K.; Glasziou, P. Effect of covid-19 vaccination on long covid: Systematic review. BMJ Med. 2023, 2, e000385. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Iwagami, M.; Yasuhara, J.; Takagi, H.; Kuno, T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Vimercati, L.; De Maria, L.; Quarato, M.; Caputi, A.; Gesualdo, L.; Migliore, G.; Cavone, D.; Sponselli, S.; Pipoli, A.; Inchingolo, F.; et al. Association between long COVID and overweight/obesity. J. Clin. Med. 2021, 10, 4143. [Google Scholar] [CrossRef] [PubMed]
- Ando, W.; Horii, T.; Uematsu, T.; Hanaki, H.; Atsuda, K.; Otori, K. Impact of overlapping risks of type 2 diabetes and obesity on coronavirus disease severity in the United States. Sci. Rep. 2021, 11, 17968. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, T.; Oba, S.; Komiya, Y.; Kawata, D.; Kamiya, M.; Iwai, H.; Miyamoto, S.; Kataoka, M.; Tobiume, M.; Kanno, T.; et al. Apple-shaped obesity: A risky soil for cytokine-accelerated severity in COVID-19. Proc. Natl. Acad. Sci. USA 2023, 120, e2300155120. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L.; Lipkin, W.I. ME/CFS and long COVID share similar symptoms and biological abnormalities: Road map to the literature. Front. Med. 2023, 10, 118763. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Delta and Before (n = 498) | Omicron (n = 555) | ||
|---|---|---|---|
| Male/Female (%) | 47.4/53.6 | 47.3/53.7 | N.S. * |
| Age (years) | 41.9 (15–87) | 41.0 (15–89) | N.S. * |
