
Effects of Melatonin on Exercise-Induced Oxidative Stress in Adults with Obesity Undergoing a Multidisciplinary Body Weight Reduction Program

 , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Subjects and Protocol
2.3. Body Weight Reduction Program (BWRP)
2.4. Resting Energy Expenditure
2.5. Anthropometric Measurements
2.6. Biological Sample Collection
2.7. Metabolic, Biochemical and Hormonal Evaluation
2.8. Measurement of Blood Pressure
2.9. Analytical Methods for d-ROMs and BAP
2.10. Measurement of HbSSG by MALDI
2.11. Statistical Analysis
3. Results
4. Discussion
- (1)
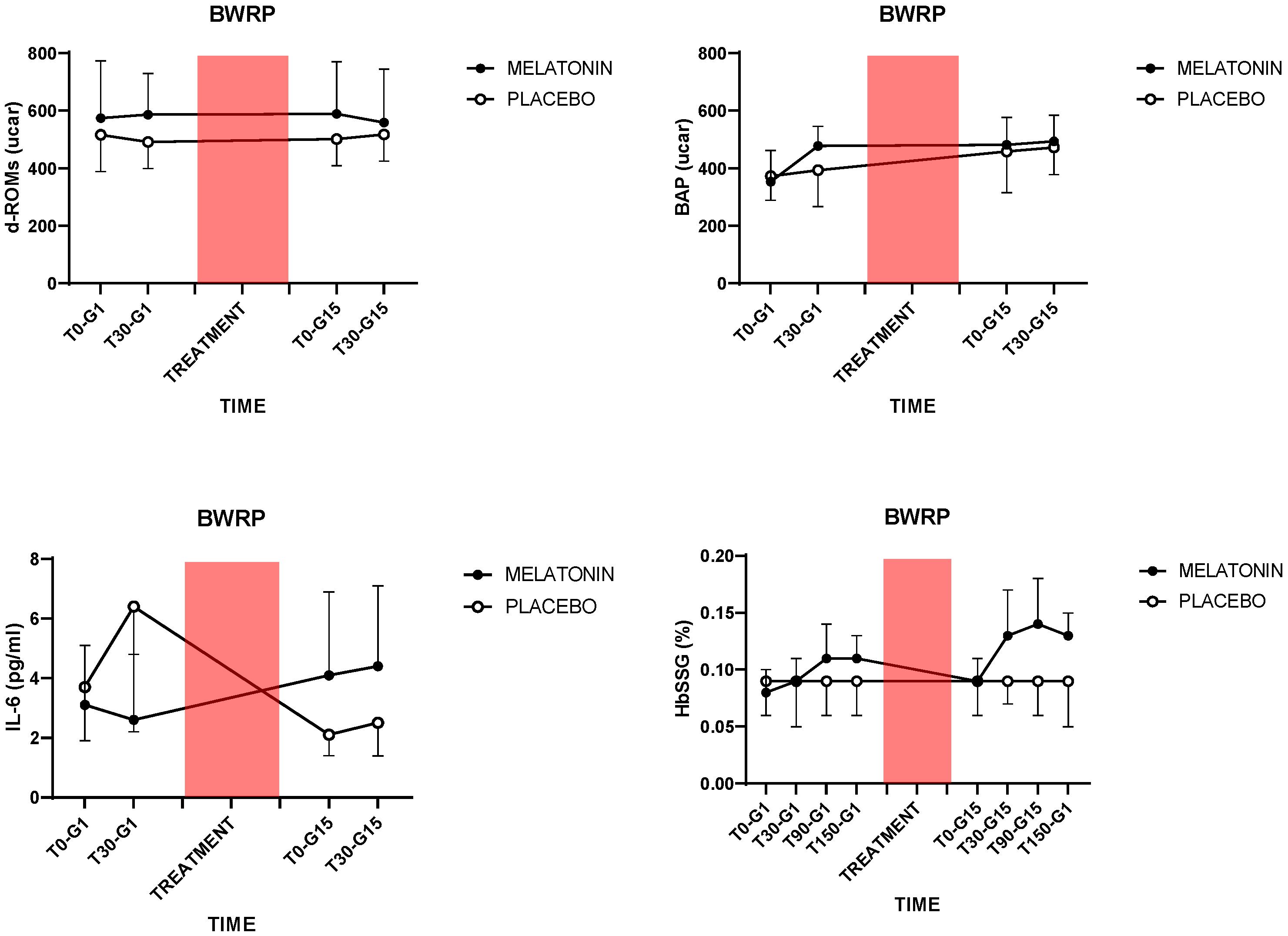
- Two weeks of BWRP, combined with a placebo (i.e., without any “active” treatment with melatonin), exerted anti-inflammatory effects, as demonstrated by the decreases in plasma IL-6 and blood NLR; the former a pro-inflammatory cytokine [40] and the latter a peripheral biomarker that conjugates two components of the immune system, i.e., the innate immune response, mainly due to neutrophils, and adaptive immunity, supported by lymphocytes [41]. Parallelly, when measuring a surrogate of antioxidant capabilities in the organism [42], a BWRP-induced increase in plasma BAP occurred, an effect that was independent of the treatment with melatonin. Melatonin, independently from BWRP, increased plasma d-ROMs and erythrocytic HbSSG, two peripheral markers of oxidative stress [43], which were generated in each exercise test (at G1 and G15 for T90 and T150);
- (2)
- Melatonin, when acutely administered (i.e., the single dose at G0), reduced plasma levels of IL-6 at G1 (T0), implying a different anti-inflammatory vs. pro-inflammatory effect for single or continuous administration;
- (3)
- Apart from decreases in BMI and WC that were found in both groups, BWRP exerted additional metabolic benefits only in the placebo group (e.g., decreases in plasma glucose and blood HbA1c).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Keaney, J.F.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.F.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and Systemic Oxidative Stress. Clinical Correlates of Oxidative Stress in the Framingham Study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Olusi, S. Obesity Is an Independent Risk Factor for Plasma Lipid Peroxidation and Depletion of Erythrocyte Cytoprotectic Enzymes in Humans. Int. J. Obes. 2002, 26, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Montezano, A.C.; Touyz, R.M. Reactive Oxygen Species and Endothelial Function–role of Nitric Oxide Synthase Uncoupling and Nox Family Nicotinamide Adenine Dinucleotide Phosphate Oxidases. Basic Clin. Pharmacol. Toxicol. 2012, 110, 87–94. [Google Scholar] [CrossRef]
