
Reliability and Validity of the Rate of Force Development for Quadriceps in Older Patients with Cardiovascular Disease
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Procedure
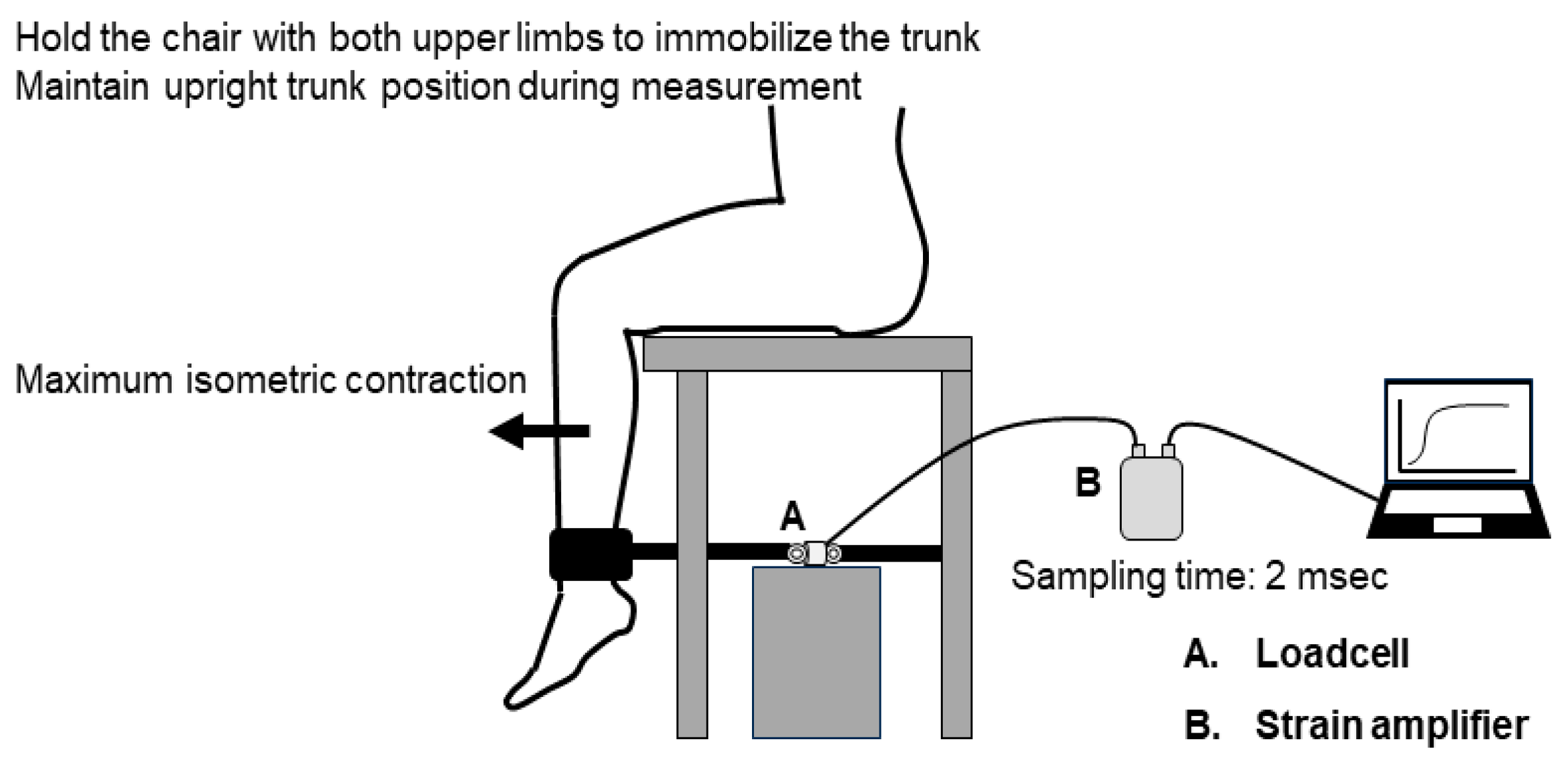
2.3. RFD Quadricep Measurements
2.4. Physical Performance Test
2.5. Clinical Data
2.6. Statistical Analyses
2.7. Ethics
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carbone, S.; Kirkman, D.L.; Garten, R.S.; Rodriguez-Miguelez, P.; Artero, E.G.; Lee, D.C.; Lavie, C.J. Muscular strength and cardiovascular disease: An updated state-of-the-art narrative review. J. Cardiopulm. Rehabil. Prev. 2020, 40, 302–309. [Google Scholar] [CrossRef]
- Kirkman, D.L.; Lee, D.-C.; Carbone, S. Resistance exercise for cardiac rehabilitation. Prog. Cardiovasc. Dis. 2022, 70, 66–72. [Google Scholar] [CrossRef]
- Abreu, A.; Frederix, I.; Dendale, P.; Janssen, A.; Doherty, P.; Piepoli, M.F.; Völler, H.; Davos, C.H.; Ambrosetti, M. Standardization and quality improvement of secondary prevention through cardiovascular rehabilitation programmes in Europe: The avenue towards EAPC accreditation programme: A position statement of the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology (EAPC). Eur. J. Prev. Cardiol. 2021, 28, 496–509. [Google Scholar] [CrossRef]
- Makita, S.; Yasu, T.; Akashi, Y.J.; Adachi, H.; Izawa, H.; Ishihara, S.; Iso, Y.; Ohuchi, H.; Omiya, K.; Ohya, Y.; et al. JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease. Cir. J. 2022, 87, 155–235. [Google Scholar] [CrossRef]
- Prokopidis, K.; Isanejad, M.; Akpan, A.; Stefil, M.; Tajik, B.; Giannos, P.; Venturelli, M.; Sankaranarayanan, R. Exercise and nutritional interventions on sarcopenia and frailty in heart failure: A narrative review of systematic reviews and meta-analyses. ESC Heart Fail. 2022, 9, 2787–2799. [Google Scholar] [CrossRef]
- Bjarnason-Wehrens, B.; Schwaab, B.; Reiss, N.; Schmidt, T. Resistance training in patients with coronary artery disease, heart failure, and valvular heart disease. J. Cardiopulm. Rehabil. Prev. 2022, 42, 304–315. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Zuo, X.; Li, X.; Tang, K.; Zhao, R.; Wu, M.; Wang, Y.; Li, T. Sarcopenia and cardiovascular diseases: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1183–1198. [Google Scholar] [CrossRef]
- Maffiuletti, N.A.; Aagaard, P.; Blazevich, A.J.; Folland, J.; Tillin, N.; Duchateau, J. Rate of force development: Physiological and methodological considerations. Eur. J. Appl. Physiol. 2016, 116, 1091–1116. [Google Scholar] [CrossRef]
- Gollie, J.M.; Harris-Love, M.O.; Patel, S.S.; Shara, N.M.; Blackman, M.R. Rate of force development is related to maximal force and sit-to-stand performance in men with stages 3b and 4 chronic kidney disease. Front. Rehabil. Sci. 2021, 2, 734705. [Google Scholar] [CrossRef]
- Chatrenet, A.; Piccoli, G.; Audebrand, J.M.; Torreggiani, M.; Barbieux, J.; Vaillant, C.; Morel, B.; Durand, S.; Beaune, B. Analysis of the rate of force development reveals high neuromuscular fatigability in elderly patients with chronic kidney disease. J. Cachexia Sarcopenia Muscle 2023, 14, 2016–2028. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Perraton, L.G.; Bower, K.J.; Adair, B.; Pua, Y.-H.; Williams, G.P.; McGaw, R.; Clark, R.A. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: A reliability and validity study. PLoS ONE 2015, 10, e0140822. [Google Scholar] [CrossRef]
- Takeda, K.; Tanabe, S.; Koyama, S.; Nagai, T.; Sakurai, H.; Kanada, Y.; Shomoto, K. Intra- and inter-rater reliability of the rate of force development of hip abductor muscles measured by hand-held dynamometer. Meas. Phys. Educ. Exerc. Sci. 2018, 22, 19–24. [Google Scholar] [CrossRef]
- Ishøi, L.; Hölmich, P.; Thorborg, K. Measures of hip muscle strength and rate of force development using a fixated handheld dynamometer: Intra-tester intra-day reliability of a clinical set-up. Int. J. Sports Phys. Ther. 2019, 14, 715–723. [Google Scholar] [CrossRef]
- Kamiya, K.; Mezzani, A.; Hotta, K.; Shimizu, R.; Kamekawa, D.; Noda, C.; Yamaoka-Tojo, M.; Matsunaga, A.; Masuda, T. Quadriceps isometric strength as a predictor of exercise capacity in coronary artery disease patients. Eur. J. Prev. Cardiol. 2014, 21, 1285–1291. [Google Scholar] [CrossRef]
- Kamiya, K.; Masuda, T.; Tanaka, S.; Hamazaki, N.; Matsue, Y.; Mezzani, A.; Matsuzawa, R.; Nozaki, K.; Maekawa, E.; Noda, C.; et al. Quadriceps strength as a predictor of mortality in coronary artery disease. Am. J. Med. 2015, 128, 1212–1219. [Google Scholar] [CrossRef]
- Nakamura, T.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Ichikawa, T.; Yamashita, M.; Maekawa, E.; Reed, J.L.; Noda, C.; et al. Quadriceps strength and mortality in older patients with heart failure. Can. J. Cardiol. 2021, 37, 476–483. [Google Scholar] [CrossRef]
- Sahaly, R.; Vandewalle, H.; Driss, T.; Monod, H. Maximal voluntary force and rate of force development in humans—Importance of instruction. Eur. J. Appl. Physiol. 2001, 85, 345–350. [Google Scholar] [CrossRef]
- Jaafar, H.; Lajili, H. The influence of verbal instruction on measurement reliability and explosive neuromuscular performance of the knee extensors. J. Hum. Kinet. 2018, 65, 21–34. [Google Scholar] [CrossRef]
- Moir, G.L.; Getz, A.; Davis, S.E.; Marques, M.; Witmer, C.A. The inter-session reliability of isometric force-time variables and the effects of filtering and starting force. J. Hum. Kinet. 2019, 66, 43–55. [Google Scholar] [CrossRef]
- Aagaard, P.; Simonsen, E.B.; Andersen, J.L.; Magnusson, P.; Dyhre-Poulsen, P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J. Appl. Physiol. 2002, 93, 1318–1326. [Google Scholar] [CrossRef] [PubMed]
- Blazevich, A.J.; Horne, S.; Cannavan, D.; Coleman, D.R.; Aagaard, P. Effect of contraction mode of slow-speed resistance training on the maximum rate of force development in the human quadriceps. Muscle Nerve 2008, 38, 1133–1146. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, 85–94. [Google Scholar] [CrossRef]
