
Gender-Affirming Phalloplasty: A Comprehensive Review
 ,
,
Abstract
1. History of Phalloplasty
2. Indications and Preoperative Evaluation
3. Anatomy
3.1. Penile and Scrotal Anatomy
3.2. Penile Urethral Anatomy
3.3. Vulvar, Vaginal, and Perineal Anatomy
3.4. Urethral Anatomy
3.5. Genital Innervation
4. Surgical Technique
4.1. Staging
4.2. Tube-Within-a-Tube Concept
4.3. Microsurgical Technique
4.4. Flap Neurotization
4.5. Hair Removal
4.6. Flaps Options for Phalloplasty
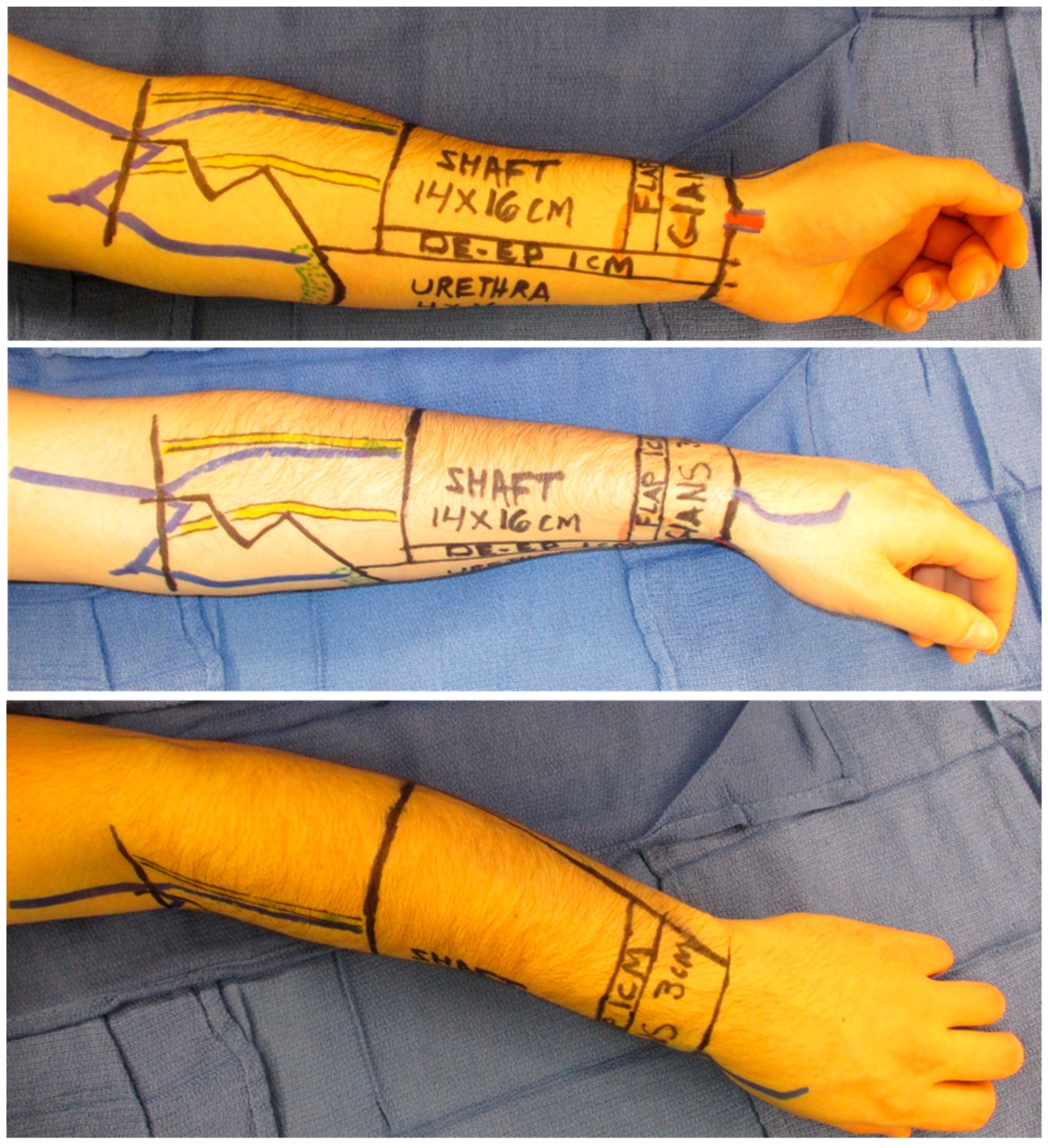
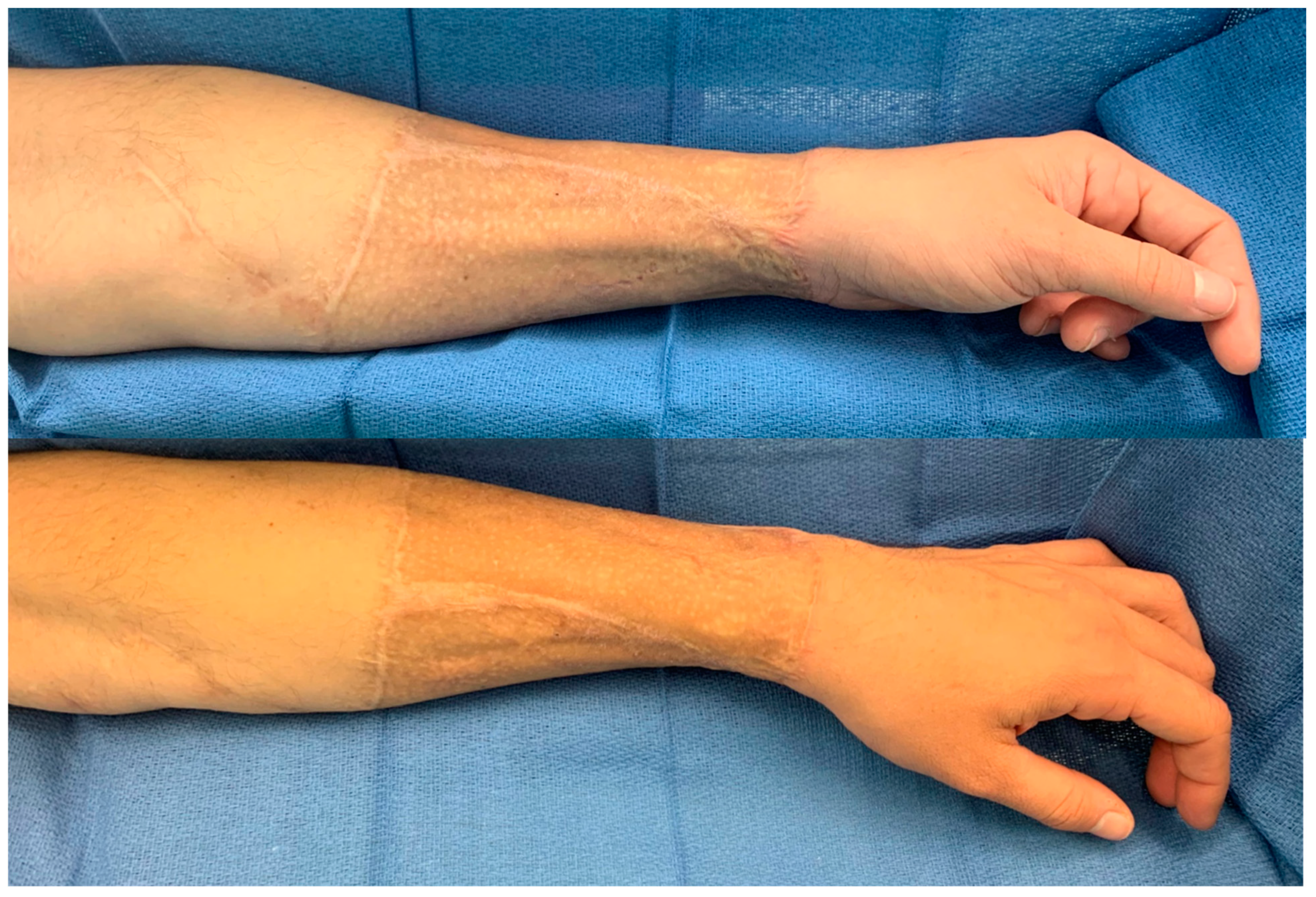
4.6.1. Radial Forearm Free Flap
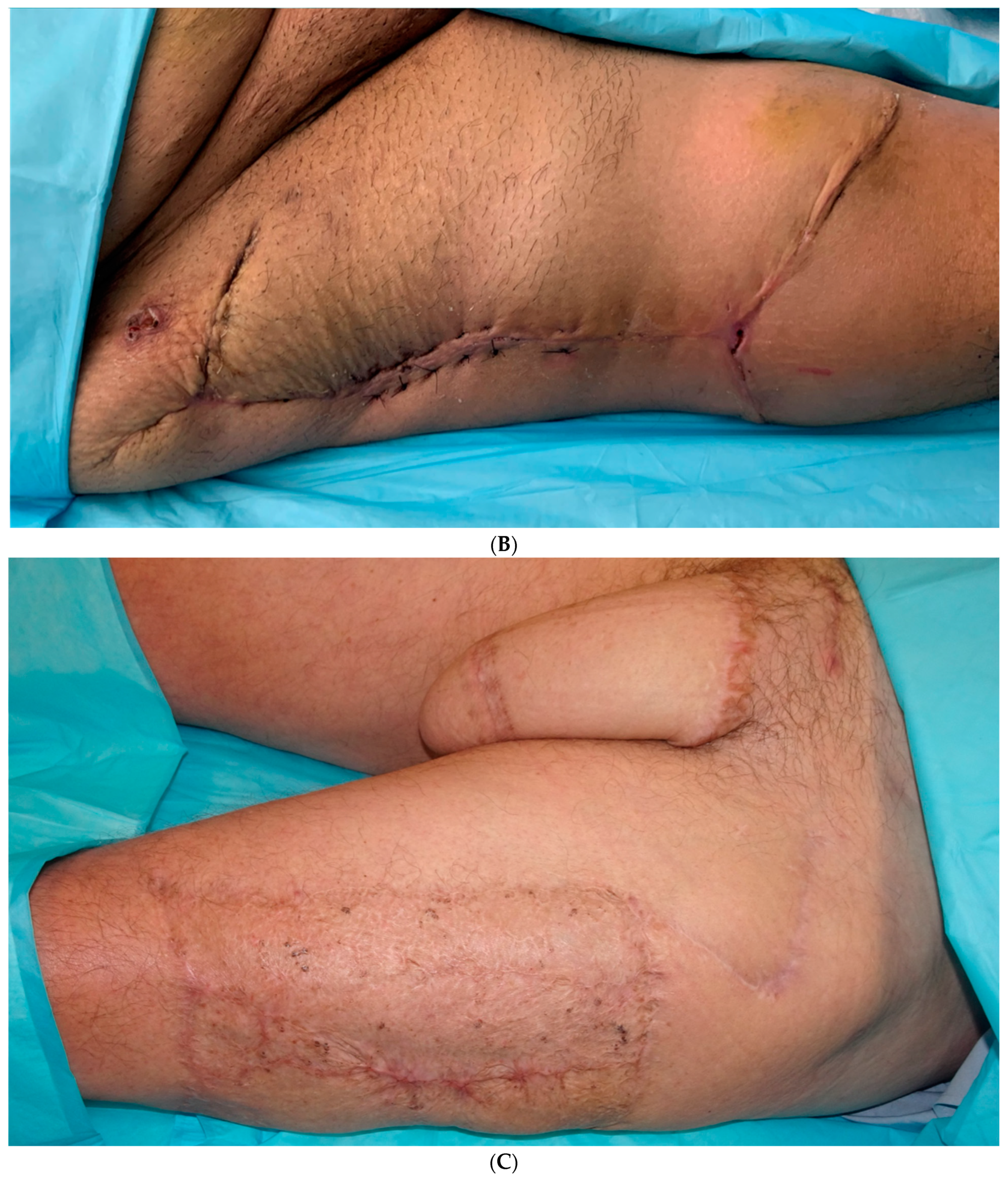
4.6.2. Anterolateral Thigh Flap
4.7. Abdominal-Based Flaps
4.8. Back-Based Donor Sites
4.9. Metoidioplasty
4.10. Adjunct Procedures
5. Outcomes
5.1. Patient-Reported Outcomes
