
A Pilot Study of Saliva MicroRNA Signatures in Children with Moderate-to-Severe Traumatic Brain Injury

Abstract
:1. Introduction
2. Materials and Methods
3. Results
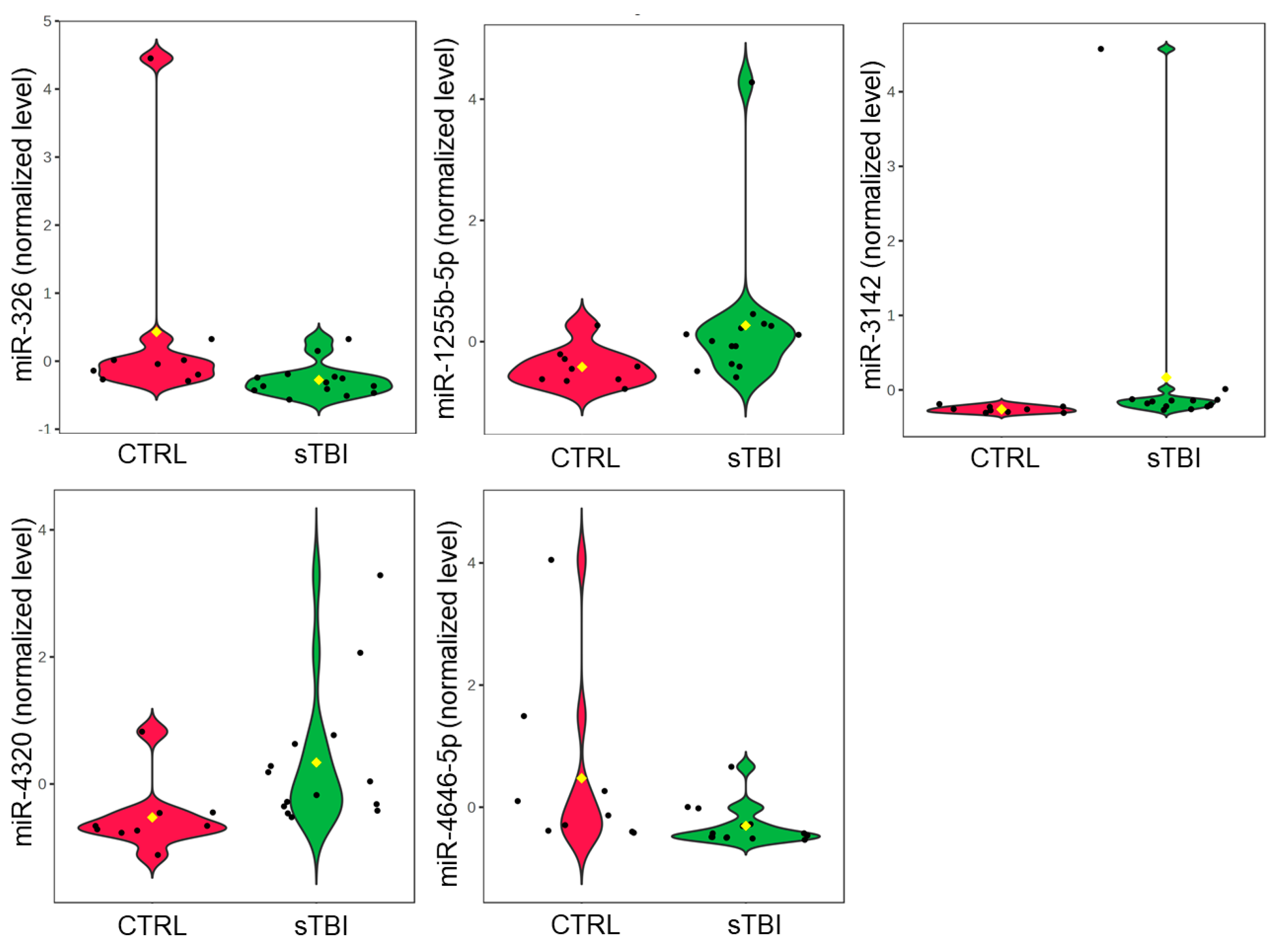
3.1. sTBI vs. Control Group
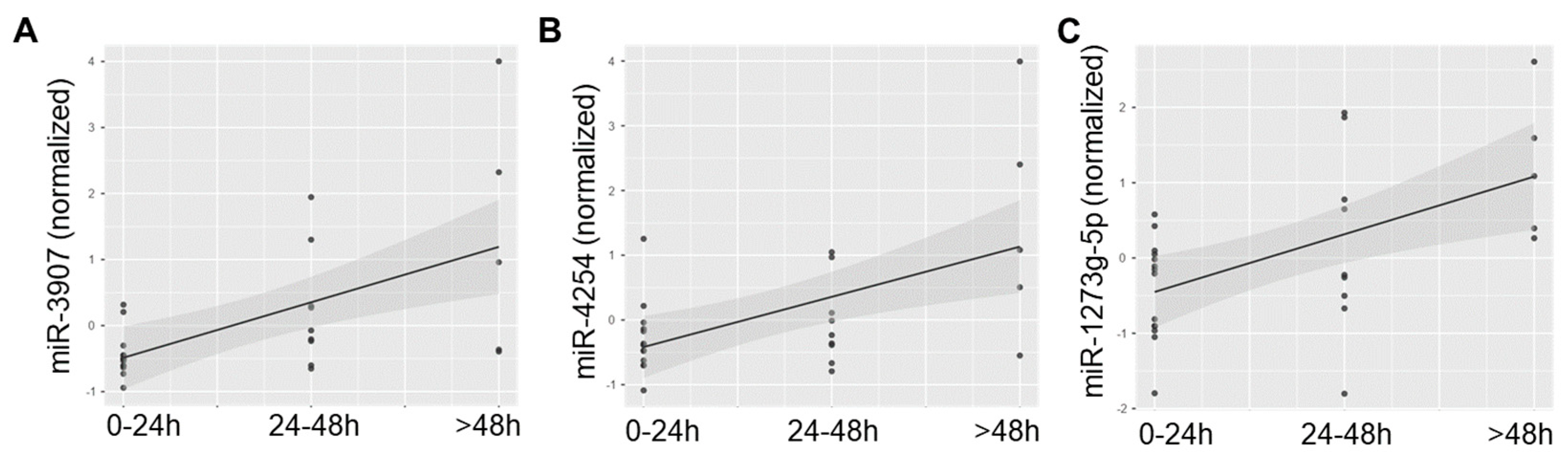
3.2. sTBI Patients over Time
3.3. Pathway Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Traumatic Brain Injury & Concussion. 2024. Available online: https://www.cdc.gov/traumatic-brain-injury/data-research/facts-stats/index.html (accessed on 24 May 2024).
- Coronado, V.G.; Xu, L.; Basavaraju, S.V.; Wald, M.M.; Faul, M.D.; Guzman, B.R.; Hemphill, J.D. Surveillance for Traumatic Brain Injury–Related Deaths—United States, 1997–2007. Center for Disease Control and Prevention. 2011. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss6005a1.htm#Tab14 (accessed on 24 May 2024).