- Kunwar, A.; Priyadarsini, K.I. Free Radicals, Oxidative Stress and Importance of Antioxidants in Human Health. J. Med. Allied Sci. 2011, 1, 53–60. [Google Scholar]
- Vider, J.; Laaksonen, D.E.; Kilk, A.; Atalay, M.; Lehtmaa, J.; Zilmer, M.; Sen, C.K. Physical Exercise Induces Activation of Nf-kappab in Human Peripheral Blood Lymphocytes. Antioxid. Redox Signal. 2001, 3, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Korda, M.; Kubant, R.; Patton, S.; Malinski, T. Leptin-induced Endothelial Dysfunction in Obesity. Am. J. Physiol. Heart Circ. Physiol. 2008, 295, H1514–H1521. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Tchernova, J.; Whincup, P.H.; Lowe, G.D.O.; Kelly, A.; Rumley, A.; Wallace, A.M.; Sattar, N. Plasma Leptin: Associations with Metabolic, Inflammatory and Haemostatic Risk Factors for Cardiovascular Disease. Atherosclerosis 2007, 191, 418–426. [Google Scholar] [CrossRef]
- Bloomer, R.J.; Kabir, M.M.; Marshall, K.E.; Canale, R.E.; Farney, T.M. Postprandial Oxidative Stress in Response to Dextrose and Lipid Meals of Differing Size. Lipids Health Dis. 2010, 9, 79. [Google Scholar] [CrossRef]
- Miyazaki, H.; Oh-ishi, S.; Ookawara, T.; Kizaki, T.; Toshinai, K.; Ha, S.; Haga, S.; Ji, L.L.; Ohno, H. Strenuous Endurance Training in Humans Reduces Oxidative Stress Following Exhausting Exercise. Eur. J. Appl. Physiol. 2001, 84, 1–6. [Google Scholar] [CrossRef]
- Yavari, A.; Javadi, M.; Mirmiran, P.; Bahadoran, Z. Exercise-induced Oxidative Stress and Dietary Antioxidants. Asian J. Sports Med. 2015, 6, e24898. [Google Scholar] [CrossRef]
- Vincent, H.K.; Morgan, J.W.; Vincent, K.R. Obesity Exacerbates Oxidative Stress Levels After Acute Exercise. Med. Sci. Sports Exerc. 2004, 36, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Vincent, H.K.; Vincent, K.R.; Bourguignon, C.; Braith, R.W. Obesity and Postexercise Oxidative Stress in Older Women. Med. Sci. Sports Exerc. 2005, 37, 213–219. [Google Scholar] [CrossRef]
- Brinkmann, C.; Chung, N.; Schmidt, U.; Kreutz, T.; Lenzen, E.; Schiffer, T.; Geisler, S.; Graf, C.; Montiel-Garcia, G.; Renner, R. Training Alters the Skeletal Muscle Antioxidative Capacity in Non-insulin-dependent Type 2 Diabetic Men. Scand. J. Med. Sci. Sports 2012, 22, 213–219. [Google Scholar] [CrossRef]
- Huang, C.-J.; McAllister, M.J.; Slusher, A.L.; Slusher, A.L.; Webb, H.E.; Mock, J.T.; Acevedo, E.O. Obesity-related Oxidative Stress: The Impact of Physical Activity and Diet Manipulation. Sports Med. Open 2015, 1, 32. [Google Scholar] [CrossRef]
- Reiter, R.J.; Tan, D.X.; Sainz, R.M.; Mayo, J.C.; Lopez-Burillo, S. Melatonin: Reducing the Toxicity and Increasing the Efficacy of Drugs. J. Pharm. Pharmacol. 2010, 54, 1299–1321. [Google Scholar] [CrossRef] [PubMed]
