
Does Surgical Treatment for Benign Prostate Enlargement (BPE)-Related Bladder Outlet Obstruction (BOO) Benefit Patients with Central Nervous System Diseases? A Systematic Review
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Types of Study Design
2.3. Types of Participants
2.4. Types of Intervention
2.5. Outcome Measures
2.6. Assessment of Risk of Bias
2.7. Data Analysis
3. Results
3.1. Quantity of Evidence Identified
3.2. Characteristics of the Included Studies
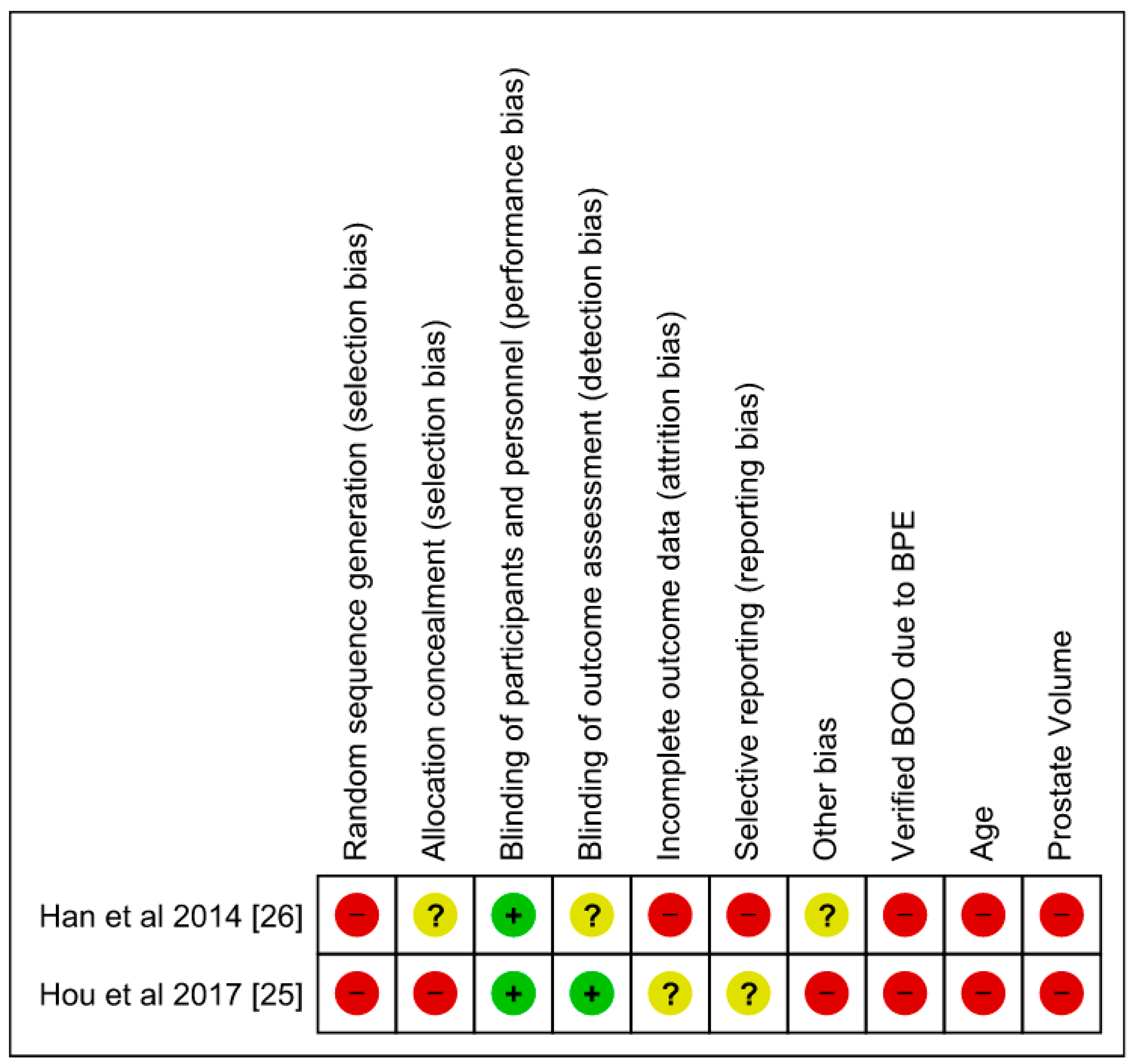
3.3. RoB and Confounding Assessment of the Included Studies
3.4. Narrative Synthesis of the Results
3.4.1. Description of Population Characteristics from the Included Studies
Spinal Cord Injury Population
Parkinson’s Disease Population
Post-Cerebrovascular Accident Population
Multiple Systemic Atrophy Population
3.4.2. Primary Outcome
Spinal Cord Injury Population
Parkinson’s Disease Population
Post-Cerebrovascular Accident Population
3.4.3. Secondary Outcomes
Postoperative Change in Continence
Postoperative Change in Urodynamic Parameters
Postoperative Changes in Questionnaires and Quality of Life Scores
Perioperative Complications
Need for Additional Medical or Surgical Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Gravas, S.; Gacci, M.; Gratzke, C.; Herrmann, T.R.W.; Karavitakis, M.; Kyriazis, I.; Malde, S.; Mamoulakis, C.; Rieken, M.; Sakalis, V.I.; et al. Summary Paper on the 2023 European Association of Urology Guidelines on the Management of Non-neurogenic Male Lower Urinary Tract Symptoms. Eur. Urol. 2023, 84, 207–222. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.J.; Coffey, D.S.; Walsh, P.C.; Ewing, L.L. The development of human benign prostatic hyperplasia with age. J. Urol. 1984, 132, 474–479. [Google Scholar] [CrossRef]
- Lepor, H. Pathophysiology of lower urinary tract symptoms in the aging male population. Rev. Urol. 2005, 7 (Suppl. S7), S3–S11. [Google Scholar]