5.2. Complications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schultheiss, D.; Gabouev, A.I.; Jonas, U.; Nikolaj, A. Bogoraz (1874–1952): Pioneer of phalloplasty and penile implant surgery. J. Sex. Med. 2005, 2, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Sriprasad, S. 1129 SIR Harold Gillies: Pioneer of Phalloplasty and the Birth of Uroplastic Surgery. J. Urol. 2010, 183, e437. [Google Scholar] [CrossRef]
- Chang, T.S.; Hwang, W.Y. Forearm flap in one-stage reconstruction of the penis. Plast. Reconstr. Surg. 1984, 74, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, L.J.; Levine, L.A. A new design for the radial forearm free-flap phallic construction. Plast. Reconstr. Surg. 1993, 92, 276–283; discussion 284. [Google Scholar] [CrossRef] [PubMed]
- Huayllani, M.T.; Boczar, D.; Saleem, H.Y.; Cinotto, G.; Avila, F.R.; Manrique, O.J.; Ciudad, P.; Rinker, B.D.; Forte, A.J. Single versus two-stage phalloplasty for transgender female-to-male patients: A systematic review of the literature. Ann. Transl. Med. 2021, 9, 608. [Google Scholar] [CrossRef]
- Coleman, E.; Radix, A.E.; Bouman, W.P.; Brown, G.R.; de Vries, A.L.C.; Deutsch, M.B.; Ettner, R.; Fraser, L.; Goodman, M.; Green, J.; et al. Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. Int. J. Transgender Health 2022, 23, S1–S259. [Google Scholar] [CrossRef]
- Standring, S. Grat’s Anatomy: The Anatomical Basis of Clinical Practice, 42nd ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Bolnick, D.A.; Koyle, M.; Yosha, A. (Eds.) Surgical Guide to Circumcision; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Brandes, S. (Ed.) Urethral Reconstructive Surgery; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Veerman, H.; de Rooij, F.P.W.; Al-Tamimi, M.; Ronkes, B.L.; Mullender, M.G.; Bouman, M.B.; van der Sluis, W.B.; Pigot, G.L.S. Functional Outcomes and Urological Complications after Genital Gender Affirming Surgery with Urethral Lengthening in Transgender Men. J. Urol. 2020, 204, 104–109. [Google Scholar] [CrossRef]
- Bekker, M.D.; Hogewoning, C.R.C.; Wallner, C.; Elzevier, H.W.; DeRuiter, M.C. The somatic and autonomic innervation of the clitoris; preliminary evidence of sexual dysfunction after minimally invasive slings. J. Sex. Med. 2012, 9, 1566–1578. [Google Scholar] [CrossRef]
- Danker, S.; Annen, A.W.; Cylinder, I.; Esmonde, N.O.; Berli, J.U. Technical Description and Microsurgical Outcomes in Phalloplasty Using the Deep Inferior Epigastric Artery and Locoregional Veins. Plast. Reconstr. Surg. 2020, 146, 196e–204e. [Google Scholar] [CrossRef]
- Schechter, L.S.; Safa, B. Introduction to Phalloplasty. Clin. Plast. Surg. 2018, 45, 387–389. [Google Scholar] [CrossRef]
- Thinking outside the Box: Alternative Techniques for Gender Affirming Phalloplasty—Cripps—2023—Neurourology and Urodynamics—Wiley Online Library. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/nau.25104 (accessed on 26 April 2024).