- Ostir, G.V.; Volpato, S.; Fried, L.P.; Chaves, P.; Guralnik, J.M. Reliability and sensitivity to change assessed for a summary measure of lower body function: Results from the women’s health and aging study. J. Clin. Epidemiol. 2002, 55, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Kitai, T.; Shimogai, T.; Tang, W.H.W.; Iwata, K.; Xanthopoulos, A.; Otsuka, S.; Nakada, F.; Yokoyama, R.; Kamiya, K.; Saito, H.; et al. Short physical performance battery vs. 6-minute walking test in hospitalized elderly patients with heart failure. Eur. Heart J. Open 2021, 1, oeab00. [Google Scholar] [CrossRef]
- Shibata, K.; Kameshima, M.; Adachi, T.; Kito, H.; Tanaka, C.; Sano, T.; Tanaka, M.; Suzuki, Y.; Tamaki, M.; Kitamura, H. Association between preoperative phase angle and all-cause mortality after cardiovascular surgery: A retrospective cohort study. J. Cachexia Sarcopenia Muscle 2024, 15, 1558–1567. [Google Scholar] [CrossRef]
- Bellettiere, J.; Lamonte, M.J.; Unkart, J.; Liles, S.; Laddu-Patel, D.; Manson, J.E.; Banack, H.; Seguin-Fowler, R.; Chavez, P.; Tinker, L.F.; et al. Short physical performance battery and incident cardiovascular events among older women. J. Am. Heart Assoc. 2020, 9, e016845. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Whellan, D.J.; Duncan, P.; Pastva, A.M.; Mentz, R.J.; Reeves, G.R.; Nelson, M.B.; Chen, H.; Upadhya, B.; Reed, S.D.; et al. Physical rehabilitation for older patients hospitalized for heart failure. New Engl. J. Med. 2021, 385, 203–216. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e2. [Google Scholar] [CrossRef]
- Ogawa, M.; Satomi-Kobayashi, S.; Yoshida, N.; Tsuboi, Y.; Komaki, K.; Nanba, N.; Izawa, K.P.; Sakai, Y.; Akashi, M.; Hirata, K. Relationship between oral health and physical frailty in patients with cardiovascular disease. J. Cardiol. 2021, 77, 131–138. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Iijima, H.; Nakamura, M.; Aoyama, T. Rate of force development in the quadriceps of individuals with severe knee osteoarthritis: A preliminary cross-sectional study. PLoS ONE 2022, 17, e0262508. [Google Scholar] [CrossRef] [PubMed]
- Lomborg, S.D.; Dalgas, U.; Hvid, L.G. The importance of neuromuscular rate of force development for physical function in aging and common neurodegenerative disorders—A systematic review. J. Musculoskelet. Neuronal Interact. 2022, 22, 562–586. [Google Scholar]
- Horstman, A.M.; Gerrits, K.H.; Beltman, M.J.; Koppe, P.A.; Janssen, T.W.; de Haan, A. Intrinsic properties of the knee extensor muscles after subacute stroke. Arch. Phys. Med. Rehabil. 2010, 91, 123–128. [Google Scholar] [CrossRef]
- Fimland, M.S.; Moen, P.M.R.; Hill, T.; Gjellesvik, T.I.; Tørhaug, T.; Helgerud, J.; Hoff, J. Neuromuscular performance of paretic versus non-paretic plantar flexors after stroke. Eur. J. Appl. Physiol. 2011, 111, 3041–3049. [Google Scholar] [CrossRef] [PubMed]
- Shimose, R.; Shimizu, S.; Onodera, A.; Shibata, K.; Ichinosawa, Y.; Enoki, I.; Tsunoda, S.; Miura, H.; Watanabe, H.; Matsunaga, A. Decreased rate of leg extensor force development in independently ambulant patients with acute stroke with mild paresis. J. Biomech. 2019, 96, 109345. [Google Scholar] [CrossRef]
