
Capillary Refill Time as a Part of Routine Physical Examination in Critically Ill Patients Undergoing Vasoactive Therapy: A Prospective Study
 ,
, 
Abstract
1. Introduction
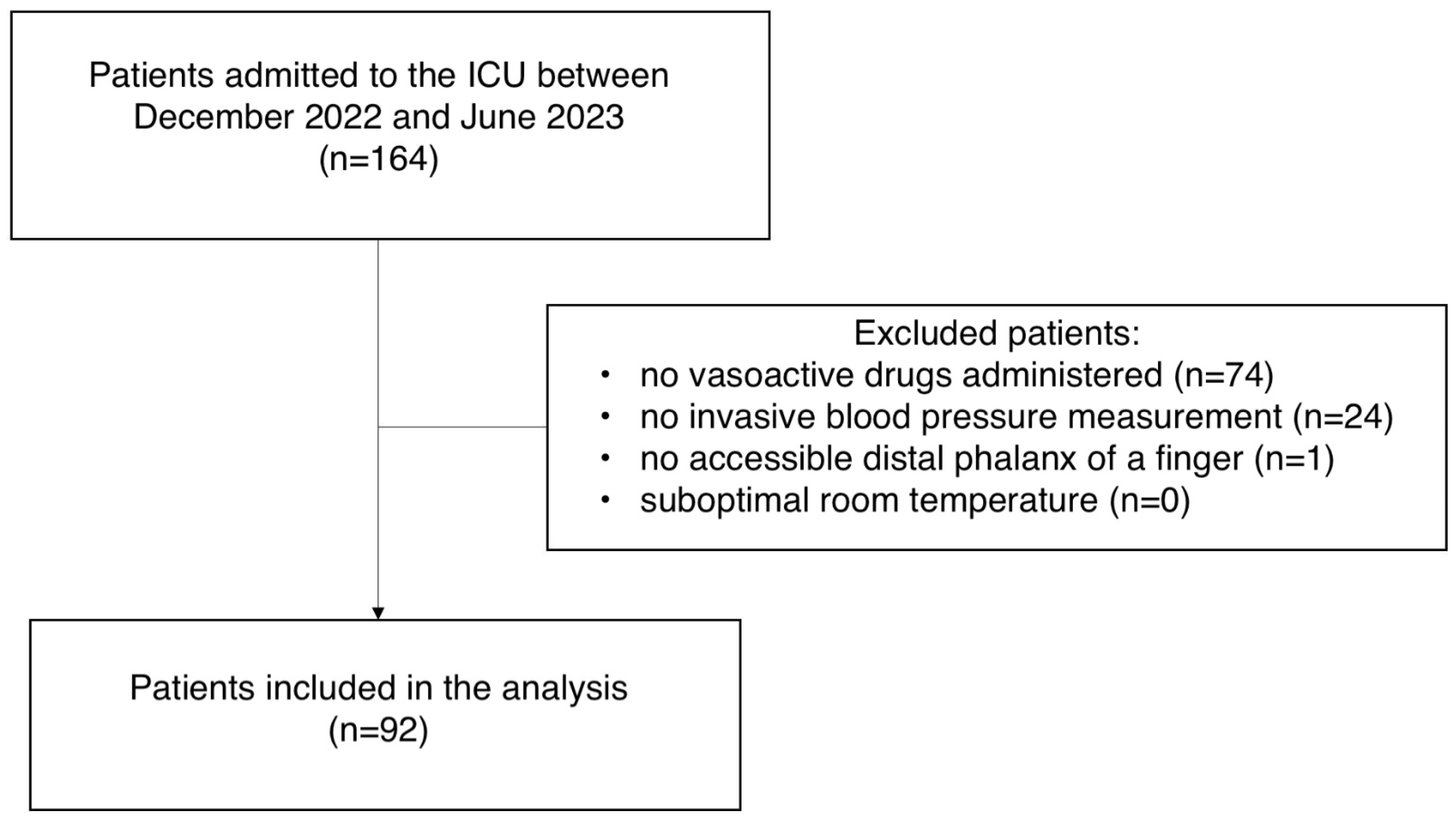
2. Material and Methods
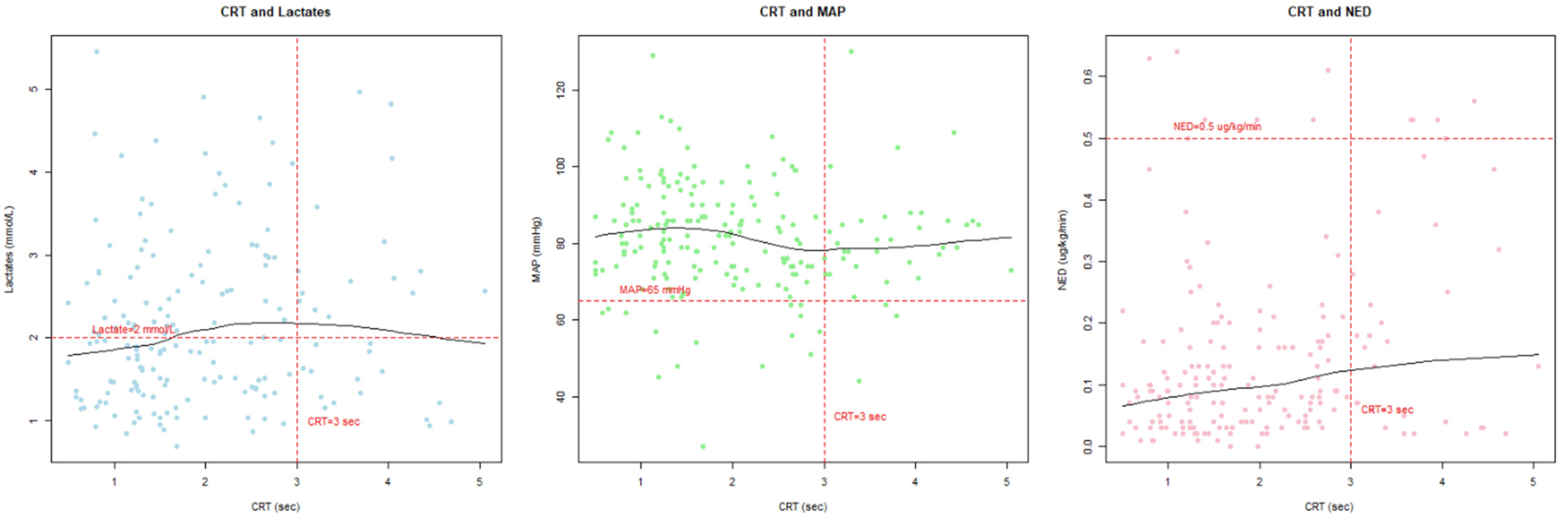
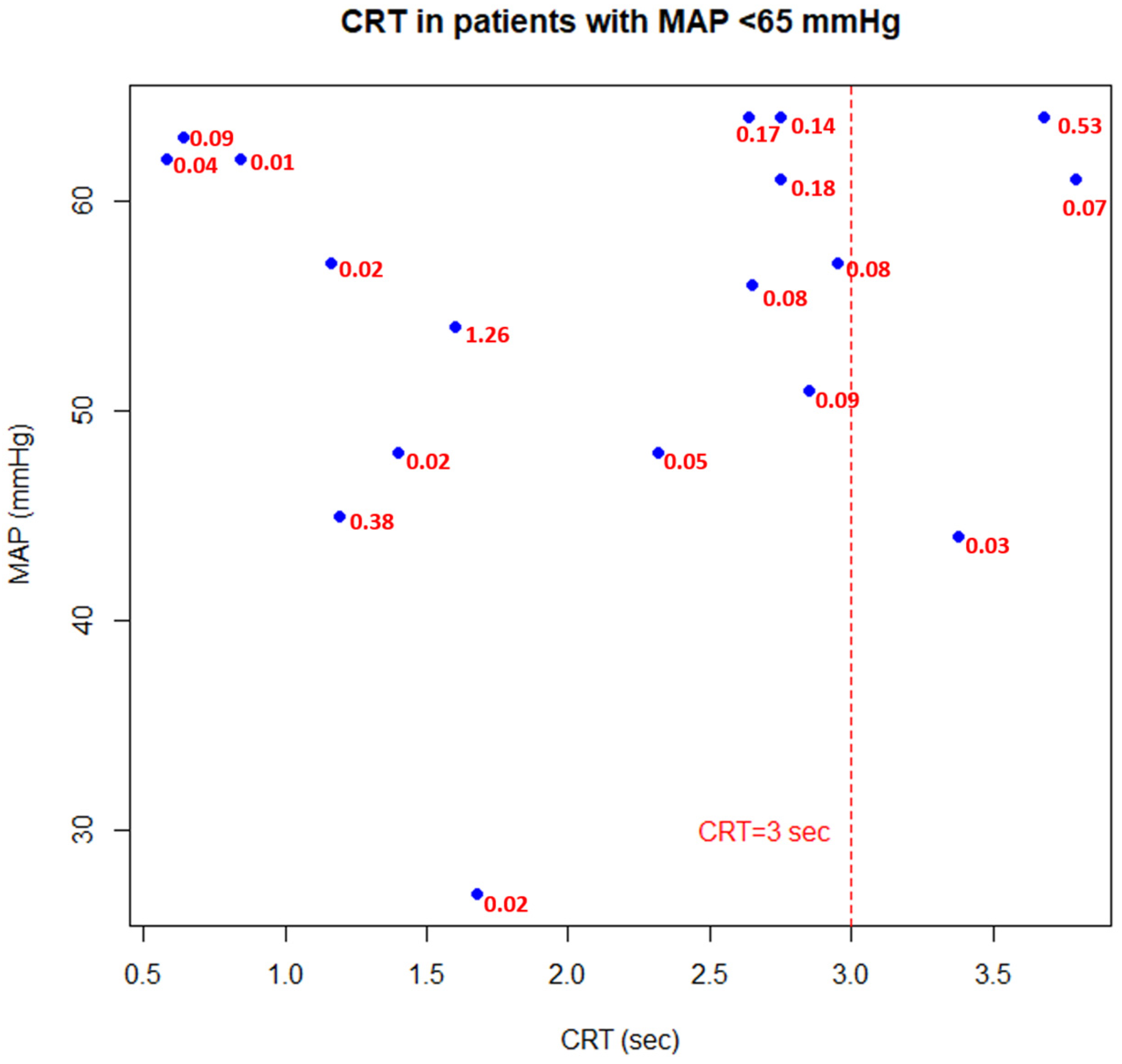
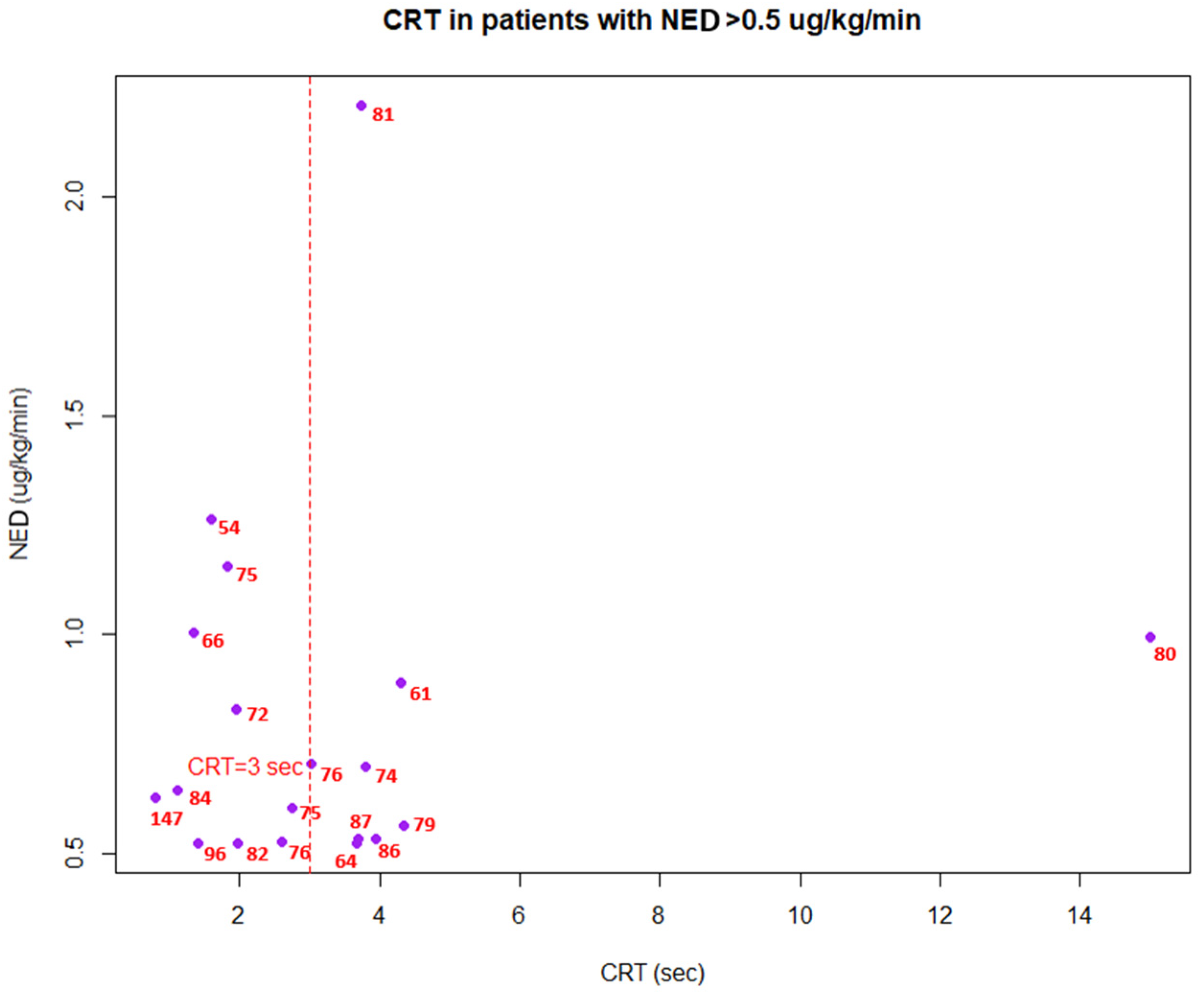
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MAP | Mean Arterial Pressure |
| CRT | Capillary Refill Time |
| NED | Norepinephrine Equivalent Dose |
| SSC | Surviving Sepsis Campaign |
| ICU | Intensive Care Unit |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| IQR | Interquartile Range |
| SAH | Subarachnoid Hemorrhage |
| PLR | Passive Leg Raising |
References
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Barrett, K.E.; Barman, S.M.; Brooks, H.L.; Yuan, J.X.J.; Ganong, W.F. Ganong’s Review of Medical Physiology, 26th ed.; McGraw-Hill Education: New York, NY, USA, 2019. [Google Scholar]
- Kato, R.; Pinsky, M.R. Personalizing blood pressure management in septic shock. Ann. Intensive Care 2015, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Hernández, G.; Ospina-Tascón, G.A.; Damiani, L.P.; Estenssoro, E.; Dubin, A.; Hurtado, J.; Friedman, G.; Castro, R.; Alegría, L.; Teboul, J.L.; et al. Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients with Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA 2019, 321, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Misango, D.; Pattnaik, R.; Baker, T.; Dünser, M.W.; Dondorp, A.M.; Schultz, M.J. Haemodynamic assessment and support in sepsis and septic shock in resource-limited settings. Trans. R Soc. Trop. Med. Hyg. 2017, 111, 483–489. [Google Scholar] [CrossRef]
- Ait-Oufella, H.; Bige, N.; Boelle, P.Y.; Pichereau, C.; Alves, M.; Bertinchamp, R.; Baudel, J.L.; Galbois, A.; Maury, E.; Guidet, B. Capillary refill time exploration during septic shock. Intensive Care Med. 2014, 40, 958–964. [Google Scholar] [CrossRef]
- Brunauer, A.; Koköfer, A.; Bataar, O.; Gradwohl-Matis, I.; Dankl, D.; Bakker, J.; Dünser, M.W. Changes in peripheral perfusion relate to visceral organ perfusion in early septic shock: A pilot study. J. Crit. Care 2016, 35, 105–109. [Google Scholar] [CrossRef]
- Morocho, J.P.; Martínez, A.F.; Cevallos, M.M.; Vasconez-Gonzalez, J.; Ortiz-Prado, E.; Barreto-Grimaldos, A.; Vélez-Páez, J.L. Prolonged Capillary Refilling as a Predictor of Mortality in Patients With Septic Shock. J. Intensive Care Med. 2022, 37, 423–429. [Google Scholar] [CrossRef]
- Kattan, E.; Hernández, G.; Ospina-Tascón, G.; Valenzuela, E.D.; Bakker, J.; Castro, R. A lactate-targeted resuscitation strategy may be associated with higher mortality in patients with septic shock and normal capillary refill time: A post hoc analysis of the ANDROMEDA-SHOCK study. Ann. Intensive Care 2020, 10, 114. [Google Scholar] [CrossRef]
- Zampieri, F.G.; Damiani, L.P.; Bakker, J.; Ospina-Tascón, G.A.; Castro, R.; Cavalcanti, A.B.; Hernandez, G. Effects of a Resuscitation Strategy Targeting Peripheral Perfusion Status versus Serum Lactate Levels among Patients with Septic Shock. A Bayesian Reanalysis of the ANDROMEDA-SHOCK Trial. Am. J. Respir. Crit. Care Med. 2020, 201, 423–429. [Google Scholar] [CrossRef]
- Lara, B.; Enberg, L.; Ortega, M.; Leon, P.; Kripper, C.; Aguilera, P.; Kattan, E.; Castro, R.; Bakker, J.; Hernandez, G. Capillary refill time during fluid resuscitation in patients with sepsis-related hyperlactatemia at the emergency department is related to mortality. PLoS ONE 2017, 12, e0188548. [Google Scholar] [CrossRef] [PubMed]
- Kotani, Y.; Di Gioia, A.; Landoni, G.; Belletti, A.; Khanna, A.K. An updated “norepinephrine equivalent” score in intensive care as a marker of shock severity. Crit. Care 2023, 27, 29. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Jacquet-Lagrèze, M.; Bouhamri, N.; Portran, P.; Schweizer, R.; Baudin, F.; Lilot, M.; Fornier, W.; Fellahi, J.L. Capillary refill time variation induced by passive leg raising predicts capillary refill time response to volume expansion. Crit. Care 2019, 23, 281. [Google Scholar] [CrossRef] [PubMed]
- Raia, L.; Gabarre, P.; Bonny, V.; Urbina, T.; Missri, L.; Boelle, P.Y.; Baudel, J.L.; Guidet, B.; Maury, E.; Joffre, J.; et al. Kinetics of capillary refill time after fluid challenge. Ann. Intensive Care 2022, 12, 74. [Google Scholar] [CrossRef]
- Hernández, G.; Valenzuela, E.D.; Kattan, E.; Castro, R.; Guzmán, C.; Kraemer, A.E.; Sarzosa, N.; Alegría, L.; Contreras, R.; Oviedo, V.; et al. Capillary refill time response to a fluid challenge or a vasopressor test: An observational, proof-of-concept study. Ann. Intensive Care 2024, 14, 49. [Google Scholar] [CrossRef]
- Dubin, A.; Pozo, M.O.; Casabella, C.A.; Pálizas, F., Jr.; Murias, G.; Moseinco, M.C.; Kanoore Edul, V.S.; Pálizas, F.; Estenssoro, E.; Ince, C.; et al. Increasing arterial blood pressure with norepinephrine does not improve microcirculatory blood flow: A prospective study. Crit. Care. 2009, 13, R92. [Google Scholar] [CrossRef]
- Lima, A.; Jansen, T.C.; Van Bommel, J.; Ince, C.; Bakker, J. The prognostic value of the subjective assessment of peripheral perfusion in critically ill patients. Crit. Care Med. 2009, 37, 934–938. [Google Scholar] [CrossRef]
- Landry, G.J.; Mostul, C.J.; Ahn, D.S.; McLafferty, B.J.; Liem, T.K.; Mitchell, E.L.; Jung, E.; Abraham, C.Z.; Azarbal, A.F.; McLafferty, R.B.; et al. Causes and outcomes of finger ischemia in hospitalized patients in the intensive care unit. J. Vasc. Surg. 2018, 68, 1499–1504. [Google Scholar] [CrossRef]