- Przydacz, M.; Chlosta, M.; Golabek, T.; Chlosta, P. Population-Based Study of Prevalence, Bother and Behavior Related to Treatment for Lower Urinary Tract Symptoms and Overactive Bladder among Polish Neurogenic Patients. Brain Sci. 2021, 11, 712. [Google Scholar] [CrossRef] [PubMed]
- Pannek, J.; Berges, R.R.; Cubick, G.; Meindl, R.; Senge, T. Prostate size and PSA serum levels in male patients with spinal cord injury. Urology 2003, 62, 845–848. [Google Scholar] [CrossRef]
- Shim, H.B.; Kim, Y.D.; Jung, T.Y.; Lee, J.K.; Ku, J.H. Prostate-specific antigen and prostate volume in Korean men with spinal cord injury: A case-control study. Spinal Cord 2008, 46, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Utomo, E.; Groen, J.; Blok, B.F. Surgical management of functional bladder outlet obstruction in adults with neurogenic bladder dysfunction. Cochrane Database Syst. Rev. 2014, 2014, CD004927. [Google Scholar] [CrossRef]
- Kim, M.; Jeong, C.W.; Oh, S.J. Diagnostic value of urodynamic bladder outlet obstruction to select patients for transurethral surgery of the prostate: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0172590. [Google Scholar] [CrossRef]
- Han, T.M.; Shenot, P.J.; Uhr, A.; Glick, L.; Das, A.K. The Evidence For and Against Prostate-Reducing Procedures for Men with Neurogenic Bladder. Curr. Bladder Dysfunct. Rep. 2020, 15, 296–302. [Google Scholar] [CrossRef]
- Noordhoff, T.C.; Groen, J.; Scheepe, J.R.; Blok, B.F.M. Surgical Management of Anatomic Bladder Outlet Obstruction in Males with Neurogenic Bladder Dysfunction: A Systematic Review. Eur. Urol. Focus 2019, 5, 875–886. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing the risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions v.5.0.2. The Cochrane Collaboration. 2011. Available online: http://www.cochrane-handbook.org/ (accessed on 10 February 2014).
