

The Impact of Telemedicine during the COVID-19 Pandemic on Diabetes Management and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus (GDM)


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association Professional Practice Committee. 15. Management of Diabetes in Pregnancy: Standards of Care in Diabetes-2024. Diabetes Care 2024, 47 (Suppl. 1), S282–S294. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.; McIntyre, H.D.; Tsoi, K.Y.; Kapur, A.; Ma, R.C.; Dias, S.; Okong, P.; Hod, M.; Poon, L.C.; Smith, G.N.; et al. Pregnancy as an opportunity to prevent type 2 diabetes mellitus: FIGO Best Practice Advice. Int. J. Gynaecol. Obstet. 2023, 160 (Suppl. 1), 56–67. [Google Scholar] [CrossRef] [PubMed]
- Mendez, Y.; Alpuing Radilla, L.A.; Delgadillo Chabolla, L.E.; Castillo Cruz, A.; Luna, J.; Surani, S. Gestational diabetes mellitus and COVID-19: The epidemic during the pandemic. World J. Diabetes 2023, 14, 1178–1193. [Google Scholar] [CrossRef] [PubMed]
- Gregory, E.C.W.; Ely, D.M. Trends and Characteristics in Gestational Diabetes: United States, 2016–2020. Natl. Vital Stat. Rep. 2022, 71, 1–15. [Google Scholar] [PubMed]
- Zanardo, V.; Tortora, D.; Sandri, A.; Severino, L.; Mesirca, P.; Straface, G. COVID-19 pandemic: Impact on gestational diabetes mellitus prevalence. Diabetes Res. Clin. Pract. 2022, 183, 109149. [Google Scholar] [CrossRef] [PubMed]
- Mirsky, E.; Mastronardi, A.; Paudel, A.M.; Young, M.; Zite, N.; Maples, J. Comparison of the Prevalence of Gestational Diabetes Pre-COVID-19 Pandemic Versus During COVID-19 [A196]. Obstet. Gynecol. 2022, 139, 57S. [Google Scholar] [CrossRef]
- La Verde, M.; Torella, M.; Riemma, G.; Narciso, G.; Iavarone, I.; Gliubizzi, L.; Palma, M.; Morlando, M.; Colacurci, N.; De Franciscis, P. Incidence of gestational diabetes mellitus before and after the Covid-19 lockdown: A retrospective cohort study. J. Obstet. Gynaecol. Res. 2022, 48, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Eberle, C.; Stichling, S. Telemedical Approaches to Managing Gestational Diabetes Mellitus During COVID-19: Systematic Review. JMIR Pediatr. Parent. 2021, 4, e28630. [Google Scholar] [CrossRef] [PubMed]
