
Aortic and Mitral Valve Endocarditis—Simply Left-Sided Endocarditis or Different Entities Requiring Individual Consideration?—Insights from the CAMPAIGN Database
 , , ,
, , ,  , , , , , ,
, , , , , ,  on behalf of the Study Group “Clinical, Multicenter Project of Analysis of Infective Endocarditis in Germany” (CAMPAIGN)
on behalf of the Study Group “Clinical, Multicenter Project of Analysis of Infective Endocarditis in Germany” (CAMPAIGN)
Abstract
1. Introduction
- Surgical treatment of MV-IE is associated with a higher mortality rate than that of AV-IE.
- MV-IE itself is an independent risk factor for mortality.
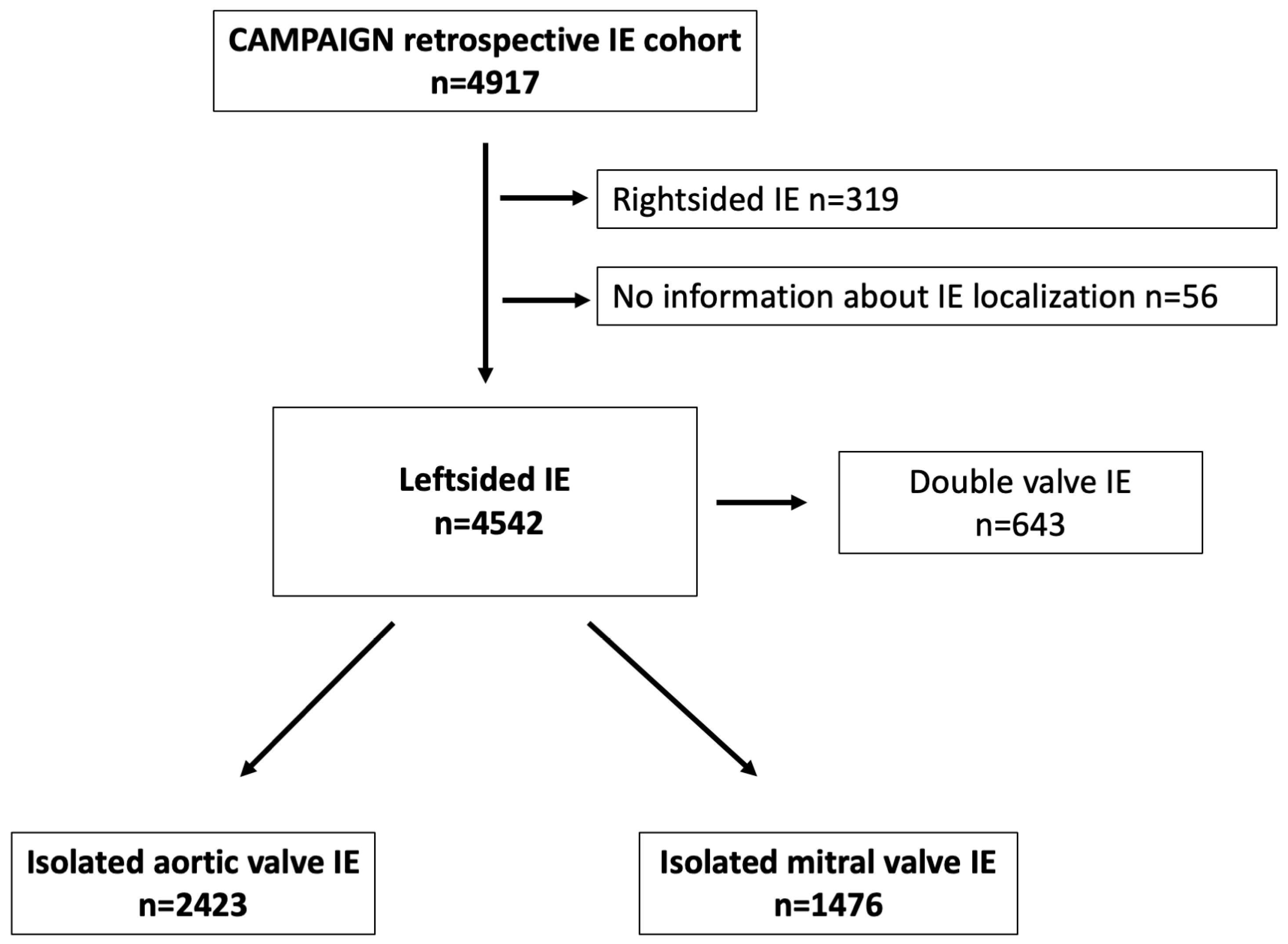
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
2.3. Ethical Statement
3. Results
3.1. Characteristics of Patients with MV-IE versus AV-IE
3.2. Postoperative Outcomes after Surgery for MV-IE versus AV-IE
3.3. Independent Predictors of Mortality for Patients with Left-Sided IE
4. Discussion
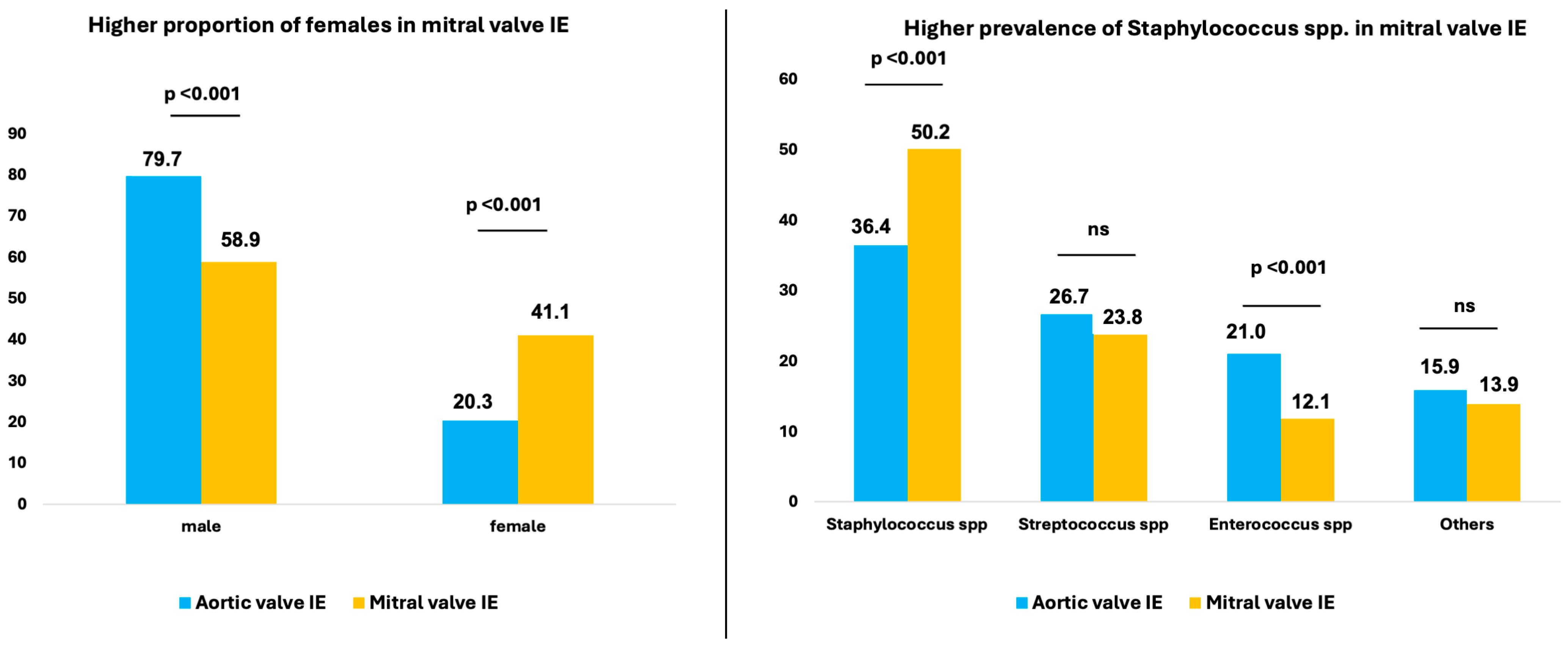
4.1. Gender Distribution in MV-IE versus AV-IE
4.2. Risk of Cerebral Embolism in MV-IE Compared with AV-IE
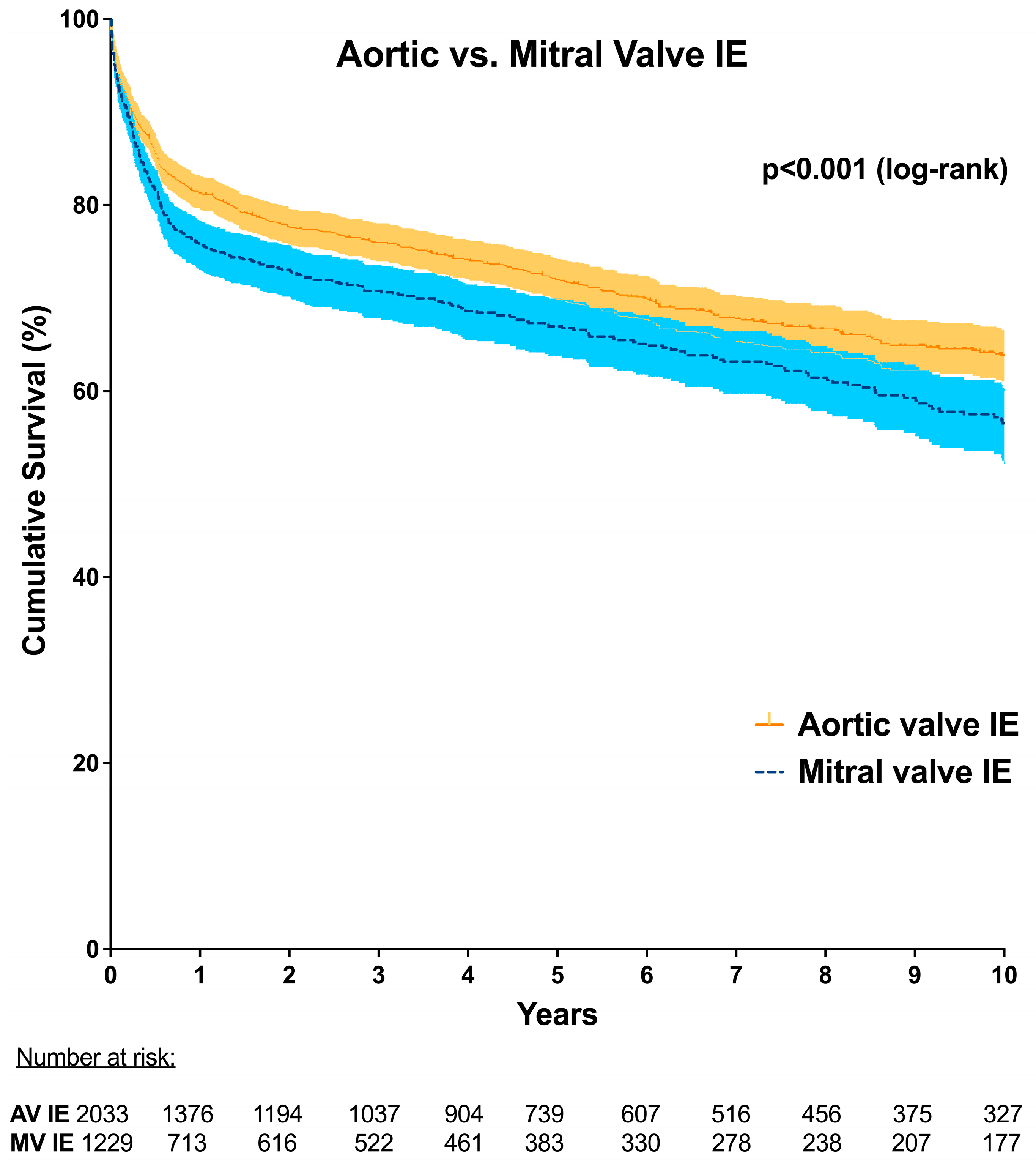
4.3. Mortality in MV-IE versus AV-IE
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Vlasselaer, A.; Rasmussen, M.; Nilsson, J.; Olaison, L.; Ragnarsson, S. Native aortic versus mitral valve infective endocarditis: A nationwide registry study. Open Heart 2019, 6, e000926. [Google Scholar] [CrossRef]
- David, T.E.; Armstrong, S.; McCrindle, B.W.; Manlhiot, C. Late outcomes of mitral valve repair for mitral regurgitation due to degenerative disease. Circulation 2013, 127, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- Barnes, A.M.T.; Frank, K.L.; Dale, J.L.; Manias, D.A.; Powers, J.L.; Dunny, G.M. Enterococcus faecalis colonizes and forms persistent biofilm microcolonies on undamaged endothelial surfaces in a rabbit endovascular infection model. FEMS Microbes 2021, 2, xtab014. [Google Scholar] [CrossRef]
- Kaushik, A.; Kest, H.; Sood, M.; Steussy, B.W.; Thieman, C.; Gupta, S. Biofilm Producing Methicillin-Resistant Staphylococcus aureus (MRSA) Infections in Humans: Clinical Implications and Management. Pathogens 2024, 13, 76. [Google Scholar] [CrossRef] [PubMed]