- Knoll, T.; Omar, M.I.; Maclennan, S.; Hernández, V.; Canfield, S.; Yuan, Y.; Bruins, M.; Marconi, L.; Van Poppel, H.; N’dow, J.; et al. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur. Urol. 2017, 73, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Roth, B.; Studer, U.E.; Fowler, C.J.; Kessler, T.M. Benign prostatic obstruction and parkinson’s disease—should transurethral resection of the prostate be avoided? J. Urol. 2009, 181, 2209–2213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Kuo, H.C. Satisfaction with Surgical Procedures and Bladder Management of Chronic Spinal Cord Injured Patients with Voiding Dysfunction Who Desire Spontaneous Voiding. J. Pers. Med. 2022, 12, 1751. [Google Scholar] [CrossRef]
- Sampogna, G.; Barbosa, F.; Brambillasca, P.M.; Montanari, E.; Rampoldi, A.; Spinelli, M. Prostatic artery embolization in people with spinal cord injury: A safe and effective technique to ease intermittent catheterization in case of concomitant benign prostatic hyperplasia. Spinal Cord Ser. Cases 2022, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Shinno, Y.; Koyanagi, T.; Kakizaki, H.; Kobayashi, S.; Ameda, K.; Morita, H. Urinary control after radical transurethral resection of the prostate in male paraplegics: Urodynamic evaluation of its effectiveness in relieving incontinence. Int. J. Urol. 1994, 1, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Staskin, D.S.; Vardi, Y.; Siroky, M.B. Post-prostatectomy continence in the parkinsonian patient: The significance of poor voluntary sphincter control. J. Urol. 1988, 140, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, T.; Morita, H.; Takamatsu, T.; Taniguchi, K.; Shinno, Y. Radical transurethral resection of the prostate in male paraplegics revisited: Further clinical experience and urodynamic considerations for its effectiveness. J. Urol. 1987, 137, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Koyanagi, T.; Arikado, K.; Tsuji, I. Radical transurethral resection of the prostate for neurogenic dysfunction of the bladder in male paraplegics. J. Urol. 1981, 125, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.; Betts, C.; Fowler, C.J. Genitourinary dysfunction in multiple system atrophy: Clinical features and treatment in 62 cases. J. Urol. 1994, 151, 1336–1341. [Google Scholar] [CrossRef] [PubMed]
- Lum, S.K.; Marshall, V.R. Results of prostatectomy in patients following a cerebrovascular accident. Br. J. Urol. 1982, 54, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Elsaesser, E.; Stoephasius, E. Urological operations for improvement of bladder voiding in paraplegic patients. Paraplegia 1972, 10, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.L.; Chen, S.F.; Kuo, H.C. Surgical outcome of male patients with chronic central nervous system disorders and voiding dysfunction due to bladder outlet obstruction. Int. Urol. Nephrol. 2022, 54, 2511–2519. [Google Scholar] [CrossRef]