- Osawa, Y.; Studenski, S.A.; Ferrucci, L. Knee extension rate of torque development and peak torque: Associations with lower extremity function. J. Cachexia Sarcopenia Muscle 2018, 9, 530–539. [Google Scholar] [CrossRef]
- Burbank, C.M.; Branscum, A.; Bovbjerg, M.L.; Hooker, K.; Smit, E. Muscle Power Predicts Frailty Status over Four Years: A Retrospective Cohort Study of the National Health and Aging Trends Study. J. Frailty Sarcopenia Falls 2023, 8, 1–8. [Google Scholar] [CrossRef]
- Hester, G.M.; Ha, P.L.; Dalton, B.E.; Vandusseldorp, T.A.; Olmos, A.A.; Stratton, M.T.; Bailly, A.R.; Vroman, T.M. Rate of force development as a predictor of mobility in community-dwelling older adults. J. Geriatr. Phys. Ther. 2021, 44, 74–81. [Google Scholar] [CrossRef]
- Staron, R.S.; Hagerman, F.C.; Hikida, R.S.; Murray, T.F.; Hostler, D.P.; Crill, M.T.; Ragg, K.E.; Toma, K. Fiber type composition of the vastus lateralis muscle of young men and women. J. Histochem. Cytochem. 2000, 48, 623–629. [Google Scholar] [CrossRef]
- Buchner, D.M.; Larson, E.B.; Wagner, E.H.; Koepsell, T.D.; de Lateur, B.J. Evidence for a non-linear relationship between leg strength and gait speed. Age Ageing 1996, 25, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Cossich, V.; Maffiuletti, N.A. Early vs. late rate of torque development: Relation with maximal strength and influencing factors. J. Electromyogr. Kinesiol. 2020, 55, 102486. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, J.I.; Maganaris, C.N.; Franchi, M.V.; Smith, K.; Atherton, P.J.; Szewczyk, N.J.; Greenhaff, P.L.; Phillips, B.E.; Blackwell, J.I.; Boereboom, C.; et al. Muscle and tendon contributions to reduced rate of torque development in healthy older males. J. Gerontol. 2018, 73, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Churchward-Venne, T.A.; Tieland, M.; Verdijk, L.B.; Leenders, M.; Dirks, M.L.; de Groot, L.C.P.G.M.; van Loon, L.J.C. There are no nonresponders to resistance-type exercise training in older men and women. J. Am. Med. Dir. Assoc. 2015, 16, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Kitzman, D.W.; Nelson, M.B.; Pastva, A.M.; Duncan, P.; Whellan, D.J.; Mentz, R.J.; Chen, H.; Upadhya, B.; Reeves, G.R. Frailty and effects of a multidomain physical rehabilitation intervention among older patients hospitalized for acute heart failure: A secondary analysis of a randomized clinical trial. JAMA Cardiol. 2023, 8, 167–176. [Google Scholar] [CrossRef]
- Mann, N.; Rosenzweig, A. Can exercise teach us how to treat heart disease? Circulation 2012, 126, 2625–2635. [Google Scholar] [CrossRef]
- Claflin, D.R.; Larkin, L.M.; Cederna, P.S.; Horowitz, J.F.; Alexander, N.B.; Cole, N.M.; Galecki, A.T.; Chen, S.; Nyquist, L.V.; Carlson, B.M.; et al. Effects of high- and low-velocity resistance training on the contractile properties of skeletal muscle fibers from young and older humans. J. Appl. Physiol. 2011, 111, 1021–1030. [Google Scholar] [CrossRef]
