
The Effect of Sex on the Remimazolam Dosage Required for Successful i-gel Supraglottic Airway Insertion with Remifentanil in Non-Paralyzed Patients: An Up-and-Down Sequential Allocation Trial

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
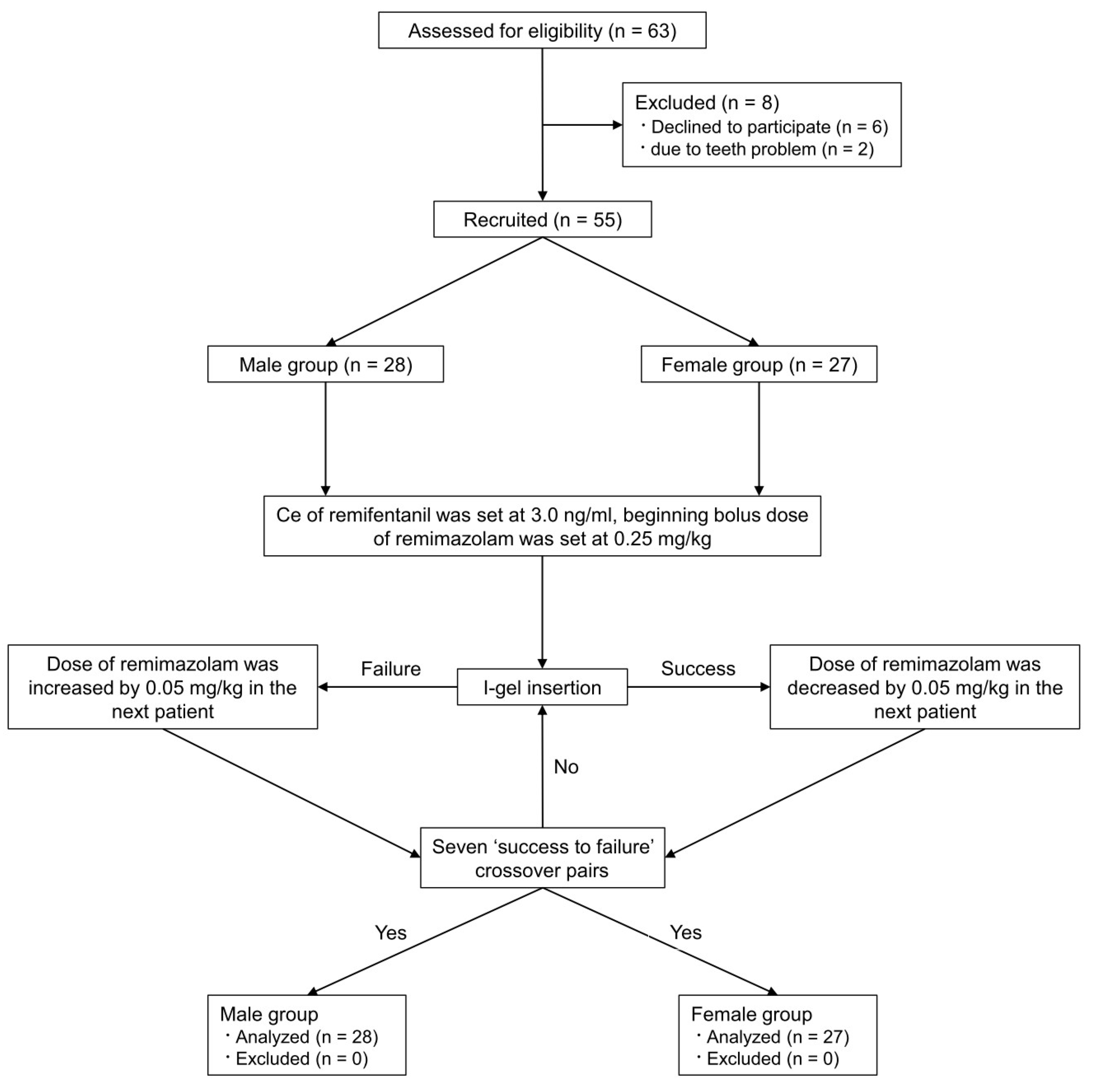
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kilpatrick, G.J. Remimazolam: Non-Clinical and Clinical Profile of a New Sedative/Anesthetic Agent. Front. Pharmacol. 2021, 12, 690875. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, Y. Efficacy and Safety Profile of Remimazolam for Sedation in Adults Undergoing Short Surgical Procedures. Ther. Clin. Risk Manag. 2022, 18, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.C.; Hung, K.C.; Illias, A.M.; Chiu, C.C.; Yu, C.H.; Lin, C.M.; Chen, I.W.; Sun, C.K. The use of remimazolam versus propofol for induction and maintenance of general anesthesia: A systematic review and meta-analysis. Front. Pharmacol. 2023, 14, 1101728. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Hu, P.; Jiang, J. Metabolite characterization of a novel sedative drug, remimazolam in human plasma and urine using ultra high-performance liquid chromatography coupled with synapt high-definition mass spectrometry. J. Pharm. Biomed. Anal. 2017, 137, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M. Remimazolam: Pharmacological characteristics and clinical applications in anesthesiology. Anesth. Pain Med. 2022, 17, 1–11. [Google Scholar] [CrossRef]
- Lohmer, L.L.; Schippers, F.; Petersen, K.U.; Stoehr, T.; Schmith, V.D. Time-to-Event Modeling for Remimazolam for the Indication of Induction and Maintenance of General Anesthesia. J. Clin. Pharmacol. 2020, 60, 505–514. [Google Scholar] [CrossRef]
- Oh, J.; Park, S.Y.; Lee, G.Y.; Park, J.H.; Joe, H.B. Effective dose of remimazolam co-administered with remifentanil to facilitate I-gel insertion without neuromuscular blocking agents: An up-and-down sequential allocation trial. BMC Anesthesiol. 2023, 23, 81. [Google Scholar] [CrossRef]
- Pleym, H.; Spigset, O.; Kharasch, E.D.; Dale, O. Gender differences in drug effects: Implications for anesthesiologists. Acta Anaesthesiol. Scand. 2003, 47, 241–259. [Google Scholar] [CrossRef]
- Choi, J.J.; Kim, J.Y.; Lee, D.; Chang, Y.J.; Cho, N.R.; Kwak, H.J. Male patients require higher optimal effect-site concentrations of propofol during i-gel insertion with dexmedetomidine 0.5 mug/kg. BMC Anesthesiol. 2016, 16, 20. [Google Scholar] [CrossRef]
- Kim, M.K.; Lee, J.W.; Jang, D.J.; Shin, O.Y.; Nam, S.B. Effect-site concentration of remifentanil for laryngeal mask airway insertion during target-controlled infusion of propofol. Anaesthesia 2009, 64, 136–140. [Google Scholar] [CrossRef]
- Schuttler, J.; Eisenried, A.; Lerch, M.; Fechner, J.; Jeleazcov, C.; Ihmsen, H. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: Part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology 2020, 132, 636–651. [Google Scholar] [CrossRef] [PubMed]