- Stehle, J.H.; Reuss, S.; Riemann, R.; Seidel, A.; Vollrath, L. The Role of Arginine-vasopressin for Pineal Melatonin Synthesis in the Rat: Involvement of Vasopressinergic Receptors. Neurosci. Lett. 1991, 123, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.; Mayo, J.C.; Sainz, R.M.; Antolín, I.; Herrera, F.; Martín, V.; Reiter, R.J. Regulation of Antioxidant Enzymes: A Significant Role for Melatonin. J. Pineal Res. 2004, 36, 1–9. [Google Scholar] [CrossRef]
- Cagnacci, A.; Cannoletta, M.; Renzi, A.; Baldassari, F.; Arangino, S.; Volpe, A. Prolonged Melatonin Administration Decreases Nocturnal Blood Pressure in Women. Am. J. Hypertens. 2005, 18, 1614–1618. [Google Scholar] [CrossRef]
- Maarman, G.J.; Reiter, R.J. Melatonin Therapy for Blunt Trauma and Strenuous Exercise: A Mechanism Involving Cytokines, Nfκb, Akt, MAFBX and MURF-1. J. Sports Sci. 2018, 36, 1897–1901. [Google Scholar] [CrossRef]
- Reiter, R.J.; Mayo, J.C.; Tan, D.X.; Sainz, R.M.; Alatorre-Jiménez, M.A.; Qin, L. Melatonin as an Antioxidant: Under Promises but over Delivers. J. Pineal Res. 2016, 61, 253–278. [Google Scholar] [CrossRef]
- Tan, D. Melatonin: A Potent, Endogenous Hydroxyl Radical Scavenger. J. Pineal Res. 1993, 1, 57–60. [Google Scholar]
- Gedikli, S.; Gelen, V.; Şengül, E.; Ozkanlar, S.; Gur, C.; Agirbas, O.; Çakmak, F.; Kara, A. Therapeutic Effects of Melatonin on Liver and Kidney Damages in Intensive Exercise Model of Rats. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 308–314. [Google Scholar] [CrossRef]
- Leonardo-Mendonça, R.C.; Ocaña-Wilhelmi, J.; de Haro, T.; de Teresa-Galván, C.; Guerra-Hernández, E.; Rusanova, I.; Fernández-Ortiz, M.; Sayed, R.K.A.; Sayed, R.K.A.; Escames, G. The Benefit of a Supplement with the Antioxidant Melatonin on Redox Status and Muscle Damage in Resistance-trained Athletes. Appl. Physiol. Nutr. Metab. 2017, 42, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Ochoa, J.J.; Díaz-Castro, J.; Kajarabille, N.; García, C.; Guisado, I.M.; De Teresa, C.; Guisado, R. Melatonin Supplementation Ameliorates Oxidative Stress and Inflammatory Signaling Induced by Strenuous Exercise in Adult Human Males. J. Pineal Res. 2011, 51, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.L. Antioxidants and oxidative stress in exercise. Proc. Soc. Exp. Biol. Med. 1999, 222, 283–292. [Google Scholar] [CrossRef]
- Maldonado, M.D.; Manfredi, M.; Ribas-Serna, J.; Garcia-Moreno, H.; Calvo, J.R. Melatonin Administrated Immediately Before an Intense Exercise Reverses Oxidative Stress, Improves Immunological Defenses and Lipid Metabolism in Football Players. Physiol. Behav. 2012, 105, 1099–1103. [Google Scholar] [CrossRef]
- Reiter, R.J.; Tan, D.X.; Mayo, J.C.; Sainz, R.M.; León, J.; Czarnocki, Z. Melatonin as an Antioxidant: Biochemical Mechanisms and Pathophysiological Implications in Humans. Acta Biochim. Pol. 2003, 50, 1129–1146. [Google Scholar] [CrossRef]
