
Radiation Exposure with Self-Expandable Metallic Stent versus Transanal Decompression Tube for Malignant Colorectal Obstruction: A Post Hoc Propensity Score Matched Analysis

 , , , , ,
, , , , ,  , and add
Show full author list
, and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients, Outcomes and Definitions
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients and Lesions
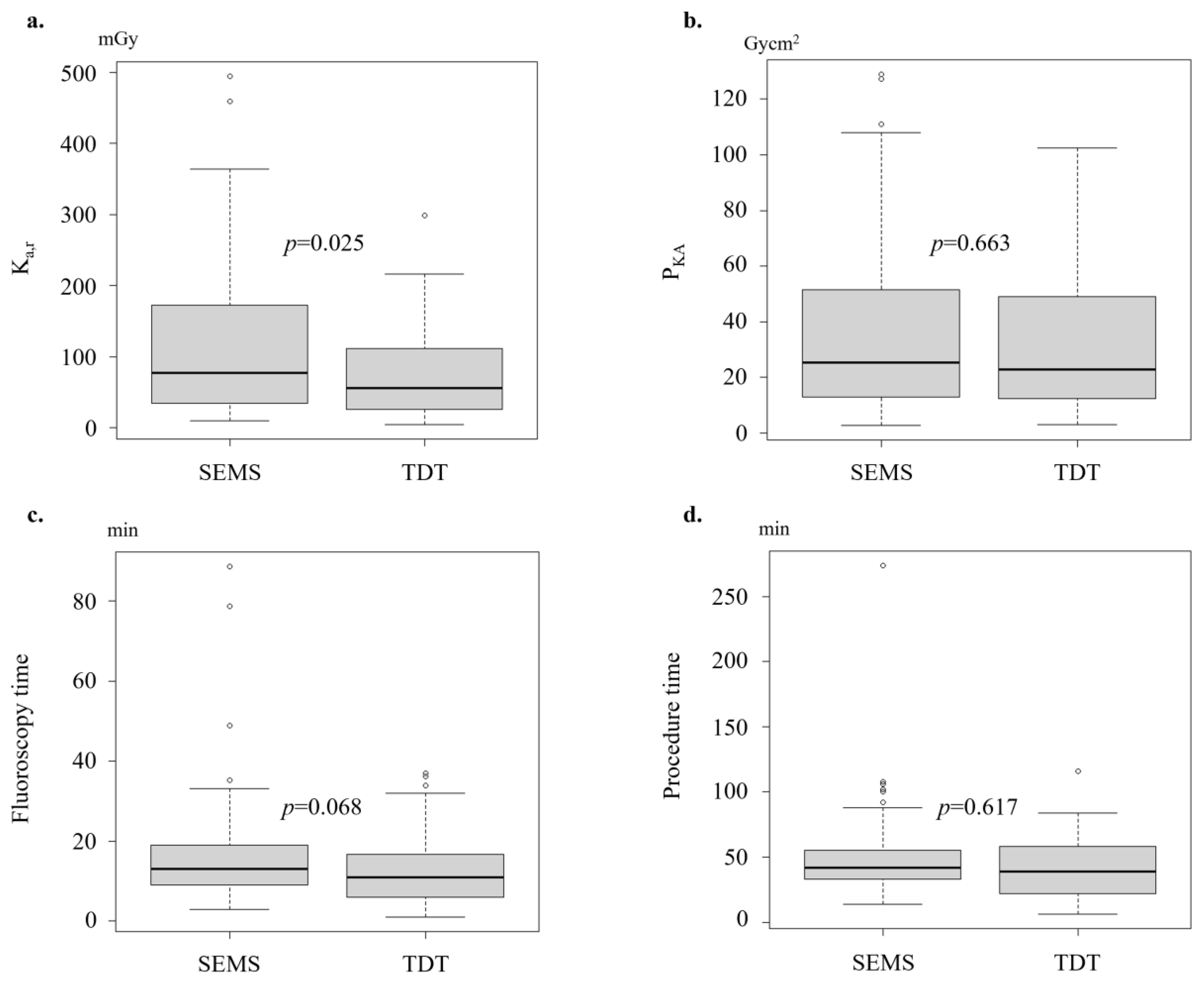
3.2. Radiation Exposure
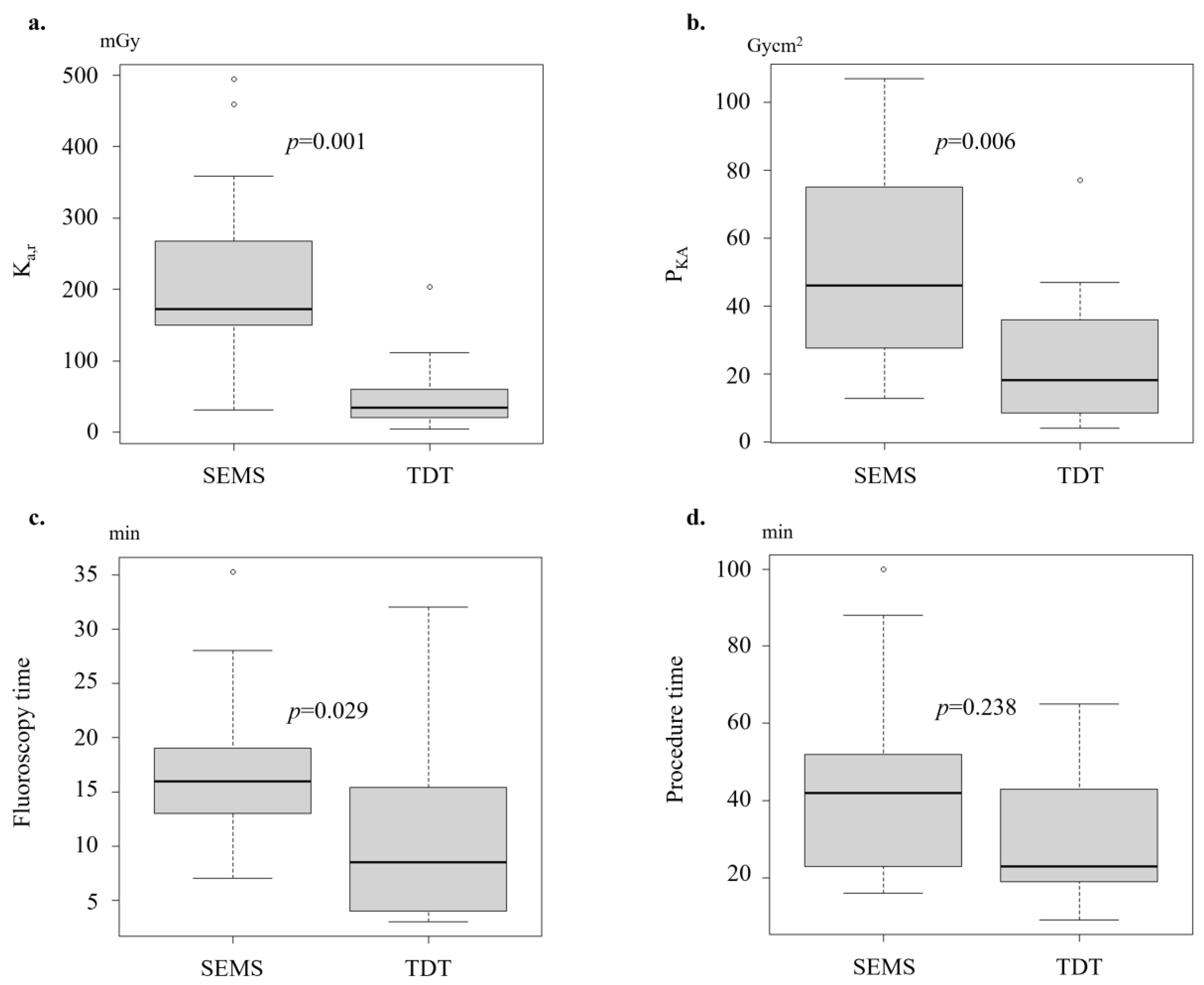
3.3. Subgroup Analyses of Radiation Exposure by Location
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Winner, M.; Mooney, S.J.; Hershman, D.L.; Feingold, D.L.; Allendorf, J.D.; Wright, J.D.; Neugut, A.I. Incidence and predictors of bowel obstruction in elderly patients with stage IV colon cancer: A population-based cohort study. JAMA Surg. 2013, 148, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Mármol, I.; Sánchez-De-Diego, C.; Pradilla Dieste, A.; Cerrada, E.; Rodriguez Yoldi, M. Colorectal Carcinoma: A General Overview and Future Perspectives in Colorectal Cancer. Int. J. Mol. Sci. 2017, 18, 197. [Google Scholar] [CrossRef] [PubMed]
- Van Hooft, J.E.; Veld, J.V.; Arnold, D.; Beets-Tan, R.G.; Everett, S.; Götz, M.; van Halsema, E.E.; Hill, J.; Manes, G.; Meisner, S.; et al. Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline-Update 2020. Endoscopy 2020, 52, 389–407. [Google Scholar] [CrossRef]