- Anderson, B.; Kelly, A.M.; Kerr, D.; Clooney, M.; Jolley, D. Impact of patient and environmental factors on capillary refill time in adults. Am. J. Emerg. Med. 2008, 26, 62–65. [Google Scholar] [CrossRef]
- Brown, L.H.; Prasad, N.H.; Whitley, T.W. Adverse lighting condition effects on the assessment of capillary refill. Am. J. Emerg. Med. 1994, 12, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, R.; Nakada, T.; Oshima, T.; Shinozaki, M.; Nakaguchi, T.; Haneishi, H.; Oda, S. Optimal pressing strength and time for capillary refilling time. Crit. Care 2019, 23, 4. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Morton, R.; Bevan, C. How to use capillary refill time. Arch. Dis. Child. 2014, 99, 111–116. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 92) |
|---|---|
| Age—median (IQR), years | 66 (45–72) |
| Gender—n (%) | |
| Female | 45 (49%) |
| Male | 47 (51%) |
| CRT—median (IQR), s | 1.9 (1.25–2.75) |
| MAP—median (IQR), mmHg | 82 (74–90) |
| Lactate—median (IQR), mmol/L | 2.1 (1.46–3.1) |
| NED—median (IQR), μg/kg/min | 0.01 (0.04–0.20) |
| ICU mortality—n (%) | 39 (42%) |
| Cause of admission—n(%) | |
| Acute respiratory failure | 32 (34.8%) |
| Subarachnoid hemorrhage (SAH) | 21 (22.8%) |
| Acute neurological disease (other than SAH) | 17 (18.5%) |
| Acute pancreatitis | 5 (5.4%) |
| Sudden cardiac arrest | 4 (4.3%) |
| Acute heart failure | 3 (3.3%) |
| Septic shock | 3 (3.3%) |
| Shock (other than septic) | 3 (3.3%) |
| Acute liver failure | 2 (2.2%) |
| Malignant neoplasm | 2 (2.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wesołek, F.; Putowski, Z.; Staniszewska, W.; Latacz, R.; Krzych, Ł.J. Capillary Refill Time as a Part of Routine Physical Examination in Critically Ill Patients Undergoing Vasoactive Therapy: A Prospective Study. J. Clin. Med. 2024, 13, 5782. https://doi.org/10.3390/jcm13195782
Wesołek F, Putowski Z, Staniszewska W, Latacz R, Krzych ŁJ. Capillary Refill Time as a Part of Routine Physical Examination in Critically Ill Patients Undergoing Vasoactive Therapy: A Prospective Study. Journal of Clinical Medicine. 2024; 13(19):5782. https://doi.org/10.3390/jcm13195782
Chicago/Turabian StyleWesołek, Fabian, Zbigniew Putowski, Wiktoria Staniszewska, Robert Latacz, and Łukasz J. Krzych. 2024. "Capillary Refill Time as a Part of Routine Physical Examination in Critically Ill Patients Undergoing Vasoactive Therapy: A Prospective Study" Journal of Clinical Medicine 13, no. 19: 5782. https://doi.org/10.3390/jcm13195782
APA StyleWesołek, F., Putowski, Z., Staniszewska, W., Latacz, R., & Krzych, Ł. J. (2024). Capillary Refill Time as a Part of Routine Physical Examination in Critically Ill Patients Undergoing Vasoactive Therapy: A Prospective Study. Journal of Clinical Medicine, 13(19), 5782. https://doi.org/10.3390/jcm13195782