
Transitions and Long-Term Clinical Outcomes in Patients Admitted in Intensive Care Units Receiving Continuous Renal Replacement Therapy
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
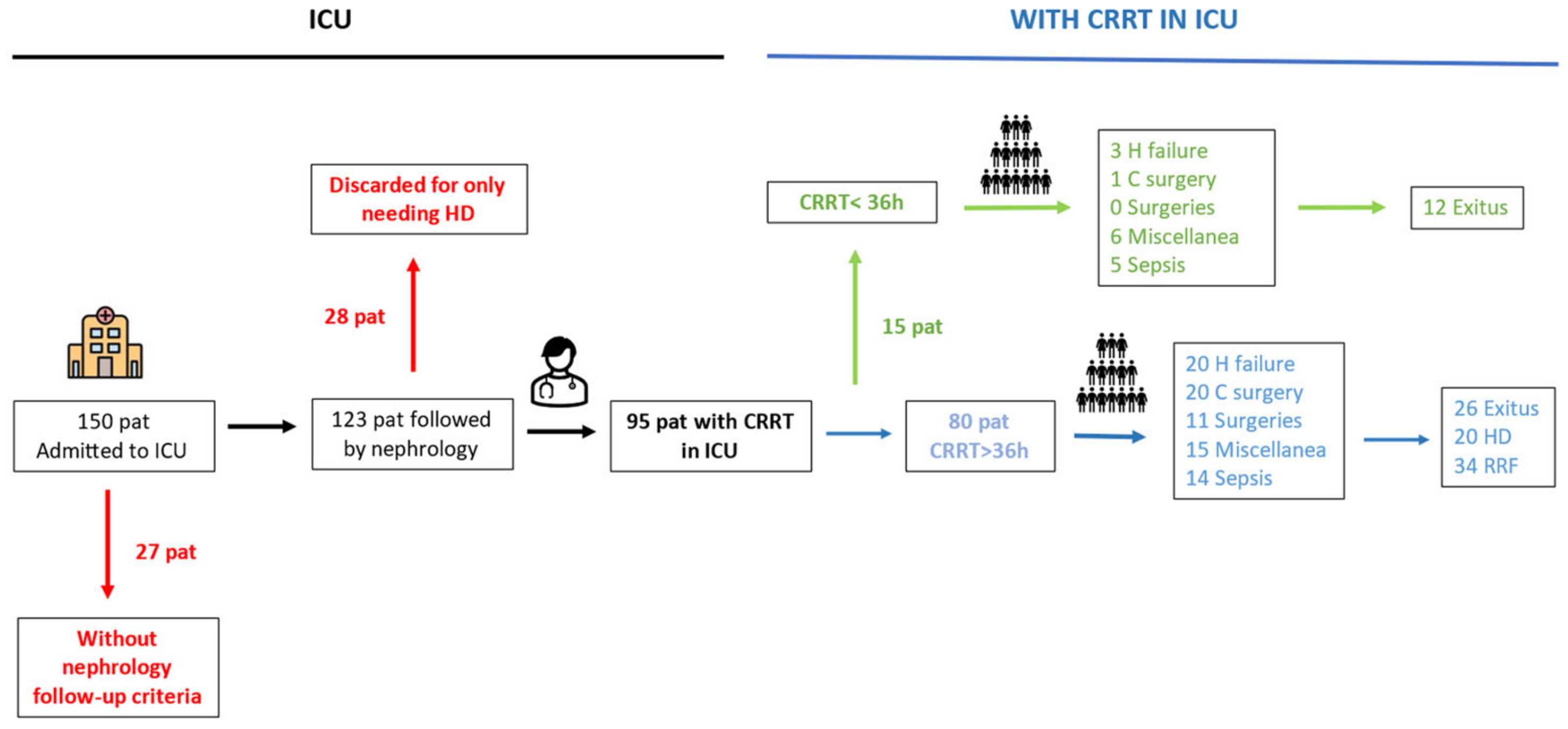
3.1. Patient Description
3.2. CRRT Transitions and Renal and Patient Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waikar, S.S.; Murray, P.T.; Singh, A.K. Core Concepts in Acute Kidney Injury; Springer: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Tenorio Cañamás, M.T.; Galeano Alvarez, C.; Rodríguez Mendiola, N.; Liaño García, F. Differential diagnosis of acute renal failure. NephroPlus 2010, 3, 1–58. [Google Scholar]
- Hoste, E.A.J.; Kellum, J.A.; Selby, N.M.; Zarbock, A.; Palevsky, P.M.; Bagshaw, S.M.; Goldstein, S.L.; Cerdá, J.; Chawla, L.S. Global epidemiology and outcomes of acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 607–625. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Romagnani, P.; Ashuntantang, G.; Ronco, C.; Zarbock, A.; Anders, H.-J. Acute kidney injury. Nat. Rev. Dis. Primer 2021, 7, 52. [Google Scholar] [CrossRef]
- Negi, S.; Koreeda, D.; Kobayashi, S.; Yano, T.; Tatsuta, K.; Mima, T.; Shigematsu, T.; Ohya, M. Acute kidney injury: Epidemiology, outcomes, complications, and therapeutic strategies. Semin. Dial. 2018, 31, 519–527. [Google Scholar] [CrossRef]
- Susantitaphong, P.; Cruz, D.N.; Cerda, J.; Abulfaraj, M.; Alqahtani, F.; Koulouridis, I.; Jaber, B.L. World incidence of AKI: A meta-analysis. Clin. J. Am. Soc. Nephrol. 2013, 8, 1482–1493, Erratum in: Clin. J. Am. Soc. Nephrol. 2014, 9, 1148. [Google Scholar] [CrossRef]
- Herrera-Gutierrez, M.E.; Seller-Perez, G.; Maynar-Moliner, J.; Sanchez-Izquierdo-Riera, J.A. FRAMI Study Research Group. Epidemiology of acute renal failure in Spanish ICUs. FRAMI Prospect Multicent Study. Intensive Med. 2006, 30, 260–267. [Google Scholar]
- Tomasa, T.M.; Sabater, J.; Poch, E.; Fort Ros, J.; Lloret Cora, M.J.; Roca Antònio, J.; Navas Pérez, A.; Ortiz Ballujera, P.; Serviá Goxiar, L.; González de Molina Ortiz, F.J.; et al. Current management of continuous renal replacement therapies: Multicenter epidemiological study. Intensive Med. 2017, 41, 216–226. [Google Scholar]
- Tolwani, A. Continuous renal-replacement therapy for acute kidney injury. N. Engl. J. Med. 2012, 367, 2505–2514. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Gutierrez, M.E.; Seller-Perez, G.; Sanchez-Izquierdo-Riera, J.A.; Maynar-Molinr, J.; COFRADE Investigators Group. Prevalence of acute kidney injury in intensive care units: The “Cut-off of prevalence of renal dysfunction and clearance in critically ill patients” point-prevalence multicenter study. J. Crit. Care 2013, 28, 687–694. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siev, E.D.; Baghaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Filtzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef]
- Kidney Disease Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl 2012, 2, 1–138. [Google Scholar]
- Valdenebro, M.; Martín-Rodríguez, L.; Tarragón, B.; Sánchez-Briales, P.; Portolés, J. Renal replacement therapy in critically ill patients with acute kidney injury: 2020 nephrologist’s perspective. Nefrologia 2021, 41, 102–114. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Report of the Madrid Registree of Renal Patients. Available online: https://www.comunidad.madrid/sites/default/files/doc/sanidad/asis/informe_remer_2021.pdf (accessed on 20 May 2024).