- Kinney, K.J.; Stach, J.M.; Kulhankova, K.; Brown, M.; Salgado-Pabón, W. Vegetation Formation in Staphylococcus aureus Endocarditis Inversely Correlates with RNAIII and sarA Expression in Invasive Clonal Complex 5 Isolates. Front. Cell. Infect. Microbiol. 2022, 12, 925914. [Google Scholar] [CrossRef]
- Nappi, F. Current Knowledge of Enterococcal Endocarditis: A Disease Lurking in Plain Sight of Health Providers. Pathogens 2024, 13, 235. [Google Scholar] [CrossRef]
- Álvarez-Zaballos, S.; Vázquez-Alen, P.; Muñoz, P.; de Alarcón, A.; Gutiérrez Carretero, E.; Álvarez-Uría, A.; Fariñas, M.C.; Rodríguez-García, R.; Goenaga, M.; Cuervo, G.; et al. Prevalence and prognostic impact of stroke in a national cohort of infective endocarditis. Int. J. Stroke 2024. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Gassa, A.; Rokohl, A.; Sabashnikov, A.; Deppe, A.C.; Eghbalzadeh, K.; Merkle, J.; Hamacher, S.; Liakopoulos, O.J.; Wahlers, T. Severity of presentation, not sex, increases risk of surgery for infective endocarditis. Ann. Thorac. Surg. 2018, 107, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, P.; Marin-Cuartas, M.; Weber, C.; De La Cuesta, M.; Lichtenberg, A.; Petrov, A.; Hagl, C.; Aubin, H.; Matschke, K.; Diab, M.; et al. Sex-related differences in patients with infective endocarditis requiring cardiac surgery: Insights from the CAMPAIGN Study Group. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2024, 66, ezae292. [Google Scholar] [CrossRef] [PubMed]
- De Miguel-Yanes, J.M.; Jimenez-Garcia, R.; De Miguel-Diez, J.; Hernández-Barrera, V.; Carabantes-Alarcon, D.; Zamorano-Leon, J.J.; Noriega, C.; Lopez-de-Andres, A. Differences in Sex and the Incidence and In-Hospital Mortality among People Admitted for Infective Endocarditis in Spain, 2016–2020. J. Clin. Med. 2022, 11, 6847. [Google Scholar] [CrossRef] [PubMed]
- Leterrier, J.; Iung, B.; de Tymoski, C.; Deconinck, L.; Para, M.; Duval, X.; Provenchere, S.; Mesnier, J.; Delhomme, C.; Haviari, S.; et al. Sex differences and outcomes in surgical infective endocarditis. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2024, 65, ezae114. [Google Scholar] [CrossRef] [PubMed]