- Nouhjah, S.; Jahanfar, S. Challenges of diabetes care management in developing countries with a high incidence of COVID-19: A brief report. Diabetes Metab. Syndr. 2020, 14, 731–732. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, H.D.; Gibbons, K.S.; Ma, R.C.W.; Tam, W.H.; Sacks, D.A.; Lowe, J.; Madsen, L.R.; Catalano, P.M. Testing for gestational diabetes during the COVID-19 pandemic. An evaluation of proposed protocols for the United Kingdom, Canada and Australia. Diabetes Res. Clin. Pract. 2020, 167, 108353. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Meehan, T.; Veerasingham, M.; Sivanesan, K. COVID-19 pandemic gestational diabetes screening guidelines: A retrospective study in Australian women. Diabetes Metab. Syndr. 2021, 15, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Munda, A.; Indihar, B.Š.; Okanovič, G.; Zorko, K.; Steblovnik, L.; Barlovič, D.P. Maternal and Perinatal Outcomes During the COVID-19 Epidemic in Pregnancies Complicated by Gestational Diabetes. Zdr. Varst. 2023, 62, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Kozica-Olenski, S.L.; Soldatos, G.; Marlow, L.; Cooray, S.D.; Boyle, J.A. Exploring the acceptability and experience of receiving diabetes and pregnancy care via telehealth during the COVID-19 pandemic: A qualitative study. BMC Pregnancy Childbirth 2022, 22, 932. [Google Scholar] [CrossRef] [PubMed]
- PeŐĀrez-Ferre, N.; Galindo, M.; FernaŐĀndez, M.D.; Velasco, V.; Runkle, I.; de la Cruz, M.J.; MartiŐĀn Rojas-Marcos, P.; Del Valle, L.; Calle-Pascual, A.L. The outcomes of gestational diabetes mellitus after a telecare approach are not inferior to traditional outpatient clinic visits. Int. J. Endocrinol. 2010, 2010, 386941. [Google Scholar] [CrossRef] [PubMed]
- Wilk, M.; Surowiec, P.; Matejko, B.; Wróbel, A.; Zięba-Parkitny, J.; Cyganek, K.; Huras, H.; Małecki, M.T. Diabetes Management Delivery and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus during the First Wave of the 2020 COVID-19 Pandemic: A Single-Reference Center Report. J. Diabetes Res. 2021, 2021, 5515902. [Google Scholar] [CrossRef] [PubMed]
 dispersion of patients on the x and y axes.
dispersion of patients on the x and y axes.
dispersion of patients on the x and y axes.
dispersion of patients on the x and y axes.
 diet treated patients;
diet treated patients;  insulin treated patients.