- Hou, C.P.; Lin, Y.H.; Chen, T.H.; Chang, P.L.; Juang, H.H.; Chen, C.L.; Yang, P.S.; Tsui, K.H. Transurethral resection of the prostate achieves favorable outcomes in stroke patients with symptomatic benign prostate hyperplasia. Aging Male 2018, 21, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Han, H.H.; Ko, W.J.; Yoo, T.K.; Oh, T.H.; Kim, D.Y.; Kwon, D.D.; Byun, S.S.; Kim, S.I.; Jung, T.Y. Factors associated with continuing medical therapy after transurethral resection of prostate. Urology 2014, 84, 675–680. [Google Scholar] [CrossRef]
- Gammon, S.R.; Berni, K.C.; Virgo, K.S.; Johnson, F.E. Surgical treatment for prostate cancer in patients with prior spinal cord injury. Ann. Surg. Oncol. 2005, 12, 674–678. [Google Scholar] [CrossRef]
- Begg, C.B.; Riedel, E.R.; Bach, P.B.; Kattan, M.W.; Schrag, D.; Warren, J.L.; Scardino, P.T. Variations in morbidity after radical prostatectomy. N. Engl. J. Med. 2002, 346, 1138–1144. [Google Scholar] [CrossRef]
- Cornu, J.N.; Ahyai, S.; Bachmann, A.; de la Rosette, J.; Gilling, P.; Gratzke, C.; McVary, K.; Novara, G.; Woo, H.; Madersbacher, S. A Systematic Review and Meta-analysis of Functional Outcomes and Complications Following Transurethral Procedures for Lower Urinary Tract Symptoms Resulting from Benign Prostatic Obstruction: An Update. Eur. Urol. 2015, 67, 1066–1096. [Google Scholar] [CrossRef]
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 3, 17013. [Google Scholar] [CrossRef]
- Poewe, W. Non-motor symptoms in Parkinson’s disease. Eur. J. Neurol. 2008, 15 (Suppl. S1), 14–20. [Google Scholar] [CrossRef]
- Li, F.-F.; Cui, Y.-S.; Yan, R.; Cao, S.-S.; Feng, T. Prevalence of lower urinary tract symptoms, urinary incontinence and retention in Parkinson’s disease: A systematic review and meta-analysis. Front. Aging Neurosci. 2022, 14, 977572. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Sakakibara, R.; Kuno, S.; Ishizuka, O.; Kitta, T.; Yoshimura, N. Prevalence and treatment of LUTS in patients with Parkinson disease or multiple system atrophy. Nat. Rev. Urol. 2016, 14, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.; A Bennett, D.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Choi, J.G.; Shin, J.H. Urological disturbance and its neuroanatomical correlate in patients with chronic brainstem stroke. Neurourol. Urodyn. 2017, 36, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Pettersen, R.; Wyller, T.B. Prognostic significance of micturition disturbances after acute stroke. J. Am. Geriatr. Soc. 2006, 54, 1878–1884. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Kumar, A.; Saroj, U.; Kumar, R.; Singh, S.K.; Choudhary, A.K.; Farheen, Z.; Priya, S. A Study on the Clinical Profiles of Patients With Cerebrovascular Accident (Stroke) in a Tertiary Care Hospital in Jharkhand. Cureus 2023, 15, e35919. [Google Scholar] [CrossRef]
- Nwachukwu, C.E.; Nwachukwu, J.; Okpala, B.C.; Nwachukwu, C.A.; Oranusi, I.O.; Ufoaroh, C.U.; Okpala, A.N.; Ofojebe, C.J.; Umeononihu, O.S.; Nwajiaku, L.A. A 7-year review of medical admission profile for clinical diseases in an intensive care unit of a low-resource setting. SAGE Open Med. 2023, 11, 20503121231153104. [Google Scholar] [CrossRef]
