
Sensitization to Staphylococcus Enterotoxin: Relationship with Aspects of Disease Severity

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Lung Function
2.3. Atopic Status
2.4. Enterotoxin Measurement
2.5. Asthma Control Test (ACT)
2.6. Sputum Induction
2.7. Bronchoscopy and Airway Remodeling Assessment
2.8. Study Design
3. Statistical Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACT | asthma control test |
| AERD | aspirin-exacerbated respiratory disease |
| APC | antigen-presenting cell |
| ATS | American Thoracic Society |
| BAL | bronchoalveolar lavage |
| BMI | body mass index |
| BMT | basement membrane thickness |
| CS | corticosteroid |
| DTT | dithiothreitol |
| ERS | European Respiratory Society |
| FEV1 | forced expiratory volume in 1 s |
| FVC | Forced Vital Capacity |
| ICS | inhaled corticosteroid |
| H&E | Hematoxylin & Eosin |
| IgE | Immunoglobulin E |
| IL-5 | interleukin-5 |
| IL-4 | interleukin-4 |
| IL-13 | interleukin-13 |
| IL-33 | interleukin-33 |
| IL-25 | interleukin-25 |
| IS | induced sputum |
| LABA | long-acting β2 agonists |
| LAMA | long-acting muscarinic antagonists |
| LTRA | leukotriene receptor antagonists |
| PAS | Periodic Acid Schiff |
| PB | post-bronchodilation |
| RBM | reticularbasement membrane |
| RCF | Relative Centrifugal Force |
| SD | standard deviation |
| SEs | Staphylococcus aureus enterotoxins |
| SMA | smooth muscle area |
| SRA | Severe Refractory Asthma |
| TCRVβ | TCR molecule |
| TSLP | thymic stromal lymphopoietin |
| TSST-1 | toxic shock syndrome toxin-1 |
| WSI | whole slide image |
References
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- Couillard, S.; Jackson, D.J.; Wechsler, M.E.; Pavord, I.D. Workup of Severe Asthma. Chest 2021, 160, 2019–2029. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, A.; Assadinia, N.; Hackett, T.L. Airway remodeling heterogeneity in asthma and its relationship to disease outcomes. Front. Physiol. 2023, 14, 1113100. [Google Scholar] [CrossRef]
- Ferreira, D.S.; Carvalho-Pinto, R.M.; Gregorio, M.G.; Annoni, R.; Teles, A.M.; Buttignol, M.; Araujo-Paulino, B.B.; Katayama, E.H.; Oliveira, B.L.; Del Frari, H.S.; et al. Airway pathology in severe asthma is related to airflow obstruction but not symptom control. Allergy 2018, 73, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Derycke, L.; Perez-Novo, C.; Van Crombruggen, K.; Corriveau, M.N.; Bachert, C. Staphylococcus aureus and Chronic Airway Disease. World Allergy Organ. J. 2010, 3, 223–228. [Google Scholar] [CrossRef]
- Flora, M.; Perrotta, F.; Nicolai, A.; Maffucci, R.; Pratillo, A.; Mollica, M.; Bianco, A.; Calabrese, C. Staphylococcus aureus in chronic airway diseases: An overview. Respir. Med. 2019, 155, 66–71. [Google Scholar] [CrossRef]