diet treated patients; insulin treated patients.
insulin treated patients.
diet treated patients; insulin treated patients.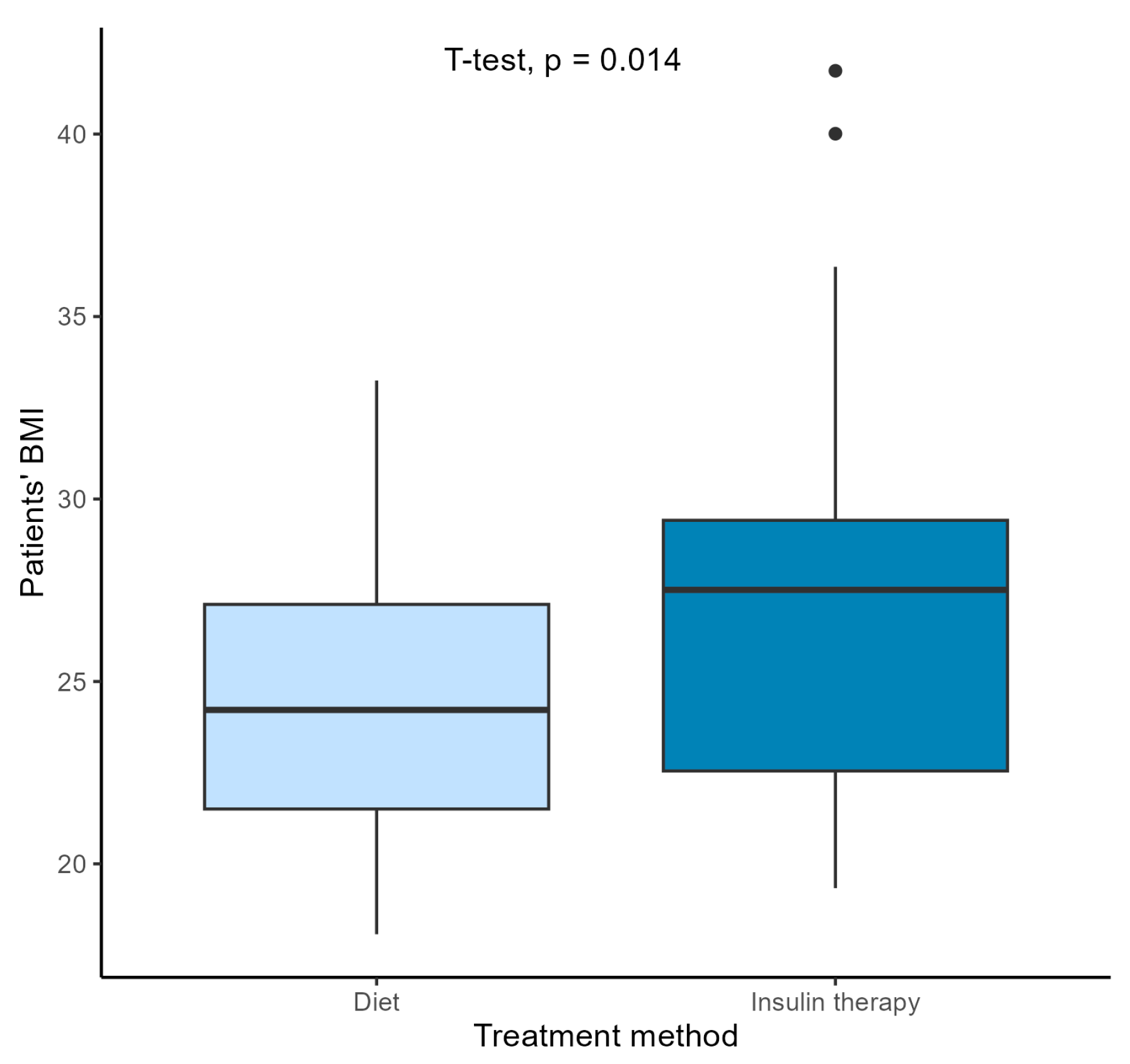 diet treated patients; insulin treated patients.
diet treated patients; insulin treated patients.
diet treated patients; insulin treated patients.
diet treated patients; insulin treated patients.

{kind=link}
{kind=link}
{kind=link}
| Variable | GDM in the 2018/2019 Group (n = 65) | GDM in the COVID-19 Group (n = 66) | p | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| Age, years | 30.9 | 4.56 | 32 | 4.6 | 0.187 | ||
| Body weight before pregnancy, kg | 73.2 | 21.4 | 68.9 | 13.4 | 0.294 | ||
| BMI, kg/m2 | 26.3 | 6.4 | 25.3 | 4 | 0.47 | ||
| Body weight gain during pregnancy, kg | 9.24 | 8.06 | 9.59 | 5.83 | 0.776 | ||
| Week in which GDM was diagnosed | 24 | 7 | 18 | 9 | <0.001 | ||
| Week of delivery | 38.1 | 2.12 | 38.4 | 1.61 | 0.43 | ||
| Neonatal body weight at delivery, g | 3220.0 | 531 | 3180.0 | 503 | 0.635 | ||
| Neonatal body length at delivery, cm | 53.7 | 3.18 | 53.7 | 3.06 | 0.937 | ||
| Median | Q1 | Q3 | Median | Q1 | Q3 | p | |
| Week in which insulin was started | 26.5 | 19.5 | 30.2 | 28 | 14 | 32 | 0.690 |
| Order of pregnancy in which GDM occurred | 1 | 1 | 2 | 2 | 1 | 3 | 0.00617 |
| Apgar score at 1 min | 10.00 | 9.00 | 10.00 | 10.00 | 10.000 | 10.00 | 0.0855 |
| Variable | 18/19 Group, n = 65 | COVID-19 Group, n = 66 | p |
|---|---|---|---|
| BMI before pregnancy | 0.032 | ||
| <25 | 59% | 45% | |
| ≥25 | 15% | 43% | |
| ≥30 | 26% | 12% | |
| Order of pregnancy in which | 0.060 | ||
| GDM occurred | |||
| 1 | 58% | 38% | |
| 2 | 24% | 31% | |
| 3 | 8% | 25% | |
| 4 | 8% | 2% | |
| 5 | 2% | 2% | |
| 6 | 0% | 2% | |
| Diagnosis of GDM (OGTT) | 0.33 | ||
| Fasting | 22 (34%) | 25 (38%) | |
| 2 PG | 19 (29%) | 11 (17%) | |
| 1h PG, 2h PG | 7 (11%) | 8 (12%) | |
| 1h PG | 7 (11%) | 6 (9%) | |
| Fasting, 1h PG, 2h PG | 3 (5%) | 10 (15%) | |
| Fasting, 1h PG | 4 (6%) | 2 (3%) | |
| Fasting, 2h PG | 3 (5%) | 3 (5%) | |
| Mother over the age of 35 | 55 (85%) | 48 (73%) | 0.15 |
| Caesarean sections/spontaneous delivery | 52%/48% | 57%/43% | 0.72 |
| Neonatal body mass at delivery: | >0.99 | ||
| <4000 g | 94% | 94% | |
| >4000 g | 6% | 6% |