- Matsuzawa, T.; Ishida, H.; Yoshida, S.; Isayama, H.; Kuwai, T.; Maetani, I.; Shimada, M.; Yamada, T.; Saito, S.; Tomita, M.; et al. A Japanese prospective multicenter study of self-expandable metal stent placement for malignant colorectal obstruction: Short-term safety and efficacy within 7 days of stent procedure in 513 cases. Gastrointest. Endosc. 2015, 82, 697–707.e1. [Google Scholar] [CrossRef] [PubMed]
- Kuwai, T.; Yamaguchi, T.; Imagawa, H.; Yoshida, S.; Isayama, H.; Matsuzawa, T.; Yamada, T.; Saito, S.; Shimada, M.; Hirata, N.; et al. Factors related to difficult self-expandable metallic stent placement for malignant colonic obstruction: A post-hoc analysis of a multicenter study across Japan. Dig. Endosc. 2019, 31, 51–58. [Google Scholar] [CrossRef]
- Saida, Y. Current status of colonic stent for obstructive colorectal cancer in Japan; a review of the literature. J. Anus Rectum Colon. 2019, 3, 99–105. [Google Scholar] [CrossRef]
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2020, 25, 1–42. [Google Scholar] [CrossRef]
- Kuwai, T.; Tamaru, Y.; Kusunoki, R.; Yoshida, S.; Matsuzawa, T.; Isayama, H.; Maetani, I.; Shimada, M.; Yamada, T.; Saito, S.; et al. Long-term outcomes of standardized colonic stenting using WallFlex as a bridge to surgery: Multicenter prospective cohort study. Dig. Endosc. 2022, 34, 840–849. [Google Scholar] [CrossRef]