- Srijan Tandukar, M.D.; Paul, M.; Palevsky, M.D. Continuous Renal Replacement Therapy Who, When, Why, and How. CHEST 2019, 155, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Morgera, S.; Schneider, M.; Neumayer, H. Long-term outcomes after acute kidney injury. Crit. Care Med. 2008, 36 (Suppl. S4), S193–S197. [Google Scholar] [CrossRef]
- Allegretti, A.S.; Steele, D.J.; David-Kasdan, J.; Bajwa, E.; Niles, J.L.; Bhan, I. Continuous renal replacement therapy outcomes in acute kidney injury and end-stage renal disease: A cohort study. Critical Care 2013, 17, R109. [Google Scholar] [CrossRef]
- Barbar, S.D.; Clere-Jehl, R.; Bourredjem, A.; Hernu, R.; Montini, F.; Bruyère, R.; Lebert, C.; Bohé, J.; Badie, J.; Eraldi, J.-P.; et al. IDEAL-ICU Trial Investigators and the CRICS TRIGGERSEP Network. Timing of Renal-Replacement Therapy in Patients with Acute Kidney Injury and Sepsis. N. Engl. J. Med. 2018, 379, 1431–1442. [Google Scholar] [CrossRef] [PubMed]
- Gaudry, S.; Hajage, D.; Schortgen, F.; Martin-Lefevre, L.; Pons, B.; Boulet, E.; Boyer, A.; Chevrel, G.; Lerolle, N.; Carpentier, D.; et al. AKIKI Study Group. Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit. N. Engl. J. Med. 2016, 375, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, J.; Soroko, S.B.; Cherlow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Metha, R.L. Fluid accumulation, survival and recovery of renal function and critically ill patients with acute renal injury. Kidney Int. 2009, 76, 422–427. [Google Scholar] [CrossRef]
- Fayad, A.I.; Buamscha, D.G.; Ciapponi, A. Timing of renal replacement therapy initiation for acute kidney injury. Cochrane Database Syst. Rev. 2018, 12, CD010612. [Google Scholar] [CrossRef]
- Jia, Y.; Jiang, L.; Wen, Y.; Wang, M.; Xi, X.; Du, B. Effect of renal replacement therapy on outcomes of critically ill patients in the intensive care unit. Nephrology 2018, 23, 405–410. [Google Scholar] [CrossRef]
- Tumlin, J.A.; Murugan, R.; Deane, A.M.; Ostermann, M.; Busse, L.W.; Ham, K.R.; Kashani, K.; Szerlip, H.M.; Prowle, J.R.; Bihora, A.; et al. Outcomes in patients with vasodilatory shock and renal replacement therapy treated with intravenous Angiotensin II. Crit. Care Med. 2018, 46, 949–957. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Santamaría, R.; Gorostidi, M.; Nefrologia al día. Síndrome Cardiorenal. Available online: https://www.nefrologiaaldia.org/es-articulo-sindrome-cardiorenal-555 (accessed on 20 May 2024).
- Kashani, K.; Rosner, M.H.; Haase, M.; Lewington, A.J.; O’Donoghue, D.J.; Wilson, F.P.; Nadim, M.K.; Silver, S.A.; Zarbock, A.; Ostermann, M.; et al. Quality improvement goals for acute kidney injury. Clin. J. Am. Soc. Nephrol. 2019, 14, 941–953. [Google Scholar] [CrossRef]