- Bachert, C.; van Steen, K.; Zhang, N.; Holtappels, G.; Cattaert, T.; Maus, B.; Buhl, R.; Taube, C.; Korn, S.; Kowalski, M.; et al. Specific IgE against Staphylococcus aureus enterotoxins: An independent risk factor for asthma. J. Allergy Clin. Immunol. 2012, 130, 376–381.e8. [Google Scholar] [CrossRef]
- Bachert, C.; Humbert, M.; Hanania, N.A.; Zhang, N.; Holgate, S.; Buhl, R.; Broker, B.M. Staphylococcus aureus and its IgE-inducing enterotoxins in asthma: Current knowledge. Eur. Respir. J. 2020, 55, 1901592. [Google Scholar] [CrossRef]
- Song, W.J.; Sintobin, I.; Sohn, K.H.; Kang, M.G.; Park, H.K.; Jo, E.J.; Lee, S.E.; Yang, M.S.; Kim, S.H.; Park, H.K.; et al. Staphylococcal enterotoxin IgE sensitization in late-onset severe eosinophilic asthma in the elderly. Clin. Exp. Allergy 2016, 46, 411–421. [Google Scholar] [CrossRef]
- Tanaka, A.; Suzuki, S.; Ohta, S.; Manabe, R.; Furukawa, H.; Kuwahara, N.; Fukuda, Y.; Kimura, T.; Jinno, M.; Hirai, K.; et al. Association between specific IgE to Staphylococcus aureus enterotoxins A and B and asthma control. Ann. Allergy Asthma Immunol. 2015, 115, 191–197.e2. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Kips, J.C.; Fahy, J.V.; Hargreave, F.E.; Ind, P.W.; In’t Veen, J.C. Methods for sputum induction and analysis of induced sputum: A method for assessing airway inflammation in asthma. Eur. Respir. J. Suppl. 1998, 26, 9S–12S. [Google Scholar] [PubMed]
- Grootendorst, D.C.; van den Bos, J.W.; Romeijn, J.J.; Veselic-Charvat, M.; Duiverman, E.J.; Vrijlandt, E.J.; Sterk, P.J.; Roldaan, A.C. Induced sputum in adolescents with severe stable asthma. Safety and the relationship of cell counts and eosinophil cationic protein to clinical severity. Eur. Respir. J. 1999, 13, 647–653. [Google Scholar] [CrossRef]
- Efthimiadis, A.; Spanevello, A.; Hamid, Q.; Kelly, M.M.; Linden, M.; Louis, R.; Pizzichini, M.M.; Pizzichini, E.; Ronchi, C.; Van Overvel, F.; et al. Methods of sputum processing for cell counts, immunocytochemistry and in situ hybridisation. Eur. Respir. J. Suppl. 2002, 37, 19s–23s. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, P.; Holgate, S.; Wenzel, S.; Endobronchial Biopsy, W. Methods for the assessment of endobronchial biopsies in clinical research: Application to studies of pathogenesis and the effects of treatment. Am. J. Respir. Crit. Care Med. 2003, 168, S1–S17. [Google Scholar] [CrossRef] [PubMed]
- Haslam, P.L.; Baughman, R.P. Report of ERS Task Force: Guidelines for measurement of acellular components and standardization of BAL. Eur. Respir. J. 1999, 14, 245–248. [Google Scholar] [CrossRef]
- Benayoun, L.; Druilhe, A.; Dombret, M.C.; Aubier, M.; Pretolani, M. Airway structural alterations selectively associated with severe asthma. Am. J. Respir. Crit. Care Med. 2003, 167, 1360–1368. [Google Scholar] [CrossRef]
- Sullivan, P.; Stephens, D.; Ansari, T.; Costello, J.; Jeffery, P. Variation in the measurements of basement membrane thickness and inflammatory cell number in bronchial biopsies. Eur. Respir. J. 1998, 12, 811–815. [Google Scholar] [CrossRef]
- Papaporfyriou, A.; Bakakos, P.; Kostikas, K.; Papatheodorou, G.; Hillas, G.; Trigidou, R.; Katafigiotis, P.; Koulouris, N.G.; Papiris, S.A.; Loukides, S. Activin A and follistatin in patients with asthma. Does severity make the difference? Respirology 2017, 22, 473–479. [Google Scholar] [CrossRef]
- Sintobin, I.; Siroux, V.; Holtappels, G.; Pison, C.; Nadif, R.; Bousquet, J.; Bachert, C. Sensitisation to staphylococcal enterotoxins and asthma severity: A longitudinal study in the EGEA cohort. Eur. Respir. J. 2019, 54, 1900198. [Google Scholar] [CrossRef]
- Caruso, C.; Colantuono, S.; Ciasca, G.; Basile, U.; Di Santo, R.; Bagnasco, D.; Passalacqua, G.; Caminati, M.; Michele, S.; Senna, G.; et al. Different aspects of severe asthma in real life: Role of Staphylococcus aureus enterotoxins and correlation to comorbidities and disease severity. Allergy 2023, 78, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Schleich, F.; Moermans, C.; Gerday, S.; Ziant, S.; Louis, G.; Bougard, N.; Paulus, V.; Guissard, F.; Henket, M.; Bachert, C.; et al. Patients With Asthma Only Sensitized to Staphylococcus aureus Enterotoxins Have More Exacerbations, Airflow Limitation, and Higher Levels of Sputum IL-5 and IgE. J. Allergy Clin. Immunol. Pract. 2023, 11, 3055–3061.e4. [Google Scholar] [CrossRef]
- Nagasaki, T.; Matsumoto, H.; Oguma, T.; Ito, I.; Inoue, H.; Iwata, T.; Tajiri, T.; Kanemitsu, Y.; Izuhara, Y.; Morimoto, C.; et al. Sensitization to Staphylococcus aureus enterotoxins in smokers with asthma. Ann. Allergy Asthma Immunol. 2017, 119, 408–414.e2. [Google Scholar] [CrossRef] [PubMed]
- de Wit, J.; Totte, J.E.E.; van Buchem, F.J.M.; Pasmans, S. The prevalence of antibody responses against Staphylococcus aureus antigens in patients with atopic dermatitis: A systematic review and meta-analysis. Br. J. Dermatol. 2018, 178, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Semic-Jusufagic, A.; Bachert, C.; Gevaert, P.; Holtappels, G.; Lowe, L.; Woodcock, A.; Simpson, A.; Custovic, A. Staphylococcus aureus sensitization and allergic disease in early childhood: Population-based birth cohort study. J. Allergy Clin. Immunol. 2007, 119, 930–936. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, M.L.; Cieslak, M.; Perez-Novo, C.A.; Makowska, J.S.; Bachert, C. Clinical and immunological determinants of severe/refractory asthma (SRA): Association with Staphylococcal superantigen-specific IgE antibodies. Allergy 2011, 66, 32–38. [Google Scholar] [CrossRef]