- Rivara, F.P.; Koepsell, T.D.; Wang, J.; Temkin, N.; Dorsch, A.; Vavilala, M.S.; Durbin, D.; Jaffe, K.M. Incidence of Disability Among Children 12 Months After Traumatic Brain Injury. Am. J. Public Health 2012, 102, 2074–2079. [Google Scholar] [CrossRef] [PubMed]
- Gilad, S.; Meiri, E.; Yogev, Y.; Benjamin, S.; Lebanony, D.; Yerushalmi, N.; Chajut, A. Serum MicroRNAs Are Promising Novel Biomarkers. PLoS ONE 2008, 3, e3148. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.J.; Lim, J.W.; Moritz, R.L.; Mathivanan, S. Exosomes: Proteomic insights and diagnostic potential. Expert Rev. Proteom. 2009, 6, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Valadi, H.; Ekström, K.; Bossios, A.; Sjöstrand, M.; Lee, J.J.; Lötvall, J.O. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef]
- Hicks, S.D.; Johnson, J.; Carney, M.C.; Bramley, H.; Olympia, R.P.; Loeffert, A.C.; Thomas, N.J. Overlapping MicroRNA Expression in Saliva and Cerebrospinal Fluid Accurately Identifies Pediatric Traumatic Brain Injury. J. Neurotrauma 2018, 35, 64–72. [Google Scholar] [CrossRef]
- Pasinetti, G.M.; Ho, L.; Dooley, C.; Abbi, B.; Lange, G. Select non-coding RNA in blood components provide novel clinically accessible biological surrogates for improved identification of traumatic brain injury in OEF/OIF Veterans. Am. J. Neurodegener. Dis. 2012, 1, 88. [Google Scholar]
- Redell, J.B.; Moore, A.N.; Ward, N.H., III; Hergenroeder, G.W.; Dash, P.K. Human traumatic brain injury alters plasma microRNA levels. J. Neurotrauma 2010, 27, 2147–2156. [Google Scholar] [CrossRef]
- Larocca, D.; Barns, S.; Hicks, S.D.; Brindle, A.; Williams, J.; Uhlig, R.; Johnson, P.; Neville, C.; Middleton, F.A. Comparison of serum and saliva miRNAs for identification and characterization of mTBI in adult mixed martial arts fighters. PLoS ONE 2019, 14, e0207785. [Google Scholar] [CrossRef]
- Hicks, S.D.; Onks, C.; Kim, R.Y.; Zhen, K.J.; Loeffert, J.; Loeffert, A.C.; Olympia, R.P.; Fedorchak, G.; DeVita, S.; Gagnon, Z.; et al. Refinement of saliva microRNA biomarkers for sports-related concussion. J. Sport Health Sci. 2023, 12, 369–378. [Google Scholar] [CrossRef]
- Di Pietro, V.; Porto, E.; Ragusa, M.; Barbagallo, C.; Davies, D.; Forcione, M.; Logan, A.; Di Pietro, C.; Purrello, M.; Grey, M.; et al. Salivary MicroRNAs: Diagnostic Markers of Mild Traumatic Brain Injury in Contact-Sport. Front. Mol. Neurosci. 2018, 11, 290. [Google Scholar] [CrossRef]
- Bhomia, M.; Balakathiresan, N.S.; Wang, K.K.; Papa, L.; Maheshwari, R.K. A panel of serum MiRNA biomarkers for the diagnosis of severe to mild traumatic brain injury in humans. Sci. Rep. 2016, 6, e28148. [Google Scholar] [CrossRef] [PubMed]
- Vos, P.E.; Jacobs, B.; Andriessen, T.M.; Lamers, K.J.; Borm, G.F.; Beems, T.; Edwards, M.; Rosmalen, C.F.; Vissers, J.L. GFAP and S100B are biomarkers of traumatic brain injury: An observational cohort study. Neurology 2010, 75, 1786–1793. [Google Scholar] [CrossRef] [PubMed]
- Abdelhak, A.; Foschi, M.; Abu-Rumeileh, S.; Yue, J.K.; D’Anna, L.; Huss, A.; Oeckl, P.; Ludolph, A.C.; Kuhle, J.; Petzold, A.; et al. Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat. Rev. Neurol. 2022, 18, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Cash, A.; Theus, M.H. Mechanisms of blood–brain barrier dysfunction in traumatic brain injury. Int. J. Mol. Sci. 2020, 21, 3344. [Google Scholar] [CrossRef]
- Bazarian, J.J.; Biberthaler, P.; Welch, R.D.; Lewis, L.M.; Barzo, P.; Bogner-Flatz, V.; Brolinson, P.G.; Büki, A.; Chen, J.Y.; Christenson, R.H.; et al. A.S. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): A multicentre observational study. Lancet Neurol. 2018, 17, 782–789. [Google Scholar] [CrossRef]
- Mannix, R.; Borglund, E.; Monashefsky, A.; Master, C.; Coewin, D.; Badawy, M.; Thomas, D.G.; Reisner, A. Age-Dependent Differences in Blood Levels of Glial Fibrillary Acidic Protein but Not Ubiquitin Carboxy-Terminal Hydrolase L1 in Children. Neurology 2024, 103, e209651. [Google Scholar] [CrossRef]
- Malec, J.F.; Brown, A.W.; Leibson, C.L.; Flaada, J.T.; Mandrekar, J.N.; Diehl, N.N.; Perkins, P.K. The mayo classification system for traumatic brain injury severity. J. Neurotrauma 2007, 24, 1417–1424. [Google Scholar] [CrossRef]
- Hicks, S.D.; Jacob, P.; Middleton, F.A.; Perez, O.; Gagnon, Z. Distance running alters peripheral microRNAs implicated in metabolism, fluid balance, and myosin regulation in a sex-specific manner. Physiol. Genom. 2018, 50, 658–667. [Google Scholar] [CrossRef]
- Vlachos, I.S.; Zagganas, K.; Paraskevopoulou, M.D.; Georgakilas, G.; Karagkouni, D.; Vergoulis, T.; Dalamagas, T.; Hatzigeorgiou, A.G. DIANA-miRPath v3. 0: Deciphering microRNA function with experimental support. Nucleic Acids Res. 2015, 43, W460–W466. [Google Scholar] [CrossRef]
- Morganti-Kossmann, M.C.; Hans, V.H.; Lenzlinger, P.M.; Dubs, R.; Ludwig, E.; Trentz, O.; Kossman, T. TGF-beta is elevated in the CSF of patients with severe traumatic brain injuries and parallels blood-brain barrier function. J. Neurotrauma 1999, 16, 617–628. [Google Scholar] [CrossRef]
- Di Pietro, V.; Ragusa, M.; Davies, D.; Su, Z.; Hazeldine, J.; Lazzarino, G.; Hill, L.J.; Crombie, N.; Foster, M.; Purrello, M.; et al. MicroRNAs as novel biomarkers for the diagnosis and prognosis of mild and severe traumatic brain injury. J. Neurotrauma 2017, 34, 1948–1956. [Google Scholar] [CrossRef]
- Mitra, B.; Rau, T.F.; Surendran, N.; Brennan, J.H.; Thaveenthiran, P.; Sorich, E.; Fitzgerald, M.C.; Rosenfeld, J.V.; Patel, S.A. Plasma micro-RNA biomarkers for diagnosis and prognosis after traumatic brain injury: A pilot study. J. Clin. Neurosci. 2017, 38, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Li, L.; Lv, Q.; Shu, Q.; Zhang, Y.; Wang, Y. Expression profile of plasma microRNAs and their roles in diagnosis of mild to severe traumatic brain injury. PLoS ONE 2018, 13, e0204051. [Google Scholar] [CrossRef] [PubMed]
- Ghaith, H.S.; Nawar, A.A.; Gabra, M.D.; Abdelrahman, M.E.; Nafady, M.H.; Bahbah, E.I.; Ebada, M.A.; Ashraf, G.M.; Negida, A.; Barreto, G.E. A literature review of traumatic brain injury biomarkers. Mol. Neurobiol. 2022, 59, 4141–4158. [Google Scholar] [CrossRef]
- McGinn, M.J.; Povlishock, J.T. Pathophysiology of traumatic brain injury. Neurosurg. Clin. 2016, 27, 397–407. [Google Scholar] [CrossRef]
- Capizzi, A.; Woo, J.; Verduzco-Gutierrez, M. Traumatic brain injury: An overview of epidemiology, pathophysiology, and medical management. Med. Clin. 2020, 104, 213–238. [Google Scholar]