- Mattiasson, A.; Djurhuus, J.C.; Fonda, D.; Lose, G.; Nordling, J.; Stöhrer, M. Standardization of outcome studies in patients with lower urinary tract dysfunction: A report on general principles from the Standardisation Committee of the International Continence Society. Neurourol. Urodyn. 1998, 17, 249–253. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Data Extraction Sheet | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID | Study DesignPeriod | Included NU Patients/Study Population | Type of NU Patients (%) | Type of Intervention (%) | Patient Age (Mean, yr) | Type of NLUTD (Symptoms %) | Indication for Surgery | Preoperative Bladder Management | Preoperative Incontinence (%) | Follow-up Time | Risk of Bias | |
| Roth et al. (2009) [14] | Retrospective, 1997–2007 | 23/23 (100%) | 23/23(100%) Parkinson’s disease (Hoehn and Yarh scale ≤3) | TURP 23/23 (100%) | Median 73 (IQR: 68–81) | Voiding (23/23) 100%, Urge Incontinence (10/23) 43% | LUTS refractory to medical therapy | IDC: 14/23 (61%) VWC: 9/23 (39%) | UUI: 10/23 (43%) | Median 3 yr (IQR 2–6) | High Risk | |
| Wu et al. (2022) [15] | Retrospective, 1997–2020 | 261/261 * | 77/77 (100%) SCI Cervical SCI: 43/77 (56%) Thoracic SCI: 13/77 (17%) Lumbar/sacral SCI: 21/77 (27%) | TUIP/TURP 77/77 (100%) | NR | NR | LUTS refractory to medical therapy | NR | 0% | Median 11 years (IQR 6.17) | High Risk | |
| Sampogna et al. (2022) [16] | Retrospective, 2015–2020 | 10/10 (100%) | 10/10 (100%) SCI Cervical SCI: 5/10 (50%) Thoracic/sacral SCI: 5/10 (50%) | Prostatic Artery Embolization (PAE) 10/10 (100%) | Median 70 (Range:59–86) | Urinary retention, BOO | Difficulties in performing ISC due to BPH 10/10 (100%) | IDC: 7/10 (7%) ISC: 3/10 (30%) | 0% | Median 33 months | High Risk | |
| Shino et al. (1994) [17] | Retrospective, 1977–1989 | 51/51 (100%) | 51/51 (100%) SCI Cervical SCI: 8/51 (16%) Thoracic SCI: 25/51 (49%) Lumbar/sacral SCI: 18/51 (35%) | TURP* Radical TUR-P that includes the resection of the peripheral zone down to the anatomical capsule | Mean: 49.2 (Range: 22–73) | Voiding 51/51: (100%), Incontinence: 42/51 (82%) * Mild UI: 14/42 (33.3%) * Moderate UI: 22/42 (52.4%) * Severe UI: 6/42 (14.3%) | LUTS refractory to medical therapy | VWC: 29/51 (57%) ISC: 11/51 (21.5%) IDC: 11/51 (21.5%) | UI: 42/51 (82%) * Not specified type of incontinence | NR | High Risk | |
| Stanskin et al. (1988) [18] | Retrospective, 1977–1984 | 36/50 (72%) | 36/36 (100% Parkinson’s disease) | TURP36/36 (100%) | NR (entire population mean 67, range 50–82 | 92% OAB, 8% acontrile detrusor (entire population) | BOO | NR | UI 6/36 (17%) * UUI: 4/6 (67%) * Overflow UI: 2/6 (33%) | Median 9.2 months (1 to 28 months) | High Risk | |
| Koyanagi et al. (1987) [19] | Retrospective, 1981–1986 | 89/89 (100%) | 89/89 (100%) SCI Cervical SCI: 20/89 (22.5%) Thoracic SCI: 34/89 (38%) Lumbar/sacral SCI: 35/89 (39.5%) | 89/89 TURP*Radical TUR-P includes the resection of the peripheral zone down to the anatomical capsule | Mean: 50 (Range: 20–80) | Voiding 89/89 (100%), due to DSD | Voiding LUTS | IDC: 89/89 (100%) | 0/89 (100%) | Mean follow-up of ~4 years | High Risk | Same group as Shinno et al. |