- Won, H.K.; Song, W.J.; Moon, S.D.; Sohn, K.H.; Kim, J.Y.; Kim, B.K.; Park, H.W.; Bachert, C.; Cho, S.H. Staphylococcal Enterotoxin-Specific IgE Sensitization: A Potential Predictor of Fixed Airflow Obstruction in Elderly Asthma. Allergy Asthma Immunol. Res. 2023, 15, 160–173. [Google Scholar] [CrossRef]
- Zhang, N.; Holtappels, G.; Gevaert, P.; Patou, J.; Dhaliwal, B.; Gould, H.; Bachert, C. Mucosal tissue polyclonal IgE is functional in response to allergen and SEB. Allergy 2011, 66, 141–148. [Google Scholar] [CrossRef]
- Bachert, C.; Holtappels, G.; Merabishvili, M.; Meyer, T.; Murr, A.; Zhang, N.; Van Crombruggen, K.; Gevaert, E.; Volker, U.; Broker, B.M.; et al. Staphylococcus aureus controls interleukin-5 release in upper airway inflammation. J. Proteom. 2018, 180, 53–60. [Google Scholar] [CrossRef]
- Persson, E.K.; Verstraete, K.; Heyndrickx, I.; Gevaert, E.; Aegerter, H.; Percier, J.M.; Deswarte, K.; Verschueren, K.H.G.; Dansercoer, A.; Gras, D.; et al. Protein crystallization promotes type 2 immunity and is reversible by antibody treatment. Science 2019, 364, eaaw4295. [Google Scholar] [CrossRef] [PubMed]
- Lan, F.; Zhang, N.; Holtappels, G.; De Ruyck, N.; Krysko, O.; Van Crombruggen, K.; Braun, H.; Johnston, S.L.; Papadopoulos, N.G.; Zhang, L.; et al. Staphylococcus aureus Induces a Mucosal Type 2 Immune Response via Epithelial Cell-derived Cytokines. Am. J. Respir. Crit. Care Med. 2018, 198, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Tomassen, P.; Jarvis, D.; Newson, R.; Van Ree, R.; Forsberg, B.; Howarth, P.; Janson, C.; Kowalski, M.L.; Kramer, U.; Matricardi, P.M.; et al. Staphylococcus aureus enterotoxin-specific IgE is associated with asthma in the general population: A GA2LEN study. Allergy 2013, 68, 1289–1297. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | SRA (n = 50) | Specific IgE SE (+) n = 12 | Specific IgE SE (−) n = 38 |
|---|---|---|---|
| Age | 53 ± 12 | 51 ± 13 | 54 ± 11 |
| Gender (female/male) | 33/17 | 9/3 | 25/13 |
| Atopy (n &%) | 29/50–58% | 8/12–66% | 21/38–55% |
| Nasal Polyps (n &%) | 17/50–34% | 4/12–30% | 13/38–34% |
| Atopic dermatitis (n &%) | 5/50–10% | 2/12–16% | 3/38–8% |
| Eczema (n &%) | 4/50–8% | 1/12–8% | 3/38–8% |
| Allergic Rhinitis (n &%) | 24/50–48% | 5/12–41% | 19/38–50% |
| Duration of asthma (years) | 17.4 ± 15.4 | 18.6 ± 15.5 | 16 ± 15 |
| Smoking (current/ex/never) | 3/13/34 | 1/4/8 | 2//9/17 |
| BMI Kg/m2 | 24.7 (23, 27) | 24.7 ± 3.9 | 25 (23, 27) |
| ACT | 21 (19, 24) | 20 (18, 23) | 21 (19, 23) |
| PB FEV1% pred. | 75 ± 21 | 55 (49, 65) | 81 ± 20 * |
| PB FEV1/FVC% | 73 ± 8 | 65 ± 12 | 77 ± 18 * |
| Treatment regimens | |||
| ICS | 50 ^ | 12 ^ | 35 |
| LABA | 48 | 11 | 37 |
| CS per os | 14^^ | 4 ^^^ | 10 |
| LAMA | 18 | 5 | 13 |
| LTRA | 16 | 5 | 11 |
| Omalizumab | 5 | 2 | 3 |
| Mepolizumab | 16 | 7 | 9 |
| Benrlazumab | 6 | 4 | 2 |
| Variables | Specific IgE SE (+) n = 12 | Specific IgE SE (−) n = 38 | p-Value |
|---|---|---|---|
| Cells × 106/mL BAL | 3.2(2.1–4.7) | 3.8 (2.4, 5.1) | 0.37 |
| Eosinophils (%) BAL | 1.1 (0, 8) | 1.3 (0, 5) | 0.62 |
| Neutrophils (%) BAL | 2.4 (0.6, 6.9) | 2 (1, 4) | 0.81 |
| Cells × 106/mL IS | 18 (14–21) | 19 (15–21) | 0.621 |
| Eosinophils (%) IS | 1 (0, 4) | 1 (0–3.5) | 0.77 |
| Neutrophils (%) IS | 25 (8, 52) | 21 (11, 30) | 0.55 |
| Eosinophils (%) blood | 4.4 (1.7, 8.5) | 3.6 (2.5, 6.5) | 0.38 |
| Eosinophils AC blood | 252 (155, 668) | 204 (121, 560) | 0.45 |
| IgEiu/mL | 176 (124, 288) | 160 (114, 275) | 0.66 |
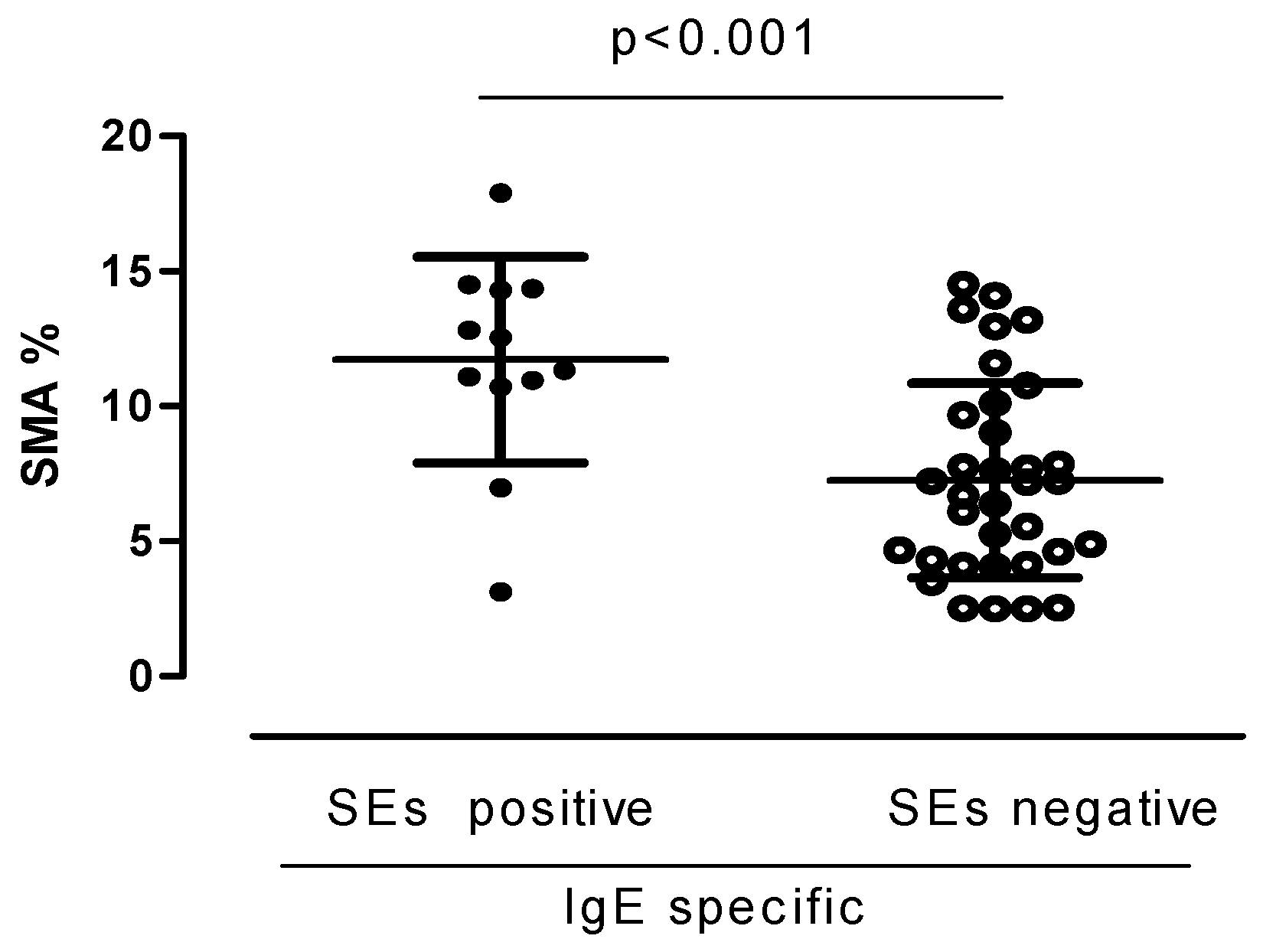
| SMA % | 11.7 ± 3.8 | 7.2 ± 3.6 | <0.01 |
| BMT μm | 9 ± 1.6 | 9.4 ± 1.22 | 0.67 |
| Integrity of the epithelium % | 40 ± 22 | 35 ± 25 | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schoini, P.; Apollonatou, V.; Kallieri, M.; Blizou, M.; Sfika, M.; Koufopoulos, N.; Pouliakis, A.; Liatsis, E.; Foukas, P.; Bakakos, P.; et al. Sensitization to Staphylococcus Enterotoxin: Relationship with Aspects of Disease Severity. J. Clin. Med. 2024, 13, 5836. https://doi.org/10.3390/jcm13195836
Schoini P, Apollonatou V, Kallieri M, Blizou M, Sfika M, Koufopoulos N, Pouliakis A, Liatsis E, Foukas P, Bakakos P, et al. Sensitization to Staphylococcus Enterotoxin: Relationship with Aspects of Disease Severity. Journal of Clinical Medicine. 2024; 13(19):5836. https://doi.org/10.3390/jcm13195836
Chicago/Turabian StyleSchoini, Pinelopi, Vasiliki Apollonatou, Maria Kallieri, Myrto Blizou, Maria Sfika, Nektarios Koufopoulos, Abraham Pouliakis, Emmanouil Liatsis, Periklis Foukas, Petros Bakakos, and et al. 2024. "Sensitization to Staphylococcus Enterotoxin: Relationship with Aspects of Disease Severity" Journal of Clinical Medicine 13, no. 19: 5836. https://doi.org/10.3390/jcm13195836
APA StyleSchoini, P., Apollonatou, V., Kallieri, M., Blizou, M., Sfika, M., Koufopoulos, N., Pouliakis, A., Liatsis, E., Foukas, P., Bakakos, P., & Loukides, S. (2024). Sensitization to Staphylococcus Enterotoxin: Relationship with Aspects of Disease Severity. Journal of Clinical Medicine, 13(19), 5836. https://doi.org/10.3390/jcm13195836