- Wang, X.-T.; Wang, C.; Zhang, H.-M.; Liu, D.-W. Clarifications on Continuous Renal Replacement Therapy and Hemodynamics. Chin. Med. J. 2017, 130, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Joannes-Boyau, O.; Honore, P.M.; Perez, P.; Bagshaw, S.M.; Grand, H.; Canivet, J.-L.; Dewitte, A.; Flamens, C.; Pujo, W.; Grandoulier, A.-S.; et al. High-volume versus standard-volume haemofiltration for septic shock patients with acute kidney injury (IVOIRE study): A multicenter randomized controlled trial. Intensive Care Med. 2013, 39, 1535–1546. [Google Scholar] [CrossRef]
- Mas-Font, S.; Ros-Martinez, J.; Pérez-Calvo, C.; Villa-Díaz, P.; Aldunate-Calvo, S.; Moreno-Clari, E. Prevention of acute kidney injury in Intensive Care Units. Intensive Med. 2017, 41, 116–126. [Google Scholar] [CrossRef]
- Chou, Y.-H.; Huang, T.-M.; Wu, V.-C.; Wang, C.-Y.; Shiao, C.-C.; Lai, C.-F.; Tsai, H.-B.; Chao, C.-T.; Young, G.-H.; Wang, W.-J.; et al. Impact of timing of renal replacement therapy initiation on outcome of septic acute kidney injury. Crit. Care 2011, 15, R134. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Cruz, D.N.; Gibney, R.N.; Ronco, C. A proposed algorithm for initiation of renal replacement therapy in adult critically ill patients. Crit. Care 2009, 13, 317. [Google Scholar] [CrossRef] [PubMed]
- Maynar-Moliner, J.; Sanchez-Izquierdo-Riera, J.A.; Herrera-Gutierrez, M. Renal support in critically ill patients with acute kidney injury. N. Engl. J. Med. 2008, 359, 1960, author reply 1961-2. [Google Scholar] [PubMed]
- Karsanji, D.J.; Pannu, N.; Manns, B.J.; Hemmelgarn, B.R.; Tan, Z.; Jindal, K.; Scott-Douglas, N.; James, M.T. Disparity between nephrologists’ opinions and contemporary practices for community follow-up after AKI hospitalization. Clin. J. Am. Soc. Nephrol. 2017, 12, 1753–1761. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Heart Failure | Cardiac Surgery | Other Surgeries | Sepsis | Miscellanea | Total | p Value | |
|---|---|---|---|---|---|---|---|
| N | 20 | 20 | 11 | 14 | 15 | 80 | |
| Men (%) | 95.0 | 55.0 | 63.3 | 64.3 | 80.0 | 72.5 | 0.05 |
| Age (year) | 62.7(15.5) | 69.1 (9.8) | 65.3 (12.1) | 66.0 (13.7) | 62.9 (16.7) | 65.3 (13.6) | 0.6 |
| Charlson index | 7 (3.4) | 5.5 (1.9) | 8.2 (4.0) | 5.4 (2.5) | 6.7 (3.4) | 6.4 (3.1) | 0.09 |
| Previous CKD (%) | 40.0 | 20.0 | 27.3 | 23.1 | 26.7 | 27.8 | 0.7 |
| DM (%) | 55.6 | 11.1 | 36.4 | 28.6 | 28.6 | 32.0 | 0.08 |
| Ischemic heart disease (%) | 40.0 | 31.6 | 27.3 | 14.4 | 13.3 | 26.6 | 0.3 |
| Reduced LVEF (<50%) (%) | 42.1 | 17.6 | 30.0 | 12.5 | 16.7 | 25.8 | 0.4 |
| Diastolic dysfunction (%) | 16.7 | 11.8 | 0.0 | 0.0 | 8.3 | 9.5 | 0.8 |
| Previous H failure (%) | 65.0 | 85.0 | 45.5 | 78.6 | 53.3 | 67.5 | 0.1 |
| Stroke or TIA (%) | 10.0 | 20.0 | 18.2 | 0.0 | 13.3 | 12.5 | 0.5 |
| Liver disease (%) | 15.0 | 10.0 | 54.5 | 28.6 | 40.0 | 26.2 | 0.04 |
| Previous neoplasia (%) | 25.0 | 15.0 | 45.5 | 28.6 | 33.3 | 27.5 | 0.5 |
| COPD (%) | 40.0 | 20.0 | 36.4 | 14.3 | 26.7 | 27.5 | 0.4 |