- Safa, B.; Lin, W.C.; Salim, A.M.; Deschamps-Braly, J.C.; Poh, M.M. Current Concepts in Masculinizing Gender Surgery. Plast. Reconstr. Surg. 2019, 143, 857e–871e. [Google Scholar] [CrossRef] [PubMed]
- Kocjancic, E.; Jaunarena, J.H.; Schechter, L.; Acar, Ö. Inflatable penile prosthesis implantation after gender affirming phalloplasty with radial forearm free flap. Int. J. Impot. Res. 2020, 32, 99–106. [Google Scholar] [CrossRef]
- Bluebond-Langner, R.; Redett, R.J. Phalloplasty in complete aphallia and ambiguous genitalia. Semin. Plast. Surg. 2011, 25, 196–205. [Google Scholar] [CrossRef]
- Strategies for Innervation of the Neophallus. Available online: https://www.oaepublish.com/articles/2347-9264.2020.124 (accessed on 25 April 2024).
- Hekner, D.D.; Abbink, J.H.; van Es, R.J.; Rosenberg, A.; Koole, R.; Van Cann, E.M. Donor-site morbidity of the radial forearm free flap versus the ulnar forearm free flap. Plast. Reconstr. Surg. 2013, 132, 387–393. [Google Scholar] [CrossRef]
- Zhang, W.R.; Garrett, G.L.; Arron, S.T.; Garcia, M.M. Laser hair removal for genital gender affirming surgery. Transl. Androl. Urol. 2016, 5, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Esmonde, N.; Bluebond-Langner, R.; Berli, J.U. Phalloplasty Flap-Related Complication. Clin. Plast. Surg. 2018, 45, 415–424. [Google Scholar] [CrossRef]
- Bencic, M.; Stojanovic, B.; Bizic, M.; Djordjevic, M.L. Musculocutaneous Latissimus Dorsi Phalloplasty. Indian. J. Plast. Surg. 2022, 55, 162–167. [Google Scholar] [CrossRef]
- Kojovic, V.; Marjanovic, M.; Radenkovic, A.; Ilic, P.; Simic, R.; Bojovic, B. Latissimus dorsi free flap phalloplasty: A systematic review. Int. J. Impot. Res. 2020, 33, 746–753. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Luo, S.; Yang, Z.; Ma, N.; Li, Y.Q. Deep inferior epigastric vessels for free scapular flap phalloplasty. Medicine 2023, 102, e34603. [Google Scholar] [CrossRef]
- Frey, J.D.; Poudrier, G.; Chiodo, M.V.; Hazen, A. A Systematic Review of Metoidioplasty and Radial Forearm Flap Phalloplasty in Female-to-male Transgender Genital Reconstruction: Is the “Ideal” Neophallus an Achievable Goal? Plast. Reconstr. Surg. Glob. Open 2016, 4, e1131. [Google Scholar] [CrossRef]
- Fascelli, M.; Hennig, F.; Dy, G.W. Penile and testicular prosthesis following gender-affirming phalloplasty and scrotoplasty: A narrative review and technical insights. Transl. Androl. Urol. 2023, 12, 1568–1580. [Google Scholar] [CrossRef] [PubMed]
- Preto, M.; Blecher, G.; Timpano, M.; Gontero, P.; Falcone, M. The Frontier of Penile Implants in Phalloplasty: Is the ZSI 475 FTM what we have been waiting for? Int. J. Impot. Res. 2021, 33, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.M.Q.; Tsang, V.; Mankowski, P.; Demsey, D.; Kavanagh, A.; Genoway, K. Outcomes Following Gender Affirming Phalloplasty: A Systematic Review and Meta-Analysis. Sex. Med. Rev. 2022, 10, 499–512. [Google Scholar] [CrossRef]