| BMI (kg/m2) | 22.2 (14.9–54.4) | 21.9 (14.1–45.8) | N.S. * |
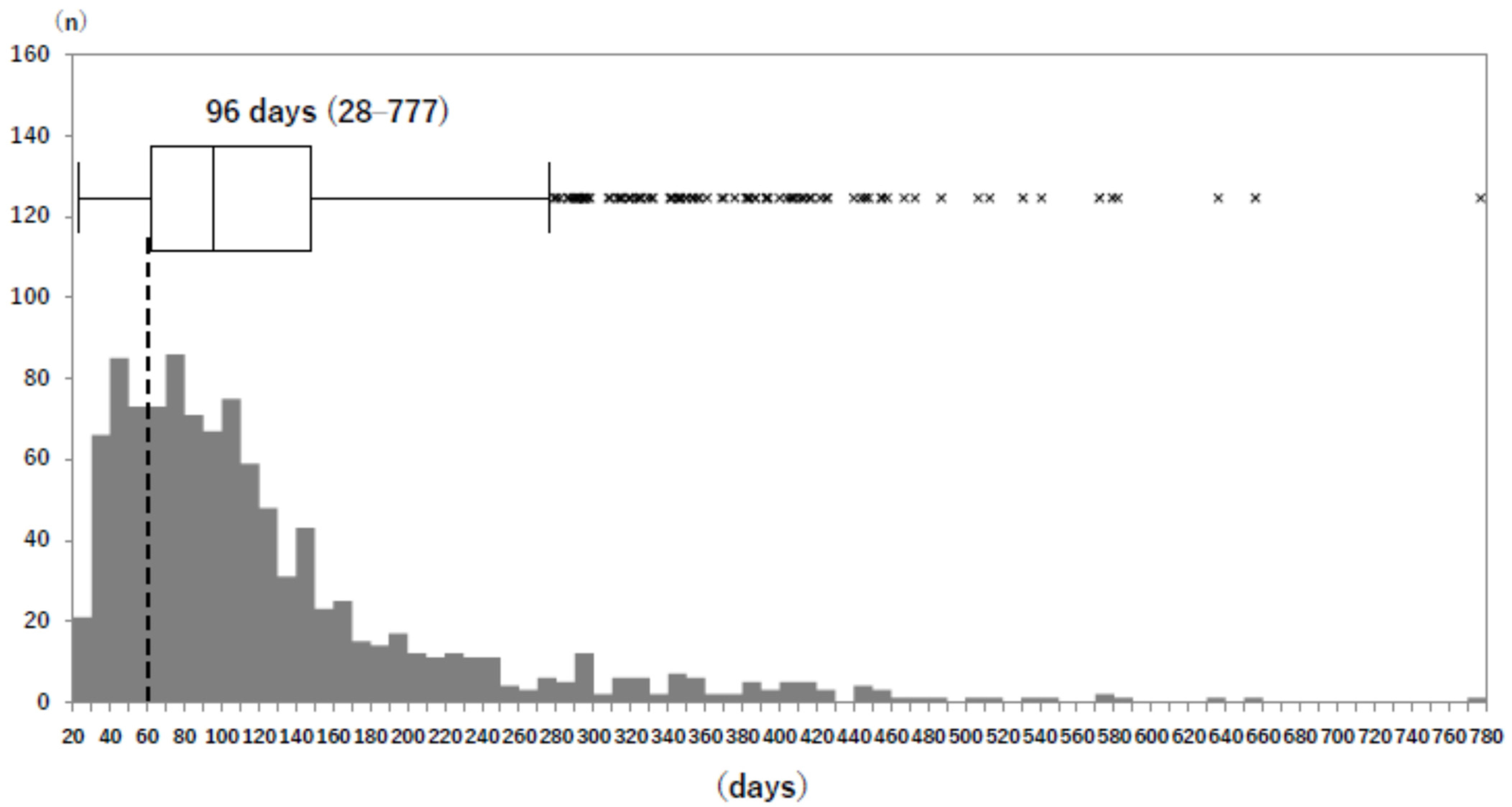
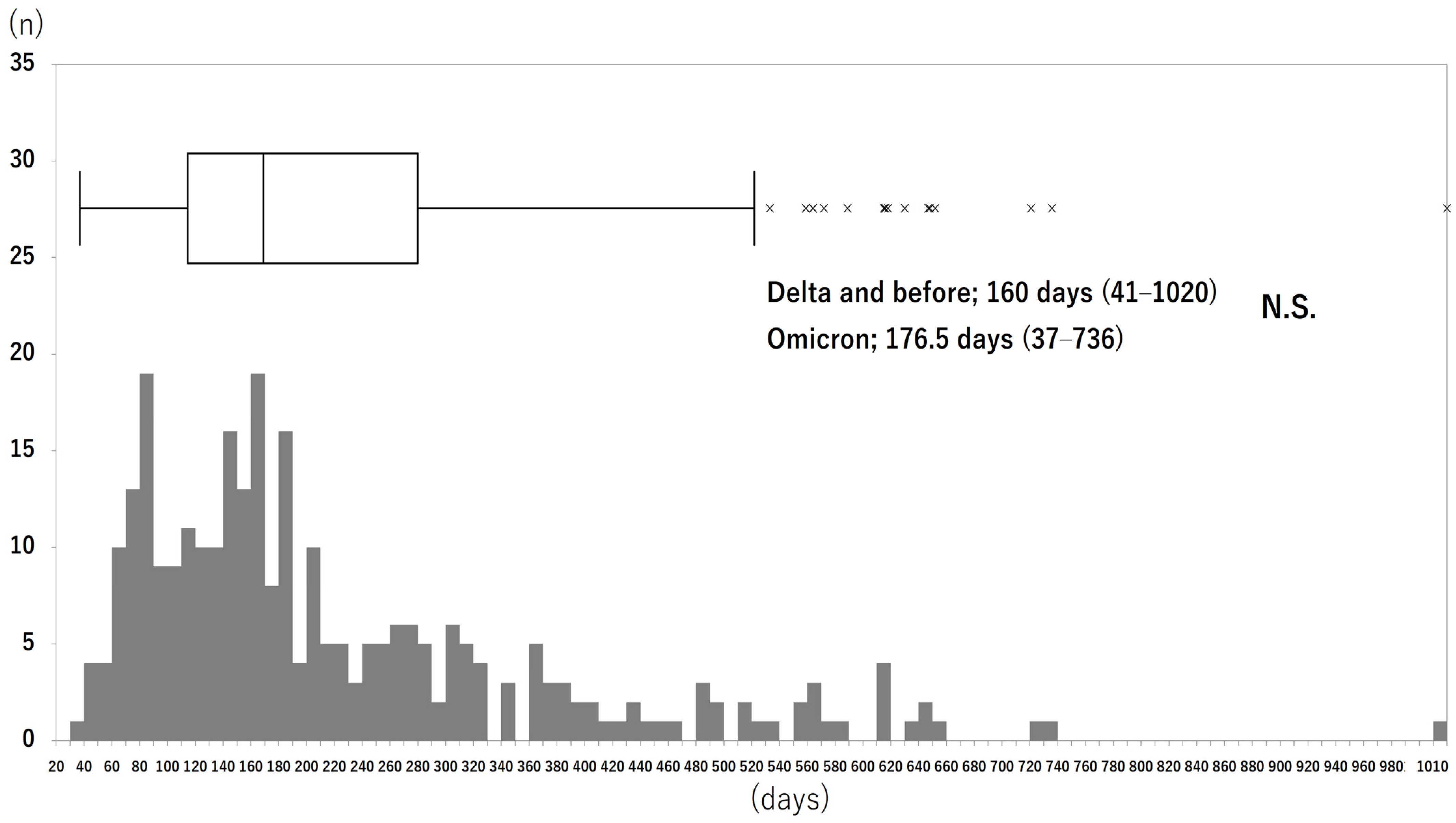
| Period (days) until visiting long COVID outpatient clinic after onset of COVID-19 ** | 101 (28–777) | 95 (28–448) | N.S. * |
| Severity of COVID-19: mild/moderate I/moderate II/severe (%) | 82.2/6.6/8.3/2.9 (n = 484) | 97.6/0.7/1.3/0.4 (n = 536) | p < 0.001 ** |
| Vaccination Y/N (%) | 37.1/67.9 (n = 467) | 73.1/26.9 (n = 554) | p < 0.001 ** |
| Performance status: 1/2/3/4/5/6/7/8/9 (%) | 38.1/30.5/5.8/4.7/1.6/ 2.7/12.8/3.5/0.4 (n = 485) | 16.9/34.1/5.2/4.5/6.2/ 3.0/22.7/6.4/1.1 (n = 534) | p < 0.001 ** |
| Covariate | Level | Hazard Ratio (95%CI) | |
|---|---|---|---|
| Infectious strain | Omicron/Delta and before | 0.875 (0.623–1.228) | N.S. |
| Sex | F/M | 0.728 (0.542–0.977) | p = 0.0341 |
| Age | Years | 0.998 (0.989–1.008) | N.S. |
| Vaccination | Y/N | 1.095 (0.815–1.471) | N.S. |
| BMI | 0.959 (0.929–0.989) | p = 0.0072 | |
| Performance status | 1.037 (0.978–1.099) | N.S. | |
| Fatigue | Y/N | 0.951 (0.716–1.262) | N.S. |
| Fever | Y/N | 0.867 (0.570–1.318) | N.S. |
| Insomnia | Y/N | 1.557 (1.048–2.313) | p = 0.0284 |
| Dyspnea | Y/N | 0.741 (0.552–0.996) | p = 0.0468 |
| Cough | Y/N | 2.295 (1.682–3.132) | p < 0.001 |
| Brain fog | Y/N | 0.780 (0.542–1.123) | N.S. |
| Depression/anxiety | Y/N | 0.962 (0.615–1.506) | N.S. |
| Headache | Y/N | 0.814 (0.576–1.150) | N.S. |
| Chest pain/discomfort | Y/N | 0.861 (0.578–1.284) | N.S. |