- Guizelini, P.C.; de Aguiar, R.A.; Denadai, B.S.; Caputo, F.; Greco, C.C. Effect of resistance training on muscle strength and rate of force development in healthy older adults: A systematic review and meta-analysis. Exp. Gerontol. 2018, 102, 51–58. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outpatients (n = 30) | Inpatients (n = 30) | p | |
|---|---|---|---|
| Age, years | 77 (72–81) | 76 (74–82) | 0.689 |
| Men | 70.0% | 36.7% | 0.010 |
| Body mass index, kg/m2 | 22.2 ± 3.1 | 21.8 ± 4.1 | 0.691 |
| Heart failure | 50.0% | 33.3% | 0.190 |
| Cardiovascular surgery | |||
| CABG | 13.3% | 3.3% | 0.161 |
| Valvular surgery | 33.3% | 30.0% | 0.781 |
| Aortic surgery | 3.3% | 16.7% | 0.071 |
| Concomitant surgery | 6.7% | 23.3% | 0.085 |
| Hypertension | 53.3% | 49.8% | 0.602 |
| Dyslipidemia | 63.3% | 53.3% | 0.432 |
| Diabetes mellitus | 50.0% | 40.7% | 0.015 |
| Left ventricular ejection fraction, % | 51 (41–60) | 55 (45–61) | 0.085 |
| NT-proBNP, pg/mL | 345 (151–792) | 1126 (353–1745) | 0.003 |
| MMSE, points | 28 (26–30) | 27 (23–29) | 0.065 |
| SPPB, points | 12 (11–12) | 9 (8–11) | <0.001 |
| Intra-Rater Reliability | Inter-Rater Reliability | |||||
|---|---|---|---|---|---|---|
| Mean ± SD | ICC (1,1) [95% CI] | Mean ± SD | ICC (2,1) [95% CI] | |||
| Day 1 | Day 2 | Rater 1 | Rater 2 | |||
| RFD50 (Nm/kg/s) | 6.76 ± 5.45 | 6.86 ± 6.01 | 0.742 [0.523–0.868] | 6.86 ± 6.01 | 6.37 ± 4.84 | 0.810 [0.640–0.904] |
| RFD100 (Nm/kg/s) | 7.07 ± 3.18 | 6.08 ± 3.09 | 0.893 [0.528–0.963] | 6.08 ± 3.09 | 6.14 ± 2.87 | 0.918 [0.837–0.961] |
| RFD200 (Nm/kg/s) | 5.07 ± 2.01 | 4.48 ± 2.04 | 0.873 [0.636–0.948] | 4.48 ± 2.04 | 4.52 ± 1.82 | 0.930 [0.858–0.966] |
| MVC (Nm/kg) | 1.62 ± 0.44 | 1.56 ± 0.42 | 0.943 [0.886–0.973] | 1.56 ± 0.42 | 1.55 ± 0.37 | 0.947 [0.891–0.974] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adachi, T.; Morishima, C.; Nojiri, Y.; Tsunekawa, Y.; Tanimura, D.; Sano, T.; Shibata, K.; Kitamura, H. Reliability and Validity of the Rate of Force Development for Quadriceps in Older Patients with Cardiovascular Disease. J. Clin. Med. 2024, 13, 5973. https://doi.org/10.3390/jcm13195973
Adachi T, Morishima C, Nojiri Y, Tsunekawa Y, Tanimura D, Sano T, Shibata K, Kitamura H. Reliability and Validity of the Rate of Force Development for Quadriceps in Older Patients with Cardiovascular Disease. Journal of Clinical Medicine. 2024; 13(19):5973. https://doi.org/10.3390/jcm13195973
Chicago/Turabian StyleAdachi, Takuji, Chubu Morishima, Yuta Nojiri, Yuki Tsunekawa, Daisuke Tanimura, Taisei Sano, Kenichi Shibata, and Hideki Kitamura. 2024. "Reliability and Validity of the Rate of Force Development for Quadriceps in Older Patients with Cardiovascular Disease" Journal of Clinical Medicine 13, no. 19: 5973. https://doi.org/10.3390/jcm13195973
APA StyleAdachi, T., Morishima, C., Nojiri, Y., Tsunekawa, Y., Tanimura, D., Sano, T., Shibata, K., & Kitamura, H. (2024). Reliability and Validity of the Rate of Force Development for Quadriceps in Older Patients with Cardiovascular Disease. Journal of Clinical Medicine, 13(19), 5973. https://doi.org/10.3390/jcm13195973