- Group, C.R.C. Colorectal Endoscopic Stenting Trial (CReST) for obstructing left-sided colorectal cancer: Randomized clinical trial. Br. J. Surg. 2022, 109, 1073–1080. [Google Scholar] [CrossRef]
- Yamada, T.; Shimura, T.; Sakamoto, E.; Kurumiya, Y.; Komatsu, S.; Iwasaki, H.; Nomura, S.; Kanie, H.; Hasegawa, H.; Orito, E.; et al. Preoperative drainage using a transanal tube enables elective laparoscopic colectomy for obstructive distal colorectal cancer. Endoscopy 2013, 45, 265–271. [Google Scholar] [CrossRef]
- Matsuda, A.; Yamada, T.; Matsumoto, S.; Sakurazawa, N.; Kawano, Y.; Sekiguchi, K.; Matsutani, T.; Miyashita, M.; Yoshida, H. Short-term outcomes of a self-expandable metallic stent as a bridge to surgery vs. a transanal decompression tube for malignant large-bowel obstruction: A meta-analysis. Surg. Today 2019, 49, 728–737. [Google Scholar] [CrossRef] [PubMed]
- Vañó, E.; Miller, D.; Martin, C.; Rehani, M.; Kang, K.; Rosenstein, M.; Ortiz-López, P.; Mattsson, S.; Padovani, R.; Rogers, A. ICRP Publication 135: Diagnostic Reference Levels in Medical Imaging. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef] [PubMed]
- Japan Network for Research and Information on Medical Exposure, (J-RIME). National Diagnostic Reference Levels in Japan (2020) Japan DRLs. 2020. Available online: http://www.radher.jp/J-RIME/report/DRL2020_Engver.pdf (accessed on 25 September 2023).