| Variable | n | Median | Q1 | Q3 | p | |
|---|---|---|---|---|---|---|
| GDM in the 2018/2019 group | diet | 42 | 10 | 7 | 15 | |
| insulin | 23 | 7.5 | 2.25 | 11.8 | p = 0.039 | |
| GDM in the COVID-19 group | diet | 35 | 11.5 | 8 | 13 | |
| insulin | 31 | 9 | 6 | 12 | p = 0.059 |
| Maternal Comorbidities | 2018/2019 GDM Group (n = 65) | COVID-19 GDM Group (n = 66) | Chi2 Test | ||
|---|---|---|---|---|---|
| Arterial hypertension | 6 | 4.58% | 7 | 5.344% | p = 1 |
| Hypothyroidism | 18 | 13.74% | 28 | 21.374% | p = 0.1134 |
| Polycystic ovary syndrome | 10 | 7.64% | 6 | 4.58% | p = 0.4048 |
| Neonatal Comorbidities | 18/19 GDM Group (n = 65) | COVID-19 GDM Group (n = 66) | Chi2 Test | ||
|---|---|---|---|---|---|
| Hypoglycemia | 3 | 2.29% | 1 | 0.763% | p = 0.6007 |
| Prolonged jaundice | 10 | 7.63% | 6 | 4.58% | p = 0.4048 |
| Heart defects | 2 | 1.527% | 0 | 0% | p = 0.4694 |
| COVID-19 GDM Group (n = 66) | ||
|---|---|---|
| Type of first visit | In-person | 63 (95.5%) |
| Teleconsultation | 3 (4.5%) | |
| What kind of visit do you prefer? | In-person | 9 (13.6%) |
| Teleconsultation | 40 (60.6%) | |
| Both | 7 (10.6%) | |
| I do not know | 10 (15.2%) | |
| Past COVID-19 infection? | No | 33 (50%) |
| Yes | 33 (50%) | |
| COVID-19 vaccination? | No | 27 (41%) |
| Yes | 39 (59%) | |
| Did the pandemic negatively affect your pregnancy? | No | 36 (54.5%) |
| Yes | 30 (45.5%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cichocka, E.; Gumprecht, J. The Impact of Telemedicine during the COVID-19 Pandemic on Diabetes Management and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus (GDM). J. Clin. Med. 2024, 13, 5797. https://doi.org/10.3390/jcm13195797
Cichocka E, Gumprecht J. The Impact of Telemedicine during the COVID-19 Pandemic on Diabetes Management and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus (GDM). Journal of Clinical Medicine. 2024; 13(19):5797. https://doi.org/10.3390/jcm13195797
Chicago/Turabian StyleCichocka, Edyta, and Janusz Gumprecht. 2024. "The Impact of Telemedicine during the COVID-19 Pandemic on Diabetes Management and Pregnancy Outcomes in Women with Gestational Diabetes Mellitus (GDM)" Journal of Clinical Medicine 13, no. 19: 5797. https://doi.org/10.3390/jcm13195797