- Borges, L.; Dermargos, A.; da Silva Junior, E.P.; Weimann, E.; Lambertucci, R.H.; Hatanaka, E. Melatonin Decreases Muscular Oxidative Stress and Inflammation Induced by Strenuous Exercise and Stimulates Growth Factor Synthesis. J. Pineal Res. 2015, 58, 166–172. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Akerstrom, T.; Nielsen, A.R.; Fischer, C.P. Role of Myokines in Exercise and Metabolism. J. Appl. Physiol. 2007, 103, 1093–1098. [Google Scholar] [CrossRef]
- Plomgaard, P.; Penkowa, M.; Pedersen, B.K. Fiber Type Specific Expression of Tnf-alpha, IL-6 and IL-18 in Human Skeletal Muscles. Exerc. Immunol. Rev. 2005, 11, 53. [Google Scholar]
- Mason, S.A.; Trewin, A.J.; Parker, L.; Wadley, G.D. Antioxidant Supplements and Endurance Exercise: Current Evidence and Mechanistic Insights. Redox Biol. 2020, 35, 101471. [Google Scholar] [CrossRef]
- Czuczejko, J.; Sielski, Ł.; Woźniak, B.; Woźniak, A.; Szewczyk-Golec, K. Melatonin Supplementation Improves Oxidative and Inflammatory State in the Blood of Professional Athletes During the Preparatory Period for Competitions. Free Radic. Res. 2019, 53, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Almendros-Ruiz, A.; Lopez-Moro, A.; Conde-Pipò, J.; Santalla, A.; Requena, B.; Mariscal-Arcas, M. The Effects of Melatonin Supplementation on Professional Football Player Performance: A Systematic Review. Nutrients 2023, 15, 4467. [Google Scholar] [CrossRef]
- Borg, G. Perceived Exertion: A Note on ‘history’ and Methods. Med. Sci. Sports 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Masini, S.; Carpeggiani, C.; L’Abbate, A.; Boni, C.; Zucchelli, G.C. In Vivo Total Antioxidant Capacity: Comparison of Two Different Analytical Methods. Clin. Chem. Lab. Med. 2004, 42, 84–89. [Google Scholar] [CrossRef]
- Bamonti, F.; Novembrino, C.; Ippolito, S.; Soresi, E.; Ciani, A.; Lonati, S.; Scurati-Manzoni, E.; Cighetti, G. Increased Free Malondialdehyde Concentrations in Smokers Normalise with a Mixed Fruit and Vegetable Juice Concentrate: A Pilot Study. Clin. Chem. Lab. Med. 2006, 44, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Campise, M.; Bamonti, F.; Novembrino, C.; Ippolito, S.; Tarantino, A.; Cornelli, U.; Lonati, S.; Cesana, B.M.; Ponticelli, C. Oxidative stress in kidney transplant patients. Transplantation 2003, 76, 1474–1478. [Google Scholar] [CrossRef]
- Rubino, F.M.; Ottolenghi, S.; Brizzolari, A.; Maioli, C.; Samaja, M.; Paroni, R. Enhanced-precision Measurement of Glutathionyl Hemoglobin by Maldi-tof MS. Molecules 2023, 28, 497. [Google Scholar] [CrossRef]
- Éder, K.; Baffy, N.; Falus, A.; Falus, A.; Fülöp, A. The Major Inflammatory Mediator Interleukin-6 and Obesity. Inflamm. Res. 2009, 58, 727–736. [Google Scholar] [CrossRef]
- Marra, A.; Bondesan, A.; Caroli, D.; Grugni, G.; Sartorio, A. The Neutrophil to Lymphocyte Ratio (NLR) Positively Correlates with the Presence and Severity of Metabolic Syndrome in Obese Adults, but Not in Obese Children/adolescents. BMC Endocr. Disord. 2023, 23, 121. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Baik, H.W.; Yoon, Y.S.; Joung, H.; Park, J.S.; Park, S.J.; Jang, E.J.; Park, S.W.; Kim, S.J.; Kim, M.J. Measurement of Antioxidant Capacity Using the Biological Antioxidant Potential Test and Its Role as a Predictive Marker of Metabolic Syndrome. Korean J. Intern. Med. 2014, 29, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Ottolenghi, S.; Rubino, F.M.; Sabbatini, G.; Coppola, S.; Veronese, A.; Chiumello, D.; Paroni, R. Oxidative Stress Markers to Investigate the Effects of Hyperoxia in Anesthesia. Int. J. Mol. Sci. 2019, 20, 5492. [Google Scholar] [CrossRef] [PubMed]
- Manna, P.; Jain, S.K. Obesity, Oxidative Stress, Adipose Tissue Dysfunction, and the Associated Health Risks: Causes and Therapeutic Strategies. Metab. Syndr. Relat. Disord. 2015, 13, 423–444. [Google Scholar] [CrossRef]
- Pingitore, A.; Lima, G.P.; Mastorci, F.; Quinones, A.; Iervasi, G.; Vassalle, C. Exercise and oxidative stress: Potential effects of antioxidant dietary strategies in sports. Nutrition 2015, 31, 916–922. [Google Scholar] [CrossRef]
- Guan, Q.; Wang, Z.; Cao, J.; Dong, Y.; Chen, Y. Mechanisms of melatonin in obesity: A review. Int. J. Mol. Sci. 2021, 23, 218. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.M.; Zhang, Y. Melatonin: A Well-documented Antioxidant with Conditional Pro-oxidant Actions. J. Pineal Res. 2014, 57, 131–146. [Google Scholar] [CrossRef]
- Semak, I.; Naumova, M.; Korik, E.; Terekhovich, V.; Wortsman, J.; Slominski, A. A Novel Metabolic Pathway of Melatonin: Oxidation by Cytochrome C. Biochemistry 2005, 44, 9300–9307. [Google Scholar] [CrossRef]
- Thakor, A.S.; Thakor, A.S.; Allison, B.J.; Niu, Y.; Botting, K.J.; Serón-Ferré, M.; Herrera, E.A.; Giussani, D.A. Melatonin Modulates the Fetal Cardiovascular Defense Response to Acute Hypoxia. J. Pineal Res. 2015, 59, 80–90. [Google Scholar] [CrossRef]
- Fischer, T.W.; Scholz, G.; Knöll, B.; Hipler, U.-C.; Elsner, P. Melatonin Reduces Uv-induced Reactive Oxygen Species in a Dose-dependent Manner in Il-3-stimulated Leukocytes. J. Pineal Res. 2001, 31, 39–45. [Google Scholar] [CrossRef]
- Agathokleous, E.; Kitao, M.; Calabrese, E.J. New Insights into the Role of Melatonin in Plants and Animals. Chem. Biol. Interact. 2019, 299, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, S.; Rizvi, S.I. Circadian Modulation of Human Erythrocyte Plasma Membrane Redox System by Melatonin. Neurosci. Lett. 2012, 518, 32–35. [Google Scholar] [CrossRef]
- Tesoriere, L.; D’Arpa, D.; Conti, S.; Giaccone, V.; Pintaudi, A.M.; Livrea, M.A. Melatonin Protects Human Red Blood Cells from Oxidative Hemolysis: New Insights into the Radical-scavenging Activity. J. Pineal Res. 1999, 27, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Çiftçi, M.; Bilici, D.; Küfrevioğlu, O.I. Effects of Melatonin on Enzyme Activities of Glucose-6-phosphate Dehydrogenase from Human Erythrocytes in Vitro and from Rat Erythrocytes in Vivo. J. Pineal Res. 2001, 44, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Colombo, G.; Dalle-Donne, I.; Giustarini, D.; Gagliano, N.; Portinaro, N.; Colombo, R.; Rossi, R.; Milzani, A. Cellular Redox Potential and Hemoglobin S-glutathionylation in Human and Rat Erythrocytes: A Comparative Study. Blood Cells Mol. Dis. 2010, 44, 133–139. [Google Scholar] [CrossRef]
- Wang, M.D.; Liu, J.; Zhang, Z.; Zhang, H.; Wang, N.; Chen, X.; Han, X.; Lu, Q.; Chi, S. Effects of Dietary Intervention on Inflammatory Markers in Metabolic Syndrome: A Systematic Review and Meta-analysis. Front. Nutr. 2022, 9, 846591. [Google Scholar] [CrossRef]
- Soomro, S. Oxidative Stress and Inflammation. Open J. Immunol. 2019, 9, 1–20. [Google Scholar] [CrossRef]
- Pérez-Torres, I.; Guarner-Lans, V.; Rubio-Ruiz, M.E. Reductive Stress in Inflammation-associated Diseases and the Pro-oxidant Effect of Antioxidant Agents. Int. J. Mol. Sci. 2017, 18, 2098. [Google Scholar] [CrossRef]
- Lubos, E.; Loscalzo, J.; Handy, D.E. Glutathione Peroxidase-1 in Health and Disease: From Molecular Mechanisms to Therapeutic Opportunities. Antioxid. Redox Signal. 2011, 15, 1957–1997. [Google Scholar] [CrossRef]
- Brewer, A.C.; Murray, T.V.A.; Arno, M.; Zhang, M.; Anilkumar, N.; Mann, G.E.; Shah, A.M. Nox4 Regulates Nrf2 and Glutathione Redox in Cardiomyocytes in Vivo. Free Radic. Biol. Med. 2011, 51, 205–215. [Google Scholar] [CrossRef]
- Korge, P.; Calmettes, G.; Weiss, J.N. Increased Reactive Oxygen Species Production During Reductive Stress: The Roles of Mitochondrial Glutathione and Thioredoxin Reductases. Biochim. Biophys. Acta. 2015, 1847, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.P. How Mitochondria Produce Reactive Oxygen Species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef]
- Almoraie, M.M.; Shatwan, I.M. The Potential Effects of Dietary Antioxidants in Obesity: A Comprehensive Review of the Literature. Healthcare 2024, 12, 416. [Google Scholar] [CrossRef]

{kind=link}
| Parameter | Melatonin | Placebo | ||
|---|---|---|---|---|
| G1 | G15 | G1 | G15 | |
| N. | 9 | 9 | 9 | 9 |
| Sex (F/M) | 7/2 | 7/2 | 6/3 | 6/3 |
| Age (years) | 27.8 ± 5.6 | 27.8 ± 5.6 | 28.8 ± 5.0 | 28.9 ± 5.0 |
| BMI (kg/m2) | 43.0 ± 4.9 | 41.6 ± 4.4 a | 42.8 ± 4.0 | 40.7 ± 4.0 b |
| WC (cm) | 110.2 ± 10.0 | 104.6 ± 9.5 a | 119.1 ± 12.1 | 111.3 ± 11.5 b |
| SBP (mmHg) | 131.1 ± 7.8 | 122.2 ± 8.3 | 122.9 ± 14.0 | 123.9 ± 10.5 |
| DBP (mmHg) | 81.1 ± 6.0 | 77.2 ± 4.4 | 79.4 ± 8.8 | 75.6 ± 7.7 |
| HR (bpm) | 92.1 ± 13.3 | 81.3 ± 7.2 a | 83.7 ± 12.6 | 80.3 ± 14.5 |
| FFM (kg) | 55.1 ± 7.2 | 54.1 ± 6.7 | 50.0 ± 21.1 | 49.4 ± 21.5 |
| FFM (%) | 47.8 ± 4.7 | 48.2 ± 4.6 | 51.4 ± 7.0 | 50.9 ± 9.0 |
| FM (kg) | 60.4 ± 8.8 | 58.3 ± 8.4 | 49.9 ± 20.2 | 49.0 ± 20.4 |
| FM (%) | 52.2 ± 4.7 | 51.8 ± 4.6 | 48.6 ± 7.0 | 48.6 ± 8.1 |
| Glucose (mg/dL) | 88.3 ± 8.8 | 86.4 ± 6.9 | 87.1 ± 6.2 | 82.3 ± 6.1 b |
| Insulin (mU/L) | 17.8 ± 6.0 | 19.1 ± 7.4 | 18.3 ± 6.9 | 17.7 ± 5.9 |
| HOMA-IR | 3.9 ± 1.4 | 4.1 ± 1.1 | 4.0 ± 1.7 | 3.6 ± 1.4 |
| T-C (mg/dL) | 148.7 ± 28.3 | 141.9 ± 31.5 | 166.2 ± 33.9 | 160.1 ± 21.2 |
| HDL-C (mg/dL) | 46.0 ± 10.3 | 45.7 ± 11.3 | 39.7 ± 8.4 | 40.4 ± 9.2 |
| LDL-C (mg/dL) | 85.4 ± 28.6 | 77.7 ± 28.0 | 106.0 ± 30.4 | 99.2 ± 17.5 |
| TG (mg/dL) | 102.9 ± 43.7 | 111.9 ± 47.0 | 145.3 ± 77.3 | 123.6 ± 43.3 |
| HbA1c (%) | 5.2 ± 0.5 | 5.2 ± 0.5 | 5.3 ± 0.3 | 5.1 ± 0.3 b |
| hs-CRP (mg/dL) | 0.56 ± 0.4 | 0.69 ± 0.9 | 0.50 ± 0.4 | 0.3 ± 0.3 |
| NLR | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.7 ± 0.3 | 1.3 ± 0.4 b |
| Comparison | Diff. of Means | t | p |
|---|---|---|---|
| Comparisons for factor: TREATMENT | |||
| MELATONIN vs. PLACEBO | 70.306 | 2.054 | 0.044 |
| Comparisons for factor: EXERCISE | |||
| T0 vs. T30 | 7.083 | 0.207 | 0.837 |
| Comparisons for factor: BWRP | |||
| G1 vs. G15 | 0.361 | 0.0105 | 0.992 |
| Comparison | Diff. of Means | t | p |
|---|---|---|---|
| Comparisons for factor: TREATMENT | |||
| MELATONIN vs. PLACEBO | 27.462 | 1.124 | 0.265 |
| Comparisons for factor: EXERCISE | |||
| T30 vs. T0 | 42.664 | 1.746 | 0.086 |
| Comparisons for factor: BWRP | |||
| G15 vs. G1 | 76.828 | 3.144 | 0.003 |
| Comparison | Diff. of Means | t | p |
|---|---|---|---|
| Comparisons for factor: TREATMENT | |||
| PLACEBO vs. MELATONIN | 0.117 | 0.204 | 0.839 |
| Comparisons for factor: EXERCISE | |||
| T30 vs. T0 | 0.739 | 1.295 | 0.200 |
| Comparisons for factor: BWRP | |||
| G1 vs. G15 | 0.689 | 1.207 | 0.232 |
| Comparisons for factor: BWRP within PLACEBO | |||
| G1 vs. G15 | 2.772 | 3.435 | 0.001 |
| Comparisons for factor: BWRP within MELATONIN | |||
| G15 vs. G1 | 1.394 | 1.728 | 0.089 |
| Comparisons for factor: TREATMENT within G1 | |||
| PLACEBO vs. MELATONIN | 2.200 | 2.726 | 0.008 |
| Comparisons for factor: TREATMENT within G15 | |||
| MELATONIN vs. PLACEBO | 1.967 | 2.437 | 0.018 |
| Comparison | Diff. of Means | t | p |
|---|---|---|---|
| Comparisons for factor: TREATMENT | |||
| MELATONIN vs. PLACEBO | 0.0228 | 4.611 | <0.001 |
| Comparisons for factor: EXERCISE | |||
| T90 vs. T0 | 0.0184 | 2.630 | 0.058 |
| T90 vs. T30 | 0.0101 | 1.439 | 0.916 |
| T90 vs. T150 | 0.00285 | 0.404 | 1.000 |
| T150 vs. T0 | 0.0156 | 2.223 | 0.168 |
| T150 vs. T30 | 0.00722 | 1.032 | 1.000 |
| T30 vs. T0 | 0.00833 | 1.200 | 1.000 |
| Comparisons for factor: BWRP | |||
| G15 vs. G1 | 0.0120 | 2.421 | 0.017 |
| Comparisons for factor: EXERCISE within MELATONIN | |||
| T90 vs. T0 | 0.0374 | 3.747 | 0.002 |
| T90 vs. T30 | 0.0168 | 1.685 | 0.566 |
| T90 vs. T150 | 0.00514 | 0.508 | 1.000 |
| T150 vs. T0 | 0.0322 | 3.232 | 0.009 |
| T150 vs. T30 | 0.0117 | 1.170 | 1.000 |
| T30 vs. T0 | 0.0206 | 2.093 | 0.230 |
| Comparisons for factor: EXERCISE within PLACEBO | |||
| T0 vs. T30 | 0.00389 | 0.396 | 1.000 |
| T0 vs. T150 | 0.00111 | 0.113 | 1.000 |
| T0 vs. T90 | 0.000556 | 0.0566 | 1.000 |
| T90 vs. T30 | 0.00333 | 0.339 | 1.000 |
| T90 vs. T150 | 0.000556 | 0.0566 | 1.000 |
| T150 vs. T30 | 0.00278 | 0.283 | 1.000 |
| Comparisons for factor: TREATMENT within T0 | |||
| PLACEBO vs. MELATONIN | 0.00111 | 0.113 | 0.910 |
| Comparisons for factor: TREATMENT within T30 | |||
| MELATONIN vs. PLACEBO | 0.0233 | 2.376 | 0.019 |
| Comparisons for factor: TREATMENT within T90 | |||
| MELATONIN vs. PLACEBO | 0.0368 | 3.691 | <0.001 |
| Comparisons for factor: TREATMENT within T150 | |||
| MELATONIN vs. PLACEBO | 0.0322 | 3.232 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigamonti, A.E.; Rubino, F.M.; Caroli, D.; Bondesan, A.; Mai, S.; Cella, S.G.; Centofanti, L.; Paroni, R.; Sartorio, A. Effects of Melatonin on Exercise-Induced Oxidative Stress in Adults with Obesity Undergoing a Multidisciplinary Body Weight Reduction Program. J. Clin. Med. 2024, 13, 5216. https://doi.org/10.3390/jcm13175216
Rigamonti AE, Rubino FM, Caroli D, Bondesan A, Mai S, Cella SG, Centofanti L, Paroni R, Sartorio A. Effects of Melatonin on Exercise-Induced Oxidative Stress in Adults with Obesity Undergoing a Multidisciplinary Body Weight Reduction Program. Journal of Clinical Medicine. 2024; 13(17):5216. https://doi.org/10.3390/jcm13175216
Chicago/Turabian StyleRigamonti, Antonello E., Federico M. Rubino, Diana Caroli, Adele Bondesan, Stefania Mai, Silvano G. Cella, Lucia Centofanti, Rita Paroni, and Alessandro Sartorio. 2024. "Effects of Melatonin on Exercise-Induced Oxidative Stress in Adults with Obesity Undergoing a Multidisciplinary Body Weight Reduction Program" Journal of Clinical Medicine 13, no. 17: 5216. https://doi.org/10.3390/jcm13175216
APA StyleRigamonti, A. E., Rubino, F. M., Caroli, D., Bondesan, A., Mai, S., Cella, S. G., Centofanti, L., Paroni, R., & Sartorio, A. (2024). Effects of Melatonin on Exercise-Induced Oxidative Stress in Adults with Obesity Undergoing a Multidisciplinary Body Weight Reduction Program. Journal of Clinical Medicine, 13(17), 5216. https://doi.org/10.3390/jcm13175216