| Exitus/CRRT output (%) | 40.0 | 15.0 | 54.2 | 21.4 | 40.0 | 32.5 | 0.4 |
| Exitus by 1 year (%) | 85.0 | 45.0 | 81.8 | 42.9 | 53.3 | 61.3 | 0.4 |
| Heart Failure | Cardiac Surgery | Other Surgeries | Sepsis | Miscellanea | Total | p Value | |
|---|---|---|---|---|---|---|---|
| Etiology | 0.06 | ||||||
| Prerenal AKI (%) | 60.0 | 35.0 | 27.3 | 35.7 | 73.3 | 47.5 | |
| ATN (%) | 40.0 | 65.0 | 72.7 | 64.3 | 26.7 | 52.5 | |
| Laboratory data | |||||||
| sCr (mg/dL) | 2.5 (1.6) | 2.0 (1.1) | 2.1 (0.9) | 2.1 (1.4) | 3.1 (1.4) | 2.3 (1.3) | 0.1 |
| sUr (mg/dL) | 137.3 (66.8) | 113.2 (67.3) | 104.8 (60.7) | 115.5 (46.3) | 143.2 (77.4) | 123.8 (65.6) | 0.45 |
| Bicarbonate (mmol/L) | 21.6 (4.3) | 25.7 (4.2) | 22.5 (2.6) | 24.3 (5.8) | 19.7 (6.5) | 22.9 (5.2) | 0.006 |
| Lactate (mmol/L) | 1.4 [1–4] | 1.1 [0.8–1.6] | 1.6 [1.3–1.9] | 1.4 [1.1–2.4] | 2.2 [1.3–6.8] | 1.4 [1–3] | 0.8 |
| Diuresis (ml/h) | 4.6 (10.0) | 7.2 (17.1) | 13.8 (34.1) | 38.8 (73.4) | 0.9 (2.6) | 11.8 (36.0) | 0.002 |
| ECMO (%) | 20.0 | 15.6 | 18.1 | 0.0 | 1.0 | 12.7 | 0.4 |
| VAS (%) | 85.0 | 90.0 | 81.8 | 78.6 | 73.3 | 82.5 | 0.8 |
| CRRT modality | 0.3 | ||||||
| CVVHDF (%) | 85.0 | 75.0 | 81.4 | 85.7 | 100.0 | 85.0 | |
| CVVHF (%) | 0.0 | 10.0 | 0.0 | 14.3 | 0.0 | 5.1 | |
| SCUF (%) | 15.0 | 15.0 | 18.2 | 0.0 | 0.0 | 10.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdenebro, M.; Portoles, J.; Serrano Salazar, M.L.; Muñoz Sánchez, A.; Alameda-Aguado, I.; Martín Rodriguez, L.; Zalamea-Jarrin, F.; López-Sánchez, P. Transitions and Long-Term Clinical Outcomes in Patients Admitted in Intensive Care Units Receiving Continuous Renal Replacement Therapy. J. Clin. Med. 2024, 13, 5085. https://doi.org/10.3390/jcm13175085
Valdenebro M, Portoles J, Serrano Salazar ML, Muñoz Sánchez A, Alameda-Aguado I, Martín Rodriguez L, Zalamea-Jarrin F, López-Sánchez P. Transitions and Long-Term Clinical Outcomes in Patients Admitted in Intensive Care Units Receiving Continuous Renal Replacement Therapy. Journal of Clinical Medicine. 2024; 13(17):5085. https://doi.org/10.3390/jcm13175085
Chicago/Turabian StyleValdenebro, María, Jose Portoles, María Luisa Serrano Salazar, Ana Muñoz Sánchez, Ines Alameda-Aguado, Leyre Martín Rodriguez, Felipe Zalamea-Jarrin, and Paula López-Sánchez. 2024. "Transitions and Long-Term Clinical Outcomes in Patients Admitted in Intensive Care Units Receiving Continuous Renal Replacement Therapy" Journal of Clinical Medicine 13, no. 17: 5085. https://doi.org/10.3390/jcm13175085
APA StyleValdenebro, M., Portoles, J., Serrano Salazar, M. L., Muñoz Sánchez, A., Alameda-Aguado, I., Martín Rodriguez, L., Zalamea-Jarrin, F., & López-Sánchez, P. (2024). Transitions and Long-Term Clinical Outcomes in Patients Admitted in Intensive Care Units Receiving Continuous Renal Replacement Therapy. Journal of Clinical Medicine, 13(17), 5085. https://doi.org/10.3390/jcm13175085