| Throat pain/discomfort | Y/N | 1.209 (0.797–1.833) | N.S. |
| Anosmia | Y/N | 1.184 (0.772–1.817) | N.S. |
| Ageusia | Y/N | 0.826 (0.613–1.327) | N.S. |
| Dizziness/auditory disorder | Y/N | 1.099 (0.698–1.729) | N.S. |
| Loss of hair | Y/N | 1.103 (0.674–1.804) | N.S. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baba, K.; Kawai, S.; Iwase, S.; Ushida, T.; Tamura, Y.; Arimoto, M.; Nojiri, M.; Watanabe, D.; Ban, N. Symptoms, Course, and Factors Related to Long-Term Morbidity, Including Differences between Infection Strains, in Patients with Long COVID in a Primary Care Clinic in Japan: An Observational Study. J. Clin. Med. 2024, 13, 5019. https://doi.org/10.3390/jcm13175019
Baba K, Kawai S, Iwase S, Ushida T, Tamura Y, Arimoto M, Nojiri M, Watanabe D, Ban N. Symptoms, Course, and Factors Related to Long-Term Morbidity, Including Differences between Infection Strains, in Patients with Long COVID in a Primary Care Clinic in Japan: An Observational Study. Journal of Clinical Medicine. 2024; 13(17):5019. https://doi.org/10.3390/jcm13175019
Chicago/Turabian StyleBaba, Kenji, Seiko Kawai, Satoshi Iwase, Takahiro Ushida, Yasuhiro Tamura, Mariko Arimoto, Makiko Nojiri, Daisuke Watanabe, and Nobutaro Ban. 2024. "Symptoms, Course, and Factors Related to Long-Term Morbidity, Including Differences between Infection Strains, in Patients with Long COVID in a Primary Care Clinic in Japan: An Observational Study" Journal of Clinical Medicine 13, no. 17: 5019. https://doi.org/10.3390/jcm13175019