- Abe, K.; Hosono, M.; Igarashi, T.; Iimori, T.; Ishiguro, M.; Ito, T.; Nagahata, T.; Tsushima, H.; Watanabe, H. The 2020 national diagnostic reference levels for nuclear medicine in Japan. Ann. Nucl. Med. 2020, 34, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Takeyama, H.; Kitani, K.; Wakasa, T.; Tsujie, M.; Fujiwara, Y.; Mizuno, S.; Yukawa, M.; Ohta, Y.; Inoue, M. Self-expanding metallic stent improves histopathologic edema compared with transanal drainage tube for malignant colorectal obstruction. Dig. Endosc. 2016, 28, 456–464. [Google Scholar] [CrossRef]
- Endo, S.; Kumamoto, K.; Enomoto, T.; Koizumi, K.; Kato, H.; Saida, Y. Comparison of survival and perioperative outcome of the colonic stent and the transanal decompression tube placement and emergency surgery for left-sided obstructive colorectal cancer: A retrospective multi-center observational study “The CODOMO study”. Int. J. Color Dis. 2021, 36, 987–998. [Google Scholar] [CrossRef]
- Hayashi, S.; Takenaka, M.; Hosono, M.; Kogure, H.; Hasatani, K.; Suda, T.; Maruyama, H.; Matsunaga, K.; Ihara, H.; Yoshio, T.; et al. Diagnostic Reference Levels for Fluoroscopy-guided Gastrointestinal Procedures in Japan from the REX-GI Study: A Nationwide Multicentre Prospective Observational Study. Lancet Reg. Health West. Pac. 2022, 20, 100376. [Google Scholar] [CrossRef]
- Nishida, T.; Hayashi, S.; Takenaka, M.; Hosono, M.; Kogure, H.; Hasatani, K.; Yamaguchi, S.; Maruyama, H.; Doyama, H.; Ihara, H.; et al. Multicentre prospective observational study protocol for radiation exposure from gastrointestinal fluoroscopic procedures (REX-GI study). BMJ Open 2020, 10, e033604. [Google Scholar] [CrossRef]
- Tokura, J.; Yoshio, T.; Hayashi, S.; Yamamoto, M.; Asai, S.; Yakushijin, T.; Ikezawa, K.; Nagaike, K.; Takagi, T.; Fujisawa, T.; et al. Medical radiation exposure during gastrointestinal enteral metallic stent placement: Post hoc analysis of the REX-GI study. JGH Open 2023, 7, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Song, H.Y.; Kim, J.H.; Kim, K.R.; Shin, J.H.; Kim, H.C.; Yu, C.S.; Kim, J.C. Malignant rectal obstruction within 5 cm of the anal verge: Is there a role for expandable metallic stent placement? Gastrointest. Endosc. 2008, 68, 713–720. [Google Scholar] [CrossRef]
- Tao, K.; Kuwai, T.; Ishaq, S.; Enomoto, T.; Saida, Y. Newly developed proximal release-type colonic stent placement for malignant lower rectal obstruction. VideoGIE 2020, 5, 250–251. [Google Scholar] [CrossRef] [PubMed]
- De Gregorio, M.A.; Laborda, A.; Tejero, E.; Miguelena, J.M.; Carnevale, F.C.; de Blas, I.; Gimenez, M.; Maynar, M.; D’Agostino, H. Ten-year retrospective study of treatment of malignant colonic obstructions with self-expandable stents. J. Vasc. Interv. Radiol. 2011, 22, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Wamba, J.S.; Martínez, A.F.; Pastrana, L.G.; González, L.L.; Arregui, Ó.B. Efficacy and complications in the use of self-expanding colonic stents: An analysis of 15 years’ experience. Radiologia 2015, 57, 402–411. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variables | All Cohort (n = 210) | Propensity-Matched Cohort (n = 122) | ||||
|---|---|---|---|---|---|---|
| SEMS Group (n = 130) | TDT Group (n = 80) | p Value | SEMS Group (n = 61) | TDT Group (n = 61) | p Value | |
| Age, median (IQR), years | 74.0 (67.0–84.0) | 71.0 (54.8–77.0) | 0.002 | 70.0 (64.0–81.0) | 73.0 (57.0–81.0) | 0.665 |
| Sex, male, n (%) | 65 (50.0) | 36 (45.0) | 0.570 | 29 (47.5) | 31 (50.8) | 0.856 |
| Location, colon, n (%) | 117 (90.0) | 50 (62.5) | ˂0.001 | 48 (78.7) | 48 (78.7) | 1.000 |