- Monstrey, S.; Hoebeke, P.; Selvaggi, G.; Ceulemans, P.; Van Landuyt, K.M.; Blondeel, P.M.; Hamdi, M.M.; Roche, N.; Weyers, S.; De Cuypere, G. Penile reconstruction: Is the radial forearm flap really the standard technique? Plast. Reconstr. Surg. 2009, 124, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Garaffa, G.; Christopher, N.A.; Ralph, D.J. Total phallic reconstruction in female-to-male transsexuals. Eur. Urol. 2010, 57, 715–722. [Google Scholar] [CrossRef]
- Terrier, J.; Courtois, F.; Ruffion, A.; Morel Journel, N. Surgical outcomes and patients’ satisfaction with suprapubic phalloplasty. J. Sex. Med. 2014, 11, 288–298. [Google Scholar] [CrossRef]
- Papadopulos, N.A.; Ehrenberger, B.; Zavlin, D.; Lellé, J.-D.; Henrich, G.P.; Kovacs, L.; Herschbach, P.P.; Machens, H.-G.; Schaff, J. Quality of Life and Satisfaction in Transgender Men After Phalloplasty in a Retrospective Study. Ann. Plast. Surg. 2021, 87, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Wirthmann, A.E.; Majenka, P.; Kaufmann, M.C.; Wellenbrock, S.V.; Kasper, L.; Hüttinger, S.; Djedovic, G.; Bozkurt, A.; Sohn, M.; Rieger, U.M. Phalloplasty in Female-to-Male Transsexuals by Gottlieb and Levine’s Free Radial Forearm Flap Technique-A Long-Term Single-Center Experience Over More than Two Decades. J. Reconstr. Microsurg. 2018, 34, 235–241. [Google Scholar] [CrossRef]
- Papadopulos, N.A.; Schaff, J.; Biemer, E. The use of free prelaminated and sensate osteofasciocutaneous fibular flap in phalloplasty. Injury 2008, 39 (Suppl. S3), S62–S67. [Google Scholar] [CrossRef]
- Massie, J.P.; Morrison, S.D.; Wilson, S.C.; Crane, C.N.; Chen, M.L. Phalloplasty with Urethral Lengthening: Addition of a Vascularized Bulbospongiosus Flap from Vaginectomy Reduces Postoperative Urethral Complications. Plast. Reconstr. Surg. 2017, 140, 551e–558e. [Google Scholar] [CrossRef]
- Al-Tamimi, M.; Pigot, G.L.; van der Sluis, W.B.; van de Grift, T.C.; van Moorselaar, R.J.A.; Mullender, M.G.; Weigert, R.; Buncamper, M.E.; Özer, M.; de Haseth, K.B.; et al. The Surgical Techniques and Outcomes of Secondary Phalloplasty After Metoidioplasty in Transgender Men: An International, Multi-Center Case Series. J. Sex. Med. 2019, 16, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Vesely, J.; Hyza, P.; Ranno, R.; Cigna, E.; Monni, N.; Stupka, I.; Justan, I.; Dvorak, Z.; Novak, P.; Ranno, S. New technique of total phalloplasty with reinnervated latissimus dorsi myocutaneous free flap in female-to-male transsexuals. Ann. Plast. Surg. 2007, 58, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.J.; Nugent, A.G.; Moody, A.M.; Chim, H.; Paz, A.M.; Chen, H.C. Immediate pedicled gracilis flap in radial forearm flap phalloplasty for transgender male patients to reduce urinary fistula. J. Plast. Reconstr. Aesthetic Surgery JPRAS 2016, 69, 1551–1557. [Google Scholar] [CrossRef]
- Bettocchi, C.; Ralph, D.J.; Pryor, J.P. Pedicled pubic phalloplasty in females with gender dysphoria. BJU Int. 2005, 95, 120–124. [Google Scholar] [CrossRef]