- Song, H.K.; Grab, J.D.; O’Brien, S.M.; Welke, K.F.; Edwards, F.; Ungerleider, R.M. Gender differences in mortality after mitral valve operation: Evidence for higher mortality in perimenopausal women. Ann. Thorac. Surg. 2008, 85, 2040–2044. [Google Scholar] [CrossRef]
- Mokhles, M.M.; Siregar, S.; Versteegh, M.I.; Noyez, L.; van Putte, B.; Vonk, A.B.; Roos-Hesselink, J.W.; Bogers, A.J.; Takkenberg, J.J. Male-female differences and survival in patients undergoing isolated mitral valve surgery: A nationwide cohort study in the Netherlands. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2016, 50, 482–487. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miro, J.M.; Fowler, V.G., Jr.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Sambola, A.; Lozano-Torres, J.; Boersma, E.; Olmos, C.; Ternacle, J.; Calvo, F.; Tribouilloy, C.; Reskovic-Luksic, V.; Separovic-Hanzevacki, J.; Park, S.W.; et al. Predictors of embolism and death in left-sided infective endocarditis: The European Society of Cardiology EURObservational Research Programme European Infective Endocarditis registry. Eur. Heart J. 2023, 44, 4566–4575. [Google Scholar] [CrossRef] [PubMed]
- Selton-Suty, C.; Delahaye, F.; Tattevin, P.; Federspiel, C.; Le Moing, V.; Chirouze, C.; Nazeyrollas, P.; Vernet-Garnier, V.; Bernard, Y.; Chocron, S.; et al. Symptomatic and Asymptomatic Neurological Complications of Infective Endocarditis: Impact on Surgical Management and Prognosis. PLoS ONE 2016, 11, e0158522. [Google Scholar] [CrossRef] [PubMed]
- Trifunovic, D.; Vujisic-Tesic, B.; Obrenovic-Kircanski, B.; Ivanovic, B.; Kalimanovska-Ostric, D.; Petrovic, M.; Boricic-Kostic, M.; Matic, S.; Stevanovic, G.; Marinkovic, J.; et al. The relationship between causative microorganisms and cardiac lesions caused by infective endocarditis: New perspectives from the contemporary cohort of patients. J. Cardiol. 2018, 71, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef] [PubMed]
- Dickerman, S.A.; Abrutyn, E.; Barsic, B.; Bouza, E.; Cecchi, E.; Moreno, A.; Doco-Lecompte, T.; Eisen, D.P.; Fortes, C.Q.; Fowler, V.G., Jr.; et al. The relationship between the initiation of antimicrobial therapy and the incidence of stroke in infective endocarditis: An analysis from the ICE Prospective Cohort Study (ICE-PCS). Am. Heart J. 2007, 154, 1086–1094. [Google Scholar] [CrossRef]
- Ruttmann, E.; Abfalterer, H.; Wagner, J.; Grimm, M.; Müller, L.; Bates, K.; Ulmer, H.; Bonaros, N. Endocarditis-related stroke is not a contraindication for early cardiac surgery: An investigation among 440 patients with left-sided endocarditis. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2020, 58, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, I.; Hunter, M.D.; Sundheim, K.; Klein, B.; Dunn, L.; Sorabella, R.; Han, S.M.; Willey, J.; George, I.; Gutierrez, J. Clinical Risk Factors for Acute Ischemic and Hemorrhagic Stroke in Patients with Infective Endocarditis. Intern. Med. J. 2018, 48, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Diab, M.; Franz, M.; Hagel, S.; Guenther, A.; Struve, A.; Musleh, R.; Penzel, A.; Sponholz, C.; Lehmann, T.; Kuehn, H.; et al. Impact of an In-Hospital Endocarditis Team and a State-Wide Endocarditis Network on Perioperative Outcomes. J. Clin. Med. 2021, 10, 4734. [Google Scholar] [CrossRef] [PubMed]
- Paul, G.; Ochs, L.; Hohmann, C.; Baldus, S.; Michels, G.; Meyer-Schwickerath, C.; Fatkenheuer, G.; Mader, N.; Wahlers, T.; Weber, C.; et al. Surgical Procedure Time and Mortality in Patients with Infective Endocarditis Caused by Staphylococcus aureus or Streptococcus Species. J. Clin. Med. 2022, 11, 2538. [Google Scholar] [CrossRef]
- Lauten, A.; Martinović, M.; Kursawe, L.; Kikhney, J.; Affeld, K.; Kertzscher, U.; Falk, V.; Moter, A. Bacterial biofilms in infective endocarditis: An in vitro model to investigate emerging technologies of antimicrobial cardiovascular device coatings. Clin. Res. Cardiol. Off. J. Ger. Card. Soc. 2021, 110, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Galar, A.; Weil, A.A.; Dudzinski, D.M.; Munoz, P.; Siedner, M.J. Methicillin-Resistant Staphylococcus aureus Prosthetic Valve Endocarditis: Pathophysiology, Epidemiology, Clinical Presentation, Diagnosis, and Management. Clin. Microbiol. Rev. 2019, 32, e00041-18. [Google Scholar] [CrossRef] [PubMed]
- Hoerr, V.; Franz, M.; Pletz, M.W.; Diab, M.; Niemann, S.; Faber, C.; Doenst, T.; Schulze, P.C.; Deinhardt-Emmer, S.; Loffler, B. S. aureus endocarditis: Clinical aspects and experimental approaches. Int. J. Med. Microbiol. 2018, 308, 640–652. [Google Scholar] [CrossRef] [PubMed]
- Ostergaard, L.; Bruun, N.E.; Voldstedlund, M.; Arpi, M.; Andersen, C.O.; Schonheyder, H.C.; Lemming, L.; Rosenvinge, F.; Valeur, N.; Sogaard, P.; et al. Prevalence of infective endocarditis in patients with positive blood cultures: A Danish nationwide study. Eur. Heart J. 2019, 40, 3237–3244. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.T.; Shrestha, N.K.; Gordon, S.M.; Houghtaling, P.L.; Blackstone, E.H.; Pettersson, G.B. Residual patient, anatomic, and surgical obstacles in treating active left-sided infective endocarditis. J. Thorac. Cardiovasc. Surg. 2014, 148, 981–988. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Aortic Valve IE (n = 2423) | Mitral Valve IE (n = 1476) | p Value | |
|---|---|---|---|
| Age (years) | 65.0 [53.0–73.0] | 66.0 [56.0–74.0] | 0.013 # |
| Sex (%) | |||
| male | 79.7% (1930/2423) | 58.9% (869/1476) | <0.001 † |
| female | 20.3% (493/2423) | 41.1% (607/1476) | <0.001 † |
| BMI (kg/m2) | 26.0 [23.7–29.3] | 25.5 [23.2–29.1] | 0.004 # |
| Underlying conditions/comorbidities | |||
| Hypertension | 50.5% (1223/2423) | 49.2% (726/1476) | 0.435 † |
| Diabetes | 24.5% (593/2423) | 29.1% (430/1476) | 0.001 † |
| Hyperlipidemia | 21.2% (489/2308) | 18.9% (270/1427) | 0.094 † |
| Smoking | 19.4% (459/2364) | 13.9% (201/1448) | <0.001 † |
| COPD | 10.3% (247/2404) | 10.0% (144/1438) | 0.796 † |
| Peripheral artery disease | 7.8% (189/2423) | 7.5% (111/1476) | 0.750 † |
| Pulmonary hypertension | 14.5% (351/2423) | 21.3% (314/1476) | <0.001 † |
| Preoperative CKD | 37.4% (906/2423) | 38.5% (568/1476) | 0.496 † |
| Preoperative hemodialysis | 7.0% (169/2423) | 8.6% (127/1476) | 0.062 † |
| Preoperative stroke | 19.3% (464/2402) | 28.2% (412/1463) | <0.001 † |
| Coronary artery disease | 27.4% (605/2208) | 29.8% (400/1342) | 0.123 † |
| Myocardial infarction | 7.4% (178/2398) | 6.8% (98/1442) | 0.467 † |
| Septic cerebral embolism | 17.7% (430/2423) | 25.4% (375/1476) | <0.001 † |
| LVEF | |||
| ≥50% | 70.3% (1639/2332) | 78.6% (1122/1428) | <0.001 † |
| ≥30% to 50% | 25.7% (599/2332) | 18.7% (267/1428) | <0.001 † |
| <30% | 4.0% (94/2332) | 2.7% (39/1428) | 0.036 † |
| Alcohol abusus | 7.3% (156/2124) | 6.4% (83/1294) | 0.301 † |
| Preoperative ventilation | 7.5% (182/2423) | 11.3% (167/1476) | <0.001 † |
| EuroSCORE | 11.0 [6.0–17.1] | 10.0 [5.0–18.0] | 0.062 # |
| Microbiology | |||
| Positive blood culture | 61.4% (1487/2423) | 67.8% (1000/1476) | <0.001 † |
| Staphylococcus spp. | 36.4% (497/1364) | 50.2% (456/908) | <0.001 † |
| Streptococcus spp. | 26.7% (364/1364) | 23.8% (216/908) | 0.121 † |
| Enterococcus spp. | 21.0% (286/1364) | 12.1% (110/908) | <0.001 † |
| Other microorganisms | 15.9% (217/1364) | 13.9% (126/908) | 0.185 † |
| Echocardiography | |||
| Presence of vegetation | 57.1% (1384/2423) | 66.6% (983/1475) | <0.001 † |
| Prosthetic valve endocarditis | 33.4% (789/2362) | 16.6% (239/1441) | <0.001 † |
| Pacemaker associated IE | 0.6% (15/2423) | 0.7% (11/1476) | 0.639 † |
| Operative data | |||
| Ascending aortic/root/arch surgery | 24.3% (558/2423) | 2.0% (29/1476) | <0.001 † |
| Concomitant CABG | 12.1% (292/2423) | 13.6% (200/1476) | 0.172 † |
| CPB time | 104.0 [76.0–152.0] | 112.0 [85.0–144.0] | 0.014 # |
| Crossclamp time | 71.0 [51.0–103.0] | 71.0 [54.0–95.0] | 0.469 # |
| Redo operation | 35.0% (848/2423) | 21.2% (313/1476) | <0.001 † |
| Aortic Valve IE (n = 2423) | Mitral Valve IE (n = 1476) | p Value | |
|---|---|---|---|
| 30 day mortality (day 0–30) | 14.6% (314/2153) | 16.7% (206/1231) | 0.095 † |
| 1 year mortality (day 0–365) | 29.0% (549/1893) | 35.3% (384/1088) | <0.001 † |
| Re-exploration | 21.7% (527/2423) | 20.7% (306/1476) | 0.452 † |
| Postoperative stroke | 14.4% (309/2143) | 17.7% (233/1319) | 0.011 † |
| Postoperative hemodialysis | 13.9% (320/2299) | 19.3% (273/1414) | <0.001 † |
| Tracheostomy | 7.0% (169/2423) | 10.2% (150/1476) | <0.001 † |
| ICU stay (days) | 3.0 [1.0–7.0] | 3.0 [1.0–5.0] | <0.001 # |
| Hospital stay (days) | 14.0 [9.0–21.0] | 13.0 [8.0–21.0] | 0.362 # |
| 30 Day Mortality | 1 Year Mortality | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age > 65 years | 1.554 | 1.121–2.154 | 0.008 | 2.046 | 1.564–2.676 | <0.001 |
| Male sex | 0.718 | 0.523–0.985 | 0.040 | 0.718 | 0.558–0.923 | 0.010 |
| LVEF < 30% | 2.537 | 1.310–4.916 | 0.006 | |||
| Coronary artery disease | 1.548 | 1.219–1.967 | <0.001 | |||
| Diabetes | 1.524 | 1.109–2.093 | 0.009 | 1.354 | 1.063–1.724 | 0.014 |
| Pulmonary hypertension | 1.424 | 1.078–1.882 | 0.013 | |||
| Alcohol | 1.830 | 1.259–2.660 | 0.002 | |||
| Preoperative CKD | 1.975 | 1.448–2.695 | <0.001 | 1.708 | 1.320–2.211 | <0.001 |
| Preoperative hemodialysis | 2.099 | 1.460–3.016 | <0.001 | |||
| Preoperative stroke | 1.414 | 1.109–1.803 | 0.005 | |||
| Preoperative ventilation | 2.104 | 1.398–3.169 | <0.001 | 1.537 | 1.095–2.156 | 0.013 |
| Urological focus | 1.410 | 1.024–1.941 | 0.035 | |||
| Wound focus | 1.461 | 1.034–2.065 | 0.032 | |||
| Septic embolism spleen | 1.360 | 1.071–1.728 | 0.012 | |||
| Staphylococcus spp. IE | 1.734 | 1.273–2.362 | <0.001 | |||
| Vegetation | 1.817 | 1.071–3.082 | 0.027 | |||
| Prosthetic valve IE | 1.536 | 1.115–2.117 | 0.009 | |||
| Redo | 1.569 | 1.236–1.991 | <0.001 | |||
| Mitral valve IE | 1.329 | 1.043–1.693 | 0.021 | |||
| Aortic Valve IE | Mitral Valve IE | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Male sex | 0.642 | 0.416–0.991 | 0.045 | |||
| LVEF < 30% | 4.452 | 2.182–9.084 | <0.001 | |||
| Myocardial infarction | 2.134 | 1.031–4.415 | 0.041 | |||
| Diabetes mellitus | 1.711 | 1.136–2.575 | 0.010 | |||
| Smoking | 0.436 | 0.220–0.864 | 0.017 | |||
| Preoperative CKD | 1.901 | 1.283–2.818 | 0.001 | 3.592 | 2.287–5.641 | <0.001 |
| Preoperative ventilation | 2.883 | 1.696–4.901 | <0.001 | |||
| Staphylococcus spp. IE | 1.810 | 1.225–2.673 | 0.004 | |||
| Prosthetic valve IE | 1.782 | 1.206–2.631 | 0.004 | |||
| Aortic Valve IE | Mitral Valve IE | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age >65 years | 1.824 | 1.259–2.643 | 0.001 | 2.302 | 1.557–3.404 | <0.001 |
| Male sex | 0.568 | 0.401–0.804 | 0.001 | |||
| LVEF >50% | 0.670 | 0.450–0.998 | 0.049 | |||
| Hypertension | 0.629 | 0.435–0.912 | 0.014 | 1.947 | 1.251–3.030 | 0.003 |
| Coronary artery disease | 1.610 | 1.165–2.224 | 0.004 | |||
| Diabetes mellitus | 1.951 | 1.344–2.832 | <0.001 | |||
| COPD | 1.614 | 1.098–2.372 | 0.015 | |||
| Preoperative CKD | 1.645 | 1.157–2.339 | 0.006 | 1.528 | 1.026–2.274 | 0.037 |
| Preoperative hemodialysis | 2.028 | 1.233–3.337 | 0.005 | 2.000 | 1.148–3.482 | 0.014 |
| Peripheral vascular disease | 1.964 | 1.330–2.900 | <0.001 | |||
| PAH | 1.495 | 1.021–2.189 | 0.039 | |||
| Alcohol abuse | 1.693 | 1.056–2.716 | 0.029 | |||
| Preoperative ventilation | 1.864 | 1.172–2.965 | 0.009 | |||
| Urological focus | 2.000 | 1.324–3.020 | <0.001 | |||
| Septic embolism kidney | 1.712 | 1.139–2.574 | 0.010 | |||
| Septic embolism spleen | 1.468 | 1.029–2.093 | 0.034 | |||
| Staphylococcus spp. IE | 1.735 | 1.198–2.513 | 0.004 | |||
| Redo | 1.699 | 1.230–2.347 | 0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, C.; Marin-Cuartas, M.; Tugtekin, S.-M.; Diab, M.; Saha, S.; Akhyari, P.; Elderia, A.; Muench, F.; Petrov, A.; Aubin, H.; et al. Aortic and Mitral Valve Endocarditis—Simply Left-Sided Endocarditis or Different Entities Requiring Individual Consideration?—Insights from the CAMPAIGN Database. J. Clin. Med. 2024, 13, 5841. https://doi.org/10.3390/jcm13195841
Weber C, Marin-Cuartas M, Tugtekin S-M, Diab M, Saha S, Akhyari P, Elderia A, Muench F, Petrov A, Aubin H, et al. Aortic and Mitral Valve Endocarditis—Simply Left-Sided Endocarditis or Different Entities Requiring Individual Consideration?—Insights from the CAMPAIGN Database. Journal of Clinical Medicine. 2024; 13(19):5841. https://doi.org/10.3390/jcm13195841
Chicago/Turabian StyleWeber, Carolyn, Mateo Marin-Cuartas, Sems-Malte Tugtekin, Mahmoud Diab, Shekhar Saha, Payam Akhyari, Ahmed Elderia, Florian Muench, Asen Petrov, Hug Aubin, and et al. 2024. "Aortic and Mitral Valve Endocarditis—Simply Left-Sided Endocarditis or Different Entities Requiring Individual Consideration?—Insights from the CAMPAIGN Database" Journal of Clinical Medicine 13, no. 19: 5841. https://doi.org/10.3390/jcm13195841
APA StyleWeber, C., Marin-Cuartas, M., Tugtekin, S.-M., Diab, M., Saha, S., Akhyari, P., Elderia, A., Muench, F., Petrov, A., Aubin, H., Misfeld, M., Lichtenberg, A., Hagl, C., Doenst, T., Matschke, K., Borger, M. A., Wahlers, T., & Luehr, M., on behalf of the Study Group “Clinical, Multicenter Project of Analysis of Infective Endocarditis in Germany” (CAMPAIGN). (2024). Aortic and Mitral Valve Endocarditis—Simply Left-Sided Endocarditis or Different Entities Requiring Individual Consideration?—Insights from the CAMPAIGN Database. Journal of Clinical Medicine, 13(19), 5841. https://doi.org/10.3390/jcm13195841