| Koyanagi et al. (1981) [20] | Retrospective, NR | 50/50 (100%) | 50/50 (100%) SCI Cervical SCI: 12/50 (24%) Thoracic SCI: 20/50 (40%) Lumbar/sacral SCI: 18/50 (36%) | 59/50 TURP*Radical TUR-P that includes the resection of the peripheral zone down to the anatomical capsule | NR | Voiding 50/50(100%) | Unsatisfactory voiding function defined as PVR >50 mL and Qmax <5 mL/s and detrusor pressure during voiding <60 cmH20. Additionally, patients with SCI and worsening kidney function | IDC: 50/50 (100%) | 0/50 (0%) | Longest 5 years, shortest 6 months; mean 2.5 years | High Risk | |
| Beck et al. (1994) [21] | Retrospective, 1987–1994 | 46/62 (100%) | 62/62 (100%) Multiple system atrophy | 20/46 (44%) TUR P | NR | Voiding suggecting BOO | Voiding LUTS | NR | 0/20 (0%) | NR | High Risk | |
| Hou et al. (2017) [25] | Retrospective comparative study, 1997–2012 | 577/6625 (8.7%) | 577/577 (100%) CVA patients | TURP | CVA: 74.1 ± 7.9 vs. non-CVA: 71.9 ± 8.3 | UTIs within 3 months: 27.7% (160/577) vs. 18.4% (1112/6048) AUR: 47.7% (275/577) vs. 34.3% (2075/6048) | AUR, UTIs | NR | NR | 5.0± 3.8 vs. 6.9 ± 4.4 years | High Risk | |
| Han et al. (2014) [26] | Retrospective comparative study, 2009–2011 | 31/372 (8%) | 31/31 (100%) CVA | 31/31 (100%) TURP | NR | Urinary retention, BOO, | Medications | 0% | 3 months | High Risk | ||
| Lum et al. (1982) [22] | Retrospective, 1975–1979 | 39/39 (100%) | 39/39 (100%) CVA | 32/39 (94.1%) TURP, 7/39 (5.9%) open prostatectomy | 72.4 | AUR, chronic retention, prostatism, and incontinence | Acute and chronic urinary retention, prostatism, and incontinence | NR | NR | 11–15 months | High Risk | |
| Elsaesser and Stoephasius (1972) [23] | Retrospective, 1969–1971 | 35/46 (76.1%) | SCI | 21/35 (60%) TURP, 14/35 (40%) Bladder neck incision | NR | NR | To improve voiding | NR | NR | NR | High Risk | |
| Chang et al. (2022) [24] | Retrospective, NR | 64/64 (100%) | 44/64 (68.7%): CVA 11/64 (17.2%)-Parkison’s disease, 8/64 (12.5%): early-stage demetia | TURP, TUI-P, TUI-BN | 71.1 ± 9.8 | OAB, BOO refractory to medical treatment, nocturia, urgency, and urinary incontinence | BOO | NR | 37/64 (58.7%) | Median 2 years (6–60 months) | High Risk | |
| Chang et al. (2022) [24] | Retrospective, NR | 64/64 (100%) | 44/64 (68.7%): CVA 11/64 (17.2%)-Parkison’s disease, 8/64 (12.5%): early-stage demetia | TURP, TUI-P, TUI-BN | 71.1 ± 9.8 | OAB, BOO refractory to medical treatment, nocturia, urgency, and urinary incontinence | BOO | NR | 37/64 (58.7%) | Median 2 years (6–60 months) | High Risk | |
| Data Extraction Sheet | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Study ID | Success (Defined as per Trialist) | Change in Incontinence Episodes After Surgery | Change in Urodynamic Parameters after Surgery | Change in Questionaire Scores | Change in QoL | Changes(Catheters Before/After, Pads Before/After, etc.) | Adverse Effects After Surgery | Need for Reoperation–Reintervention | |
| Roth et al. (2009) [14] | Definition of success: improvement of voiding parameters and change in bladder management 16/23 (70%) | No episodes of de novo UI 5/10 men with UUI restored continence (50%) 3/10 men with UUI had improved continence (30%) | Qmax: +10 mL/s (p = 0.028) * VV: +220 mL (p = 0.018) # | IPSS total score: −12 (p = 0.028) # | IPSS QoL score: −2 (p = 0.026) # | 9/14 (64%) restored voiding. 1/14 (7%) on IDC 4/14 (29%) on ISC | NR | NR | |
| Wu et al. (2022) [15] | Definition of success: patient satisfaction 50/77 (65%) Cervical SCI: 29/43 (67.4%) Thoracic SCI: 9/13 (69.2%) Lumbar/sacral SCI: 12/21 (57.1%) | UI (UUI/SUI) 19/77 (24.7%) | NR | NR | 86.5% satisfied, no official questionnaires | NR | Recurrent UTIs 65/77 (82%) Difficult Urination 41/77 (59%) UI (UUI/SUI) 19/77 (24.7%). Autonomic dysreflexia 12/77 (15.6%) | 34/77 (44.2%) Botox 9/24 (37.5%) TUI-BN: 4/24 (16.7%) Re-TUIP/TURP: 11/24 (45.8%) | |
| Sampogna et al. (2022) [16] | Definition of success: * Easy ISC 10/10 (100%) * Technical success (bilateral embolization) 9/10 (100%) | NR | NR | NR | NR | ISC: 10/10 (100%) | none | 0/10 (0%) for BPH 1/10 (10%) Botox to external urethral sphincter | |
| Shino et al. (1994) [17] | Definition of success: * Subjective or objective improvement of voiding: 47/51 (90%) * UI improved or resolved: 16/42 (38%) | 4/9 men developed de novo SUI (45%). 4/42 men with UI restored continence (10%) 12/42 men with UI had improved continence (29%) 25/42 men with UI were unchanged (59.5%) 1/42 men with UI had worsened continence (2.4%) | * Compliance: + 14.1 mL/cmH20 (p < 0.01) * Detrusor overactivity: present in 11 of 25 men (−28%) * Mean Pdet at filling: −21.3 cmH20 (p < 0.01) * Cystometric capacity: 0.2 mL (p > 0.05) * Maximum urethral closing pressure:−16.9 cmH20 (p < 0.01) | NR | NR | NR | NR | NR | |
| Stanskin et al. (1988) [18] | Definition of success: * UI improved or resolved: 2/6 (33%) | 10/36 men had UUI (28%) 6/30 men developed de novo UI (20%) 4/6 men with preop UUI were unchanged (67%) 2/6 men with preop overflow UI became continent (33%) | NR | NR | NR | NR | NR | NR | |
| Koyanagi et al. (1987) [19] | Definition of success: * Voiding without further intervention 86.5% (77/89) | 1/89 developed de novo SUI (1.2%) due to sphincter injury | PVR: −35.2 mL (p < 0.05) -Flow rate: +15 mL/s (0.05) -VUR was resolved in 15/23 ureters (65%), unchanged in 4/23(17%), and improved in 3/23 (13%) -Compliance: + 22.5 mL/cmH20 (p < 0.05) * -Detrusor overactivity: diagnosed in 15 of 26 men and improved or resolved in 13/15. -Mean Pdet at filling: −16.2 cmH20 (p < 0.05) -Maximum urethral closing pressure:−5.0 cmH20 (p > 0.05) * Data on 26/81 patients only. | NR | NR | NR | 1/89 VUR upgrade | 12/89 men required further treatment. 5/12 (41%) repeat TURP or Y-V plasty | Same group as Shinno et al. |
| Koyanagi et al. (1981) [20] | Definition of success: * Patient rendered catheter-free 46/50 (92.0%) | NR | PVR: −20 mL -Flow rate: +7 mL/s -Voided volume: +140 mL | NR | NR | Patient rendered catheter-free 46/50 (92.0%) | NR | NR | |
| Beck et al. (1994) [21] | NR | 12/20 (60%) urge incontinence | NR | NR | NR | NR | NR | NR | |
| Hou et al. (2017) [25] | Definition of success: * Voiding improvement—reduction of AUR episodes at 12 months after TUR-P: −33% vs.−26.3% (p < 0.001) * Reduction of UTI episodes at 12 months after TUR-P: −4.9% vs.−3.3% (p = 0.002) * Comparison between ischaemic vs. hemorragic CVA: AUR episodes at 12 months: −32.3% vs. −36.7% UTI episodes at 12 months: −5.6% vs. 0% | NR | NR | NR | NR | NR | Perioperative mortality: 6/577 (1%) vs. 7/6048 (0.1%) (p = 0.001) | Re-do prostate surgery 24/577 (4.2%) vs. 422/6048 (7.0%), p = 0.061 | |