- Wang, X.; Zhou, H.; Cheng, R.; Zhou, X.; Hou, X.; Chen, J.; Qiu, J. Role of miR-326 in neonatal hypoxic-ischemic brain damage pathogenesis through targeting of the δ-opioid receptor. Mol. Brain 2020, 13, 51. [Google Scholar] [CrossRef]
- Jadideslam, G.; Ansarin, K.; Sakhinia, E.; Babaloo, Z.; Abhari, A.; Ghahremanzadeh, K.; Khalili, M.; Radmehr, R.; Kabbazi, A. Diagnostic biomarker and therapeutic target applications of miR-326 in cancers: A systematic review. J. Cell. Physiol. 2019, 234, 21560–21574. [Google Scholar] [CrossRef]
- Honardoost, M.A.; Kiani-Esfahani, A.; Ghaedi, K.; Etemadifar, M.; Salehi, M. miR-326 and miR-26a, two potential markers for diagnosis of relapse and remission phases in patient with relapsing–remitting multiple sclerosis. Gene 2014, 544, 128–133. [Google Scholar] [CrossRef]
- Xu, X.; Iqbal, Z.; Xu, L.; Wen, C.; Duan, L.; Xia, J.; Yang, N.; Zhang, Y.; Liang, Y. Brain-derived extracellular vesicles: Potential diagnostic biomarkers for central nervous system diseases. Psychiatry Clin. Neurosci. 2024, 78, 83–96. [Google Scholar] [CrossRef]
- Saucier, D.; Wajnberg, G.; Roy, J.; Beauregard, A.-P.; Chacko, S.; Crapoulet, N.; Fournier, S.; Ghosh, A.; Lewis, S.M.; Marrero, A.; et al. Identification of a circulating miRNA signature in extracellular vesicles collected from amyotrophic lateral sclerosis patients. Brain Res. 2019, 1708, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Lai, N.S.; Zhang, J.Q.; Qin, F.Y.; Sheng, B.; Fang, X.G.; Li, Z.B. Serum microRNAs are non-invasive biomarkers for the presence and progression of subarachnoid haemorrhage. Biosci. Rep. 2017, 37, BSR20160480. [Google Scholar] [CrossRef]
- Gareev, I.; Beylerli, O.; Yang, G.; Izmailov, A.; Shi, H.; Sun, J.; Zhao, B.; Liu, B.; Zhao, S. Diagnostic and prognostic potential of circulating miRNAs for intracranial aneurysms. Neurosurg. Rev. 2021, 44, 2025–2039. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.B.; Chen, H.P.; Zhong, D.; Song, J.H.; Cao, J.W.; Zhao, M.Q.; Han, B.C.; Duan, Q.; Sheng, X.M.; Yao, J.L.; et al. LncRNA RMRP accelerates autophagy-mediated neurons apoptosis through miR-3142/TRIB3 signaling axis in alzheimer’s disease. Brain Res. 2022, 1785, 147884. [Google Scholar] [CrossRef] [PubMed]
- Sheng, X.; Yang, Y.; Liu, J.; Yu, J.; Guo, Q.; Guan, W.; Liu, F. Down-regulation of miR-18b-5p protects against splenic hemorrhagic shock by directly targeting HIF-1α/iNOS pathway. Immunobiology 2022, 227, 152188. [Google Scholar] [CrossRef]
- Grimes, J.A.; Robinson, K.R.; Bullington, A.M.; Schmiedt, J.M. Identification of serum microRNAs with differential expression between dogs with splenic masses and healthy dogs with histologically normal spleens. Am. J. Vet. Res. 2021, 82, 659–666. [Google Scholar] [CrossRef]
- Zacharewicz, E.; Lamon, S.; Russell, A.P. MicroRNAs in skeletal muscle and their regulation with exercise, ageing, and disease. Front. Physiol. 2013, 4, 266. [Google Scholar] [CrossRef]
- Li, Y.F.; Jing, Y.; Hao, J.; Frankfort, N.C.; Zhou, X.; Shen, B.; Liu, X.; Wang, L.; Li, R. MicroRNA-21 in the pathogenesis of acute kidney injury. Protein Cell 2013, 4, 813–819. [Google Scholar] [CrossRef]