- Glass, P.S.; Bloom, M.; Kearse, L.; Rosow, C.; Sebel, P.; Manberg, P. Bispectral analysis measures sedation and memory effects of propofol, midazolam, isoflurane, and alfentanil in healthy volunteers. Anesthesiology 1997, 86, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Drage, M.; Nunez, J.; Vaughan, R.; Asai, T. Jaw thrusting as a clinical test to assess the adequate depth of anaesthesia for insertion of the laryngeal mask. Anaesthesia 1996, 51, 1167–1170. [Google Scholar] [CrossRef] [PubMed]
- Krzych, Ł.J.; Pluta, M.P.; Putowski, Z.; Czok, M. Investigating Association between Intraoperative Hypotension and Postoperative Neurocognitive Disorders in Non-Cardiac Surgery: A Comprehensive Review. J. Clin. Med. 2020, 9, 3183. [Google Scholar] [CrossRef] [PubMed]
- Dixon, W.J. Staircase bioassay: The up-and-down method. Neurosci. Biobehav. Rev. 1991, 15, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Choi, S.C. Sequential method of estimating the LD50 using a modified up-and-down rule. J. Biopharm. Stat. 1994, 4, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Gorges, M.; Zhou, G.; Brant, R.; Ansermino, J.M. Sequential allocation trial design in anesthesia: An introduction to methods, modeling, and clinical applications. Paediatr. Anaesth. 2017, 27, 240–247. [Google Scholar] [CrossRef]
- Dilleen, M.; Heimann, G.; Hirsch, I. Non-parametric estimators of a monotonic dose-response curve and bootstrap confidence intervals. Stat. Med. 2003, 22, 869–882. [Google Scholar] [CrossRef]
- Payton, M.E.; Greenstone, M.H.; Schenker, N. Overlapping confidence intervals or standard error intervals: What do they mean in terms of statistical significance? J. Insect Sci. 2003, 3, 34. [Google Scholar] [CrossRef]
- Polverino, M.; Polverino, F.; Fasolino, M.; Ando, F.; Alfieri, A.; De Blasio, F. Anatomy and neuro-pathophysiology of the cough reflex arc. Multidiscip. Respir. Med. 2012, 7, 5. [Google Scholar] [CrossRef]
- Canning, B.J. Anatomy and neurophysiology of the cough reflex: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 33S–47S. [Google Scholar] [CrossRef] [PubMed]
- Spina, D.; McFadzean, I.; Bertram, F.; Page, C. Peripheral mechanisms II: The pharmacology of peripherally active antitussive drugs. Pharmacol. Ther. Cough 2009, 187, 155–186. [Google Scholar]
- Soh, S.; Park, W.K.; Kang, S.W.; Lee, B.R.; Lee, J.R. Sex differences in remifentanil requirements for preventing cough during anesthetic emergence. Yonsei Med. J. 2014, 55, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Joe, H.B.; Kim, J.Y.; Kwak, H.J.; Oh, S.E.; Lee, S.Y.; Park, S.Y. Effect of sex differences in remifentanil requirements for the insertion of a laryngeal mask airway during propofol anesthesia: A prospective randomized trial. Medicine 2016, 95, e5032. [Google Scholar] [CrossRef]
- Minto, C.F.; Schnider, T.W.; Egan, T.D.; Youngs, E.; Lemmens, H.J.; Gambus, P.L.; Billard, V.; Hoke, J.F.; Moore, K.H.; Hermann, D.J.; et al. Influence of age and gender on the pharmacokinetics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology 1997, 86, 10–23. [Google Scholar] [CrossRef]
- Buