

Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning
 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods

{kind=link}
{kind=link}
{kind=link}
| ICU Event | Definition |
|---|---|
| CPR | Any CPR delivered |
| Reintubation | Reintubation for any reason other than revision surgery |
| Return to OR | Any surgery due to complications within 24 h |
| Mechanical ventilation | Any postoperative ventilation > 4 h |
| Vasopressors | Continuous application of more than 0.4 mg/h norepinephrine |
| Impaired consciousness | GCS < 13 |
| Intracranial hypertension | CSF drainage or administration of mannitol due to ICP > 20 mmHg |
| Swallowing Disorder | Impaired swallowing requiring a gastral tube or parenteral nutrition |
| Death in the perioperative period | Any death within 48 h post-surgery |
3. Results
3.1. Summary of Prognostic Features
3.2. Postoperative Events
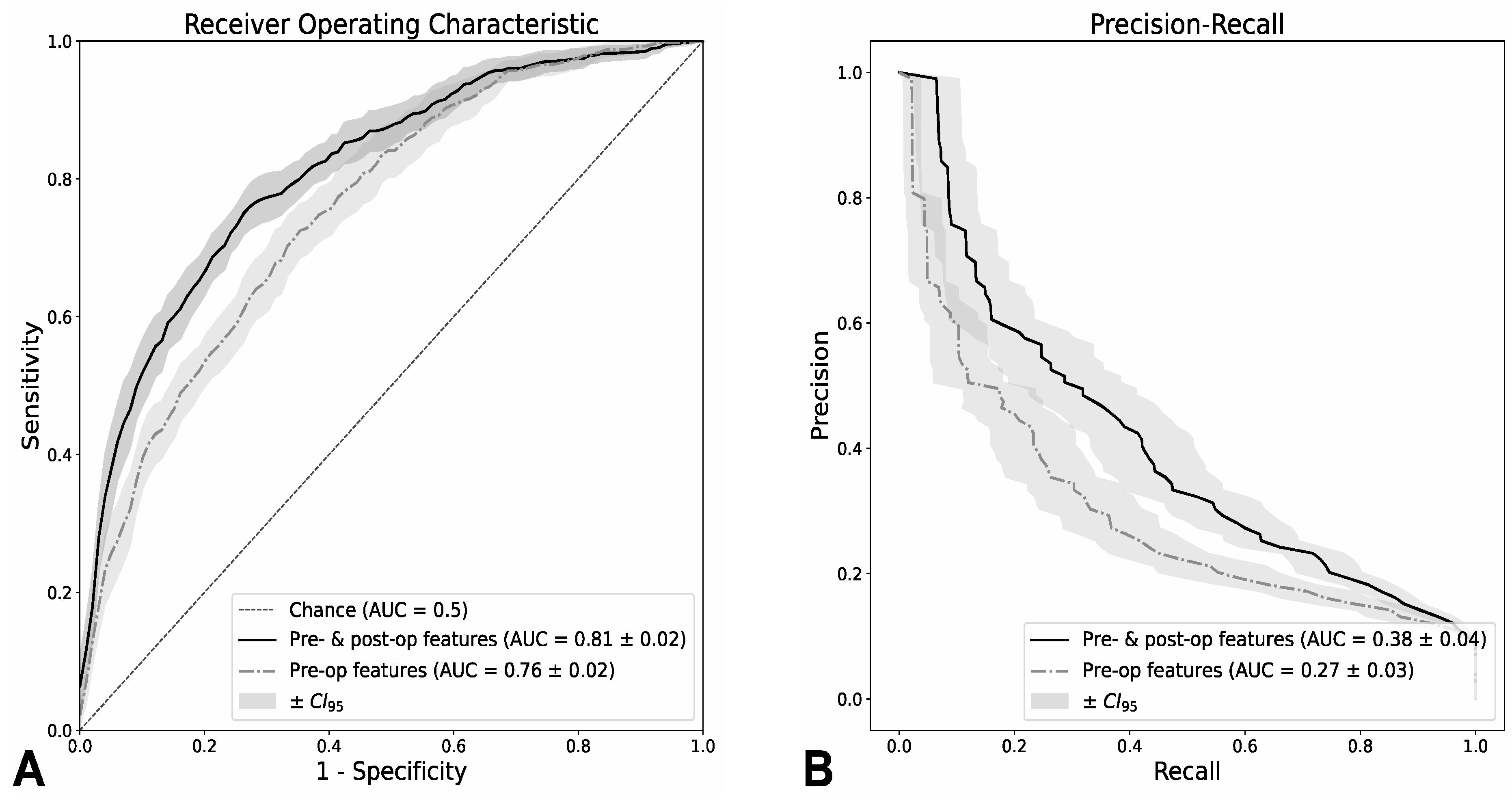
3.3. Classification Performance
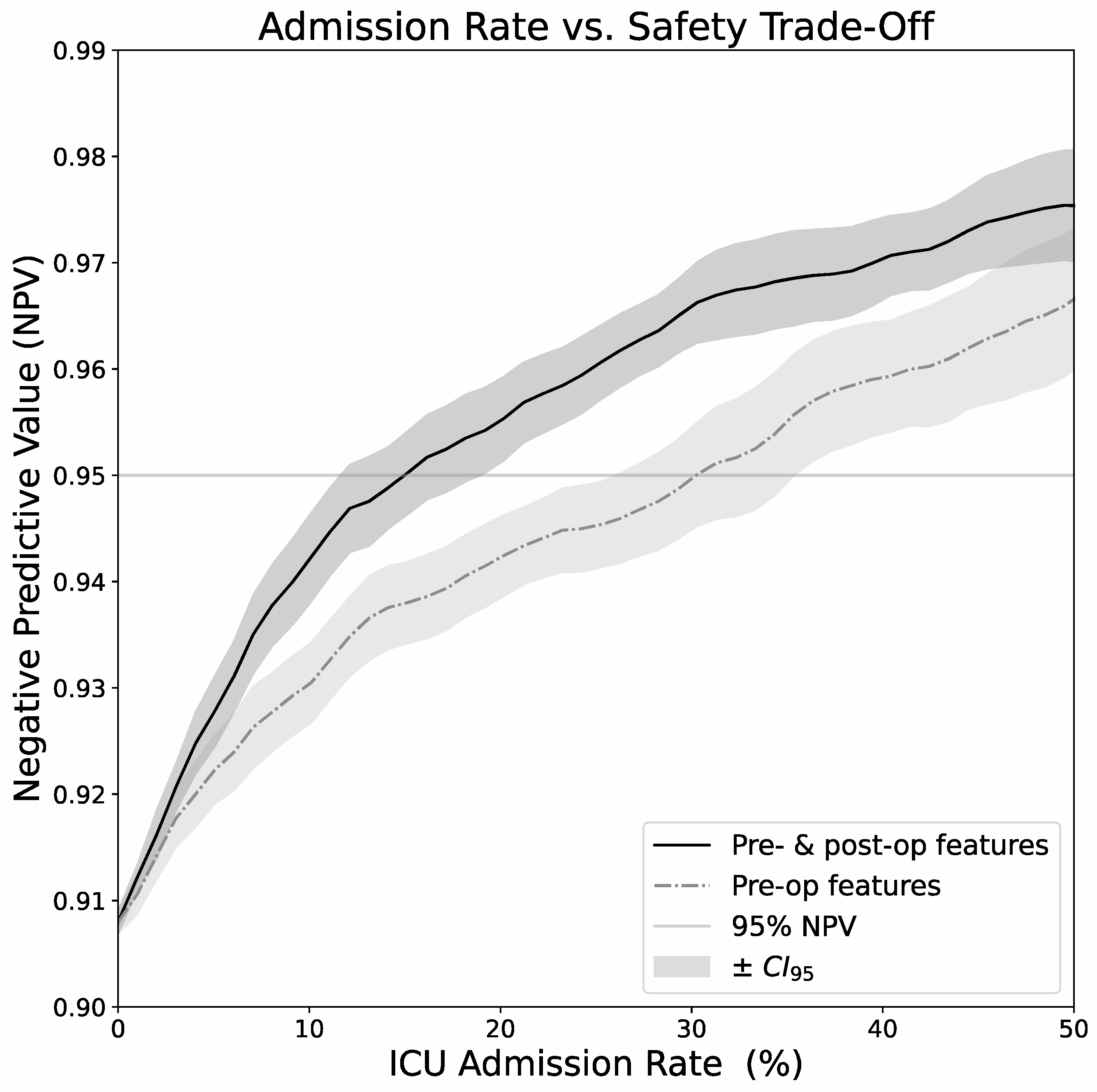
3.4. Calibration and Admission Rate/Safety Tradeoff
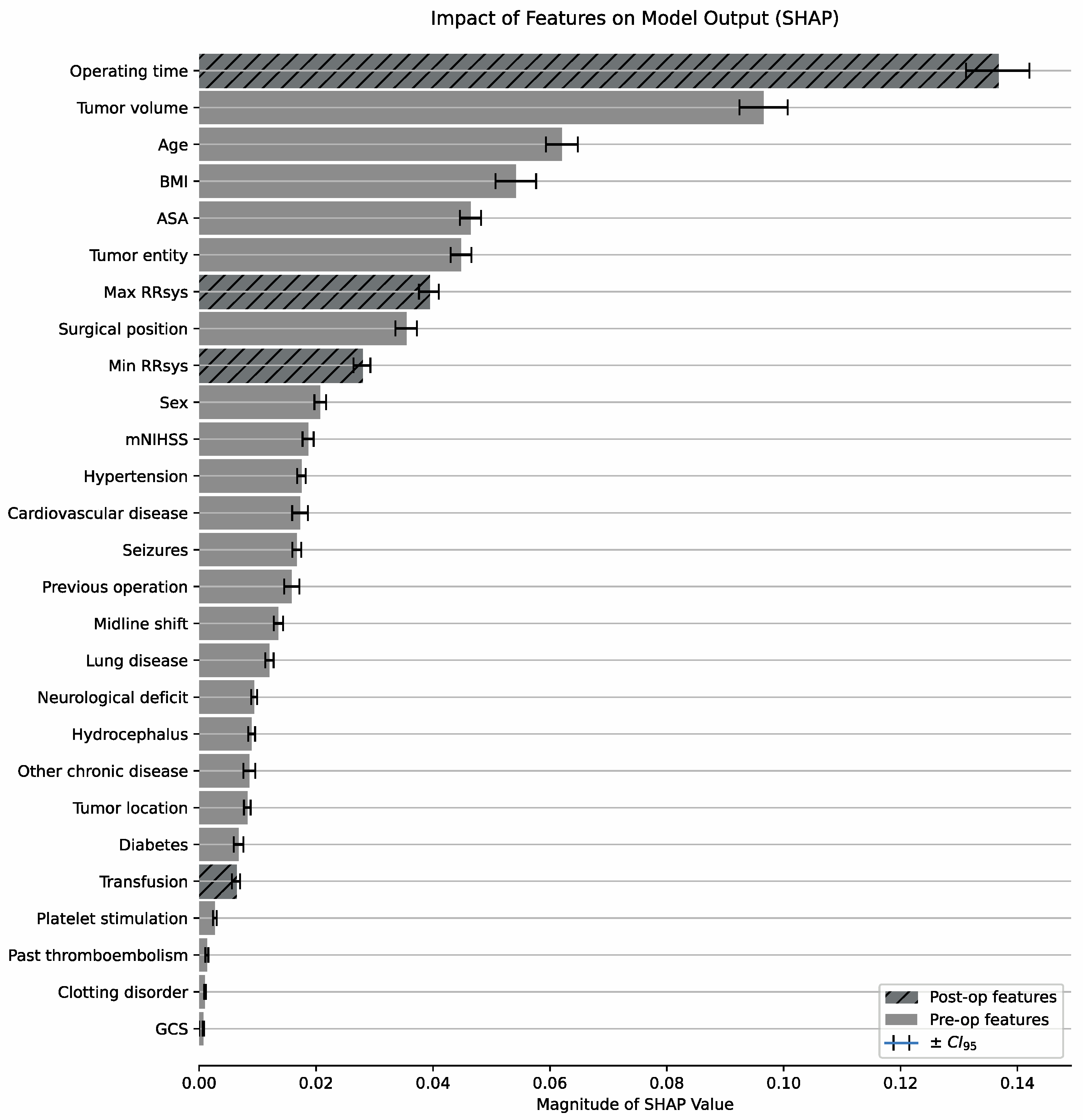
3.5. Relative Importance of Prognostic Features
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Ziai, W.C.; Varelas, P.N.; Zeger, S.L.; Mirski, M.A.; Ulatowski, J.A. Neurologic intensive care resource use after brain tumor surgery: An analysis of indications and alternative strategies. Crit. Care Med. 2003, 31, 2782–2787. [Google Scholar] [CrossRef] [PubMed]
- Beauregard, C.L.; Friedman, W.A. Routine use of postoperative ICU care for elective craniotomy: A cost-benefit analysis. Surg. Neurol. 2003, 60, 483–489, dicussion 489. [Google Scholar] [CrossRef] [PubMed]
- Bui, J.Q.H.; Mendis, R.L.; van Gelder, J.M.; Sheridan, M.M.P.; Wright, K.M.; Jaeger, M. Is postoperative intensive care unit admission a prerequisite for elective craniotomy? J. Neurosurg. 2011, 115, 1236–1241. [Google Scholar] [CrossRef] [PubMed]
- Hanak, B.W.; Walcott, B.P.; Nahed, B.V.; Muzikansky, A.; Mian, M.K.; Kimberly, W.T.; Curry, W.T. Postoperative intensive care unit requirements after elective craniotomy. World Neurosurg. 2014, 81, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.F. Neurosurgical postoperative care. Neurosurg. Clin. N. Am. 1994, 5, 789–810. [Google Scholar] [CrossRef] [PubMed]
- Colon, G.D.R.; Ohkuma, R.; Pendharkar, A.V.; Heifets, B.D.; Li, G.; Lu, A.; Gephart, M.H.; Ratliff, J.K. A Protocol for Reducing Intensive Care Utilization after Craniotomy: A 3-Year Assessment. Neurosurgery 2023, 92, 1080–1090. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.Z.; Babayan, D.; Chen, J.-S.; Wang, M.M.; Naik, P.K.; Reitz, K.; Li, J.J.; Pouratian, N.; Kim, W. Postoperative Admission of Adult Craniotomy Patients to the Neuroscience Ward Reduces Length of Stay and Cost. Neurosurgery 2021, 89, 85–93. [Google Scholar] [CrossRef] [PubMed]
- de Almeida, C.C.; Boone, M.D.; Laviv, Y.; Kasper, B.S.; Chen, C.C.; Kasper, E.M. The Utility of Routine Intensive Care Admission for Patients Undergoing Intracranial Neurosurgical Procedures: A Systematic Review. Neurocrit. Care 2018, 28, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Schar, R.T.; Tashi, S.; Branca, M.; Soll, N.; Cipriani, D.; Schwarz, C.; Pollo, C.; Schucht, P.; Ulrich, C.T.; Beck, J.; et al. How safe are elective craniotomies in elderly patients in neurosurgery today? A prospective cohort study of 1452 consecutive cases. J. Neurosurg. 2020, 134, 1113–1121. [Google Scholar] [CrossRef]
- Solheim, O.; Jakola, A.S.; Gulati, S.; Johannesen, T.B. Incidence and causes of perioperative mortality after primary surgery for intracranial tumors: A national, population-based study. J. Neurosurg. 2012, 116, 825–834. [Google Scholar] [CrossRef]
- Azad, T.D.; Shah, P.P.; Kannapadi, N.V.; Rincon-Torroella, J.; Xia, Y.; Bernhardt, L.J.; Hansen, L.J.; Materi, J.; Raj, D.; Jackson, C.M.; et al. Reexamining the Role of Postoperative ICU Admission for Patients Undergoing Elective Craniotomy: A Systematic Review. Crit. Care Med. 2022, 50, 1380–1393. [Google Scholar] [CrossRef] [PubMed]
- Cinotti, R.; Bruder, N.; Srairi, M.; Paugam-Burtz, C.; Beloeil, H.; Pottecher, J.; Geeraerts, T.; Atthar, V.; Gueguen, A.; Triglia, T.; et al. Prediction Score for Postoperative Neurologic Complications after Brain Tumor Craniotomy: A Multicenter Observational Study. Anesthesiology 2018, 129, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Munari, M.; De Cassai, A.; Sandei, L.; Correale, C.; Calandra, S.; Iori, D.; Geraldini, F.; Vitalba, A.; Grandis, M.; Chioffi, F.; et al. Optimizing post anesthesia care unit admission after elective craniotomy for brain tumors: A cohort study. Acta Neurochir. 2022, 164, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Rozeboom, P.D.; Henderson, W.G.; Dyas, A.R.; Bronsert, M.R.; Colborn, K.L.; Lambert-Kerzner, A.; Hammermeister, K.E.; McIntyre, R.C., Jr.; Meguid, R.A. Development and Validation of a Multivariable Prediction Model for Postoperative Intensive Care Unit Stay in a Broad Surgical Population. JAMA Surg. 2022, 157, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Schipmann, S.; Spille, D.C.; Gallus, M.; Lohmann, S.; Schwake, M.; Warneke, N.; Molina, E.S.; Stummer, W.; Holling, M. Postoperative surveillance in cranial and spinal tumor neurosurgery: When is this warranted? J. Neurosurg. 2022, 138, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- Franko, L.R.; Hollon, T.; Linzey, J.; Roark, C.; Rajajee, V.; Sheehan, K.; Teig, M.; Hervey-Jumper, S.; Heth, J.; Orringer, D.; et al. Clinical Factors Associated with ICU-Specific Care Following Supratentoral Brain Tumor Resection and Validation of a Risk Prediction Score. Crit. Care Med. 2018, 46, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Schweppe, J.A.; Potthoff, A.L.; Heimann, M.; Ehrentraut, S.F.; Borger, V.; Lehmann, F.; Schaub, C.; Bode, C.; Putensen, C.; Herrlinger, U.; et al. Incurring detriments of unplanned readmission to the intensive care unit following surgery for brain metastasis. Neurosurg. Rev. 2023, 46, 155. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, F.; Potthoff, A.L.; Borger, V.; Heimann, M.; Ehrentraut, S.F.; Schaub, C.; Putensen, C.; Weller, J.; Bode, C.; Vatter, H.; et al. Unplanned intensive care unit readmission after surgical treatment in patients with newly diagnosed glioblastoma—Forfeiture of surgically achieved advantages? Neurosurg. Rev. 2023, 46, 30. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.E.; Gupta, S.; O’Connor, M.; Jarvis, C.A.; Zhao, M.; Hauser, B.M.; Bernstock, J.D.; Murphy, S.; Raftery, S.M.; Lane, K.; et al. Reduced time to imaging, length of stay, and hospital charges following implementation of a novel postoperative pathway for craniotomy. J. Neurosurg. 2023, 39, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Neumann, J.O.; Schmidt, S.; Nohman, A.; Jakobs, M.; Unterberg, A. Routine ICU admission after brain tumor surgery: Retrospective validation and critical appraisal of two prediction scores. Acta Neurochir. 2023, 65, 1655–1664. [Google Scholar] [CrossRef] [PubMed]
- van Niftrik, C.H.B.; van der Wouden, F.; Staartjes, V.E.; Fierstra, J.; Stienen, M.N.; Akeret, K.; Sebök, M.; Fedele, T.; Sarnthein, J.; Bozinov, O.; et al. Machine Learning Algorithm Identifies Patients at High Risk for Early Complications after Intracranial Tumor Surgery: Registry-Based Cohort Study. Neurosurgery 2019, 85, E756–E764. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Niculescu-Mizil, A.; Caruana, R. Predicting Good Probabilities with Supervised Learning. In Proceedings of the 22nd International Conference on Machine Learning, Bonn, Germany, 7–11 August 2005. [Google Scholar]
- Lundberg, S.M.; Lee, S.-I. Consisted feature attribution for tree ensembles. In Proceedings of the 34th International Conference on Machine Learning, Sydney, Australia, 6–11 August 2017. [Google Scholar]
- Pendharkar, A.V.; Shahin, M.N.; Awsare, S.S.; Ho, A.L.; Wachira, C.; Clevinger, J.; Sigurdsson, S.; Lee, Y.; Wilson, A.; Lu, A.C.; et al. A Novel Protocol for Reducing Intensive Care Utilization after Craniotomy. Neurosurgery 2021, 89, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Laan, M.T.; Bartels, R.H. “No-ICU-Unless” Policy for Tumor Craniotomy. World Neurosurg. 2020, 136, 406. [Google Scholar] [CrossRef] [PubMed]
- Qasem, L.-E.; Al-Hilou, A.; Zacharowski, K.; Funke, M.; Strouhal, U.; Reitz, S.C.; Jussen, D.; Forster, M.T.; Konczalla, J.; Prinz, V.M.; et al. Implementation of the “No ICU–Unless” approach in postoperative neurosurgical management in times of COVID-19. Neurosurg. Rev. 2022, 45, 3437–3446. [Google Scholar] [CrossRef] [PubMed]
- Akiba, T.; Sano, S.; Yanase, T.; Ohta, T.; Koyama, M. Optuna: A Next-generation Hyperparameter Optimization Framework. In Proceedings of the 25th ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Anchorage, AK, USA, 4–8 August 2019. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
| Prognostic Features (27 Total) | Values |
|---|---|
| Demographics (3) | |
| Age | 18–88 years (57 ± 15) 1 |
| Sex | 55% female, 45% male |
| BMI | 13–46 (26 ± 5) * |
| Preoperative conditions (4) | |
| ASA | I (6%) II (58%) III (36%) IV (1%) V (0%) |
| mNIHSS | 0–11, median 0, IQR 0–1 |
| GCS | 11–15, median 15, IQR 15–15 |
| Any neurologic deficit | 63% |
| Past medical history (10) | |
| Diabetes mellitus | 11% |
| Arterial Hypertension | 41% |
| Clotting disorder | 2% |
| Thromboembolism | 4% |
| Seizures | 26% |
| Prior neurosurgery | 23% |
| Antiplatelet or anticoagulation meds | 14% |
| Cardiovascular disease | 14% |
| Lung disease 1 | 56% |
| Other chronic diseases | 14% |
| Tumor characteristics (5) | |
| Hydrocephalus on MRI | 6% |
| Location of tumor | 78% supratentorial 22% infratentorial |
| Midline shift (>3 mm) on MRI | 19% |
| Suspected entity | 36% meningioma, 19% metastasis, 16% glioblastoma, 28% other |
| Tumor volume 2 | 1–272 mL (22 ± 31) |
| Intra- and postoperative data (4 + 1) | |
| Positioning | supine 67% prone 13%, lateral 7% sitting 13% |
| Duration of surgery (min) | 20–740 min (236 ± 102) |
| Maximum systolic blood pressure (mmHg) | 90–180 (135 ± 16) |
| Minimum systolic blood pressure (mmHg) | 50–140 (100 ± 10) |
| Transfusion of red blood cells, platelets or plasma | 2% |
| Postoperative Events | No. of Cases (n = 1000) |
|---|---|
| ICU events | 149 |
| Cases with events | 92 (9.2%) |
| CPR | 4 (0.4%) |
| Return to OR | 12 (1.2%) |
| Continued mechanical ventilation | 25 (2.5%) |
| Vasopressors | 22 (2.2%) |
| Impaired consciousness | 34 (3.4%) |
| Intracranial hypertension | 22 (2.2%) |
| Swallowing Disorder | 17 (1.7%) |
| Death in the perioperative period | 0 (0.0%) |
| Other events | 540 |
| Cases with events | 351 (35.1%) |
| Any cranial nerve deficit | 72 (7.2%) |
| Hemiparesis (≤3/5) | 46 (4.6%) |
| Administration of mannitol | 47 (4.7%) |
| Postoperative CT scan | 99 (9.9%) |
| Seizure | 42 (4.2%) |
| I.V. blood pressure medication | 47 (4.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neumann, J.-O.; Schmidt, S.; Nohman, A.; Naser, P.; Jakobs, M.; Unterberg, A. Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning. J. Clin. Med. 2024, 13, 5747. https://doi.org/10.3390/jcm13195747
Neumann J-O, Schmidt S, Nohman A, Naser P, Jakobs M, Unterberg A. Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning. Journal of Clinical Medicine. 2024; 13(19):5747. https://doi.org/10.3390/jcm13195747
Chicago/Turabian StyleNeumann, Jan-Oliver, Stephanie Schmidt, Amin Nohman, Paul Naser, Martin Jakobs, and Andreas Unterberg. 2024. "Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning" Journal of Clinical Medicine 13, no. 19: 5747. https://doi.org/10.3390/jcm13195747
APA StyleNeumann, J.-O., Schmidt, S., Nohman, A., Naser, P., Jakobs, M., & Unterberg, A. (2024). Routine ICU Surveillance after Brain Tumor Surgery: Patient Selection Using Machine Learning. Journal of Clinical Medicine, 13(19), 5747. https://doi.org/10.3390/jcm13195747