| Han et al. (2014) [26] | Definition of success: * No clear definition but assessed the postoperativeuse of medications. CVA men had an odds ratio of 5.932 (p = 0.001) to use LUTS/BPH medications postoperatively | NR | NR | NR | NR | NR | NR | NR | |
| Lum et al. (1982) [22] | Definition of success: * Improvement of symptoms: 17/34 (50.0%) | 17/34 (50%) incontinence post-OP | NR | NR | NR | NR | NR | NR | |
| Elsaesser and Stoephasius (1972) [23] | Definition of success: * Outcome defined as good, improved, or not improved based on urine bacterial growth and PVR Good: 24/35 (68.6%) Improved: 4/35 (11.4%) Not improved: 7/35 (20%) | NR | NR | NR | NR | NR | 1/35 (3%) death due to urosepsis | 2/35 (6%) needed ReTUR-P | |
| Chang et al. (2022) [24] | Definition of success: * Improvement of symptoms Storage symptoms: frequency and urgency improved in 1/11 (9%) Urge incontinence: no improvement | 0/11 men with Parkinson’s disease and UI restored continence (0%) | Parkinson’s -PVR: −24.8 mL (p = 0.005) -Flow rate: +1.7 mL/s (p = 0.511) -Voided volume: −19 mL (p = 0.514) -Voided efficiency: +0.11 (p = 0.04) | NR | NR | NR | NR | NR | |
| Chang et al. (2022) [24] | Definition of success: * Improvement of symptoms Voiding symptoms: urinary retention improved from 18 to 2 men (p < 0.001), dysuria from 37 to 13 men (p < 0.001) Storage symptoms: no change | 9/44 men with CVA had worsened continence from 22/50 to 31/44 0/11 men with Parkinson’s disease and UI restored continence (0%) 1/8 men with dementia had worsened continence (12.5%) | CVA -PVR: −63.4 mL (p = 0.044) -Flow rate: +1.88 mL/s (p = 0.122) -Voided volume: +12 mL (p = 0.677) -Voided efficiency: + 0.18 (p = 0.004) | NR | NR | NR | NR | NR | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charalampous, I.; Tsikopoulos, I.; Mitkani, C.; Samarinas, M.; Yuan, Y.; Vouros, I.; Tsafrakidis, P.; Anastasios, A.; Gkotsi, A.; Sakalis, V. Does Surgical Treatment for Benign Prostate Enlargement (BPE)-Related Bladder Outlet Obstruction (BOO) Benefit Patients with Central Nervous System Diseases? A Systematic Review. J. Clin. Med. 2024, 13, 5846. https://doi.org/10.3390/jcm13195846
Charalampous I, Tsikopoulos I, Mitkani C, Samarinas M, Yuan Y, Vouros I, Tsafrakidis P, Anastasios A, Gkotsi A, Sakalis V. Does Surgical Treatment for Benign Prostate Enlargement (BPE)-Related Bladder Outlet Obstruction (BOO) Benefit Patients with Central Nervous System Diseases? A Systematic Review. Journal of Clinical Medicine. 2024; 13(19):5846. https://doi.org/10.3390/jcm13195846
Chicago/Turabian StyleCharalampous, Ioannis, Ioannis Tsikopoulos, Calypso Mitkani, Michael Samarinas, Yuhong Yuan, Ioannis Vouros, Petros Tsafrakidis, Anastasiadis Anastasios, Anastasia Gkotsi, and Vasileios Sakalis. 2024. "Does Surgical Treatment for Benign Prostate Enlargement (BPE)-Related Bladder Outlet Obstruction (BOO) Benefit Patients with Central Nervous System Diseases? A Systematic Review" Journal of Clinical Medicine 13, no. 19: 5846. https://doi.org/10.3390/jcm13195846