| Right side | 38 (29.2) | 8 (10.0) | 6 (6.8) | 8 (13.1) | ||
| Left side | 79 (60.8) | 42 (52.5) | 42 (68.9) | 40 (65.6) | ||
| Variables | Before Propensity Score Matching | After Propensity Score Matching | ||||||
|---|---|---|---|---|---|---|---|---|
| Total (n = 210) | SEMS Group (n = 130) | TDT Group (n = 80) | p Value | Total (n = 122) | SEMS Group (n = 61) | TDT Group (n = 61) | p Value | |
| Ka,r, median (IQR), mGy | 60.6 (32.9–124.6) | 62.0 (33.8–124.9) | 57.4 (26.0–123.0) | 0.245 | 63.5 (30.2–148.2) | 77.4 (34.1–172.5) | 55.6 (26.0–111.2) | 0.025 |
| PKA, median (IQR), Gycm2 | 23.0 (13.1–49.8) | 22.7 (13.5–49.8) | 25.2 (12.8–49.2) | 0.814 | 24.4 (12.3–50.0) | 25.3 (12.9–51.6) | 23.0 (12.3–48.9) | 0.663 |
| Fluoroscopy time, median (IQR), min | 11.9 (8.0–17.0) | 12.6 (9.0–18.0) | 11.0 (6.2–16.6) | 0.119 | 11.8 (8.0–18.0) | 13.0 (9.0–19.0) | 10.9 (6.0–16.7) | 0.068 |
| Procedure time, median (IQR), min | 40.0 (26.0–56.8) | 40.0 (31.3–55.8) | 38.5 (23.0–57.3) | 0.103 | 40.0 (26.0–57.8) | 24.0 (20.0–36.0) | 26.0 (14.0–39.0) | 0.617 |
| Variables | SEMS Group | TDT Group | p Value |
|---|---|---|---|
| Colon, n | 48 | 48 | |
| Ka,r, median (IQR), mGy | 64.0 (31.8–125.6) | 57.4 (26.0–124.5) | 0.524 |
| PKA, median (IQR), Gycm2 | 21.6 (11.0–49.3) | 26.7 (14.0–54.9) | 0.303 |
| Fluoroscopy time, median (IQR), min | 12.0 (9.0–18.3) | 11.0 (6.5–18.5) | 0.317 |
| Procedure time, median (IQR), min | 42.5 (33.0–56.5) | 40.0 (25.0–58.3) | 0.250 |
| Rectum, n | 13 | 13 | |
| Ka,r, median (IQR), mGy | 172.9 (149.8–268.0) | 34.6 (21.2–60.3) | 0.001 |
| PKA, median (IQR), Gycm2 | 46.0 (27.6–75.0) | 18.1 (8.5–35.8) | 0.006 |
| Fluoroscopy time, median (IQR), min | 16.0 (13.0–19.0) | 8.5 (4.0–15.4) | 0.029 |
| Procedure time, median (IQR), min | 42.0 (23.0–52.0) | 23.0 (19.0–43.0) | 0.238 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamaru, Y.; Kuwai, T.; Hayashi, S.; Nagaike, K.; Yakushijin, T.; Asai, S.; Yamamoto, M.; Yamaguchi, S.; Yamada, T.; Hasatani, K.; et al. Radiation Exposure with Self-Expandable Metallic Stent versus Transanal Decompression Tube for Malignant Colorectal Obstruction: A Post Hoc Propensity Score Matched Analysis. J. Clin. Med. 2024, 13, 5924. https://doi.org/10.3390/jcm13195924
Tamaru Y, Kuwai T, Hayashi S, Nagaike K, Yakushijin T, Asai S, Yamamoto M, Yamaguchi S, Yamada T, Hasatani K, et al. Radiation Exposure with Self-Expandable Metallic Stent versus Transanal Decompression Tube for Malignant Colorectal Obstruction: A Post Hoc Propensity Score Matched Analysis. Journal of Clinical Medicine. 2024; 13(19):5924. https://doi.org/10.3390/jcm13195924
Chicago/Turabian StyleTamaru, Yuzuru, Toshio Kuwai, Shiro Hayashi, Koji Nagaike, Takayuki Yakushijin, Satoshi Asai, Masashi Yamamoto, Shinjiro Yamaguchi, Takuya Yamada, Kenkei Hasatani, and et al. 2024. "Radiation Exposure with Self-Expandable Metallic Stent versus Transanal Decompression Tube for Malignant Colorectal Obstruction: A Post Hoc Propensity Score Matched Analysis" Journal of Clinical Medicine 13, no. 19: 5924. https://doi.org/10.3390/jcm13195924
APA StyleTamaru, Y., Kuwai, T., Hayashi, S., Nagaike, K., Yakushijin, T., Asai, S., Yamamoto, M., Yamaguchi, S., Yamada, T., Hasatani, K., Ihara, H., Tsumura, H., Doyama, H., Maetani, I., Fujisawa, T., Ito, Y., Takagi, T., Hori, Y., Takenaka, M., ... Nishida, T. (2024). Radiation Exposure with Self-Expandable Metallic Stent versus Transanal Decompression Tube for Malignant Colorectal Obstruction: A Post Hoc Propensity Score Matched Analysis. Journal of Clinical Medicine, 13(19), 5924. https://doi.org/10.3390/jcm13195924