- Kim, S.K.; Moon, J.B.; Heo, J.; Kwon, Y.S.; Lee, K.C. A new method of urethroplasty for prevention of fistula in female-to-male gender reassignment surgery. Ann. Plast. Surg. 2010, 64, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Neuville, P.; Morel-Journel, N.; Cabelguenne, D.; Ruffion, A.; Paparel, P.; Terrier, J.E. First Outcomes of the ZSI 475 FtM, a Specific Prosthesis Designed for Phalloplasty. J. Sex. Med. 2019, 16, 316–322. [Google Scholar] [CrossRef]
- Hage, J.J. Dynaflex prosthesis in total phalloplasty. Plast. Reconstr. Surg. 1997, 99, 479–485. [Google Scholar] [CrossRef]
- Hoebeke, P.; de Cuypere, G.; Ceulemans, P.; Monstrey, S. Obtaining rigidity in total phalloplasty: Experience with 35 patients. J. Urol. 2003, 169, 221–223. [Google Scholar] [CrossRef]
- Falcone, M.; Garaffa, G.; Gillo, A.; Dente, D.; Christopher, A.N.; Ralph, D.J. Outcomes of inflatable penile prosthesis insertion in 247 patients completing female to male gender reassignment surgery. BJU Int. 2018, 121, 139–144. [Google Scholar] [CrossRef]
- Campbell, J.D.; Chan, E.P.; Di Pierdominico, A.; Karakus, S.; Trock, B.; Brock, G.B.; Burnett, A.L. Chronic pain associated with penile prostheses may persist despite revision or explantation. Can. Urol. Assoc. J. 2022, 16, 42–46. [Google Scholar] [CrossRef]
- Hagedorn, J.C.; Osbun, N.; Lundy, S.; Miest, T.; Voelzke, B.B. Pd2-10 inflatable penile prosthesis failure and complications: Review of a national database. J. Urol. 2015, 193, e43–e44. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Flap | Advantages | Disadvantages |
|---|---|---|
| Anterolateral thigh | -Relatively large -Can be used as free or pedicled flap -Minimal donor site functional morbidity | -Can be excessively bulky |
| Radial forearm | -Thin, pliable tissue | -Donor site cosmetic and functional morbidity -May not provide sufficient girth for neophallus |
| Abdominal-based flap | -Shorter operative time than that for free flaps -Relatively low donor site morbidity | -Not ideal for urethral lengthening (not amenable to “tube-within-a-tube”) |
| Latissimus dorsi | -Thin, pliable tissue | -Donor site functional morbidity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alba, B.; Nolan, I.T.; Weinstein, B.; O’Neill, E.; Fritsch, A.; Jacobs, K.M.; Schechter, L. Gender-Affirming Phalloplasty: A Comprehensive Review. J. Clin. Med. 2024, 13, 5972. https://doi.org/10.3390/jcm13195972
Alba B, Nolan IT, Weinstein B, O’Neill E, Fritsch A, Jacobs KM, Schechter L. Gender-Affirming Phalloplasty: A Comprehensive Review. Journal of Clinical Medicine. 2024; 13(19):5972. https://doi.org/10.3390/jcm13195972
Chicago/Turabian StyleAlba, Brandon, Ian T. Nolan, Brielle Weinstein, Elizabeth O’Neill, Annie Fritsch, Kristin M. Jacobs, and Loren Schechter. 2024. "Gender-Affirming Phalloplasty: A Comprehensive Review" Journal of Clinical Medicine 13, no. 19: 5972. https://doi.org/10.3390/jcm13195972
APA StyleAlba, B., Nolan, I. T., Weinstein, B., O’Neill, E., Fritsch, A., Jacobs, K. M., & Schechter, L. (2024). Gender-Affirming Phalloplasty: A Comprehensive Review. Journal of Clinical Medicine, 13(19), 5972. https://doi.org/10.3390/jcm13195972