- Ding, X.; Ding, J.; Ning, J.; Yi, F.; Chen, J.; Zhao, D.; Zheng, J.; Liang, Z.; Hu, Z.; Du, Q. Circulating microRNA-122 as a potential biomarker for liver injury. Mol. Med. Rep. 2012, 5, 1428–1432. [Google Scholar] [CrossRef]
- Sullivan, R.; Montgomery, A.; Scipioni, A.; Jhaveri, P.; Schmidt, A.T.; Hicks, S.D. Confounding Factors Impacting microRNA Expression in Human Saliva: Methodological and Biological Considerations. Genes 2022, 13, 1874. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 23) | sTBI Group (n = 14) | Control Group (n = 9) | |
|---|---|---|---|
| Sex (% male) | 9 (39.1) | 5 (35.7) | 4 (44.4) |
| Age in months, mean (SD) | 88.5 (63) | 67.3 (52) | 122.9 (64) |
| Weight in kg, mean (SD) | 34.0 | 23.0 (14) | 54.3 (39) |
| Patient # | Trauma Center | Mechanism of Injury | Intracranial Injuries |
|---|---|---|---|
| 1 | A | fall | SAH, cerebral contusion |
| 2 | fall | SDH | |
| 3 | fall | SAH | |
| 4 | fall | EDH | |
| 5 | MVC | SDH | |
| 6 | car vs. pedestrian | none 1 | |
| 7 | B | fall | SDH |
| 8 | ATV ejection | EDH | |
| 9 | MVC | SDH | |
| 10 | fall | SDH | |
| 11 | MVC | SDH | |
| 12 | MVC | SDH, EDH | |
| 13 | C | fall off bicycle | SAH |
| 14 | [data not reported] | [data not reported] |
| Patient # | Trauma Center | Organs Injured |
|---|---|---|
| 15 | A | bone, spleen |
| 16 | bone, muscle, ligament, tendon | |
| 17 | kidney | |
| 18 | liver | |
| 19 | B | [data not reported] |
| 20 | [data not reported] | |
| 21 | C | spleen |
| 22 | bone | |
| 23 | bone |
| Pathway | p-Value | Transcripts (#) | MiRNAs (#) |
|---|---|---|---|
| ECM receptor interaction | 3.19 × 10−12 | 13 | 9 |
| Proteoglycans in cancer | 3.05 × 10−5 | 39 | 14 |
| FoxO signaling pathway | 0.00049 | 31 | 12 |
| Insulin signaling pathway | 0.0019 | 32 | 16 |
| PI3K-Akt signaling pathway | 0.0019 | 62 | 18 |
| Glioma | 0.0075 | 14 | 7 |
| MAPK signaling pathway | 0.0085 | 46 | 14 |
| ErbB signaling pathway | 0.0.011 | 19 | 10 |
| Amphetamine addiction | 0.012 | 13 | 9 |
| N-Glycan biosynthesis | 0.014 | 9 | 5 |
| mTOR signaling pathway | 0.014 | 16 | 10 |
| Protein processing in ER | 0.014 | 31 | 15 |
| Long-term depression | 0.017 | 14 | 8 |
| Cell adhesion molecules | 0.017 | 20 | 10 |
| Glutamatergic synapse | 0.017 | 19 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciancaglini, R.; Botash, A.S.; Armijo-Garcia, V.; Hymel, K.P.; Thomas, N.J.; Hicks, S.D. A Pilot Study of Saliva MicroRNA Signatures in Children with Moderate-to-Severe Traumatic Brain Injury. J. Clin. Med. 2024, 13, 5065. https://doi.org/10.3390/jcm13175065
Ciancaglini R, Botash AS, Armijo-Garcia V, Hymel KP, Thomas NJ, Hicks SD. A Pilot Study of Saliva MicroRNA Signatures in Children with Moderate-to-Severe Traumatic Brain Injury. Journal of Clinical Medicine. 2024; 13(17):5065. https://doi.org/10.3390/jcm13175065
Chicago/Turabian StyleCiancaglini, Robert, Ann S. Botash, Veronica Armijo-Garcia, Kent P. Hymel, Neal J. Thomas, and Steven D. Hicks. 2024. "A Pilot Study of Saliva MicroRNA Signatures in Children with Moderate-to-Severe Traumatic Brain Injury" Journal of Clinical Medicine 13, no. 17: 5065. https://doi.org/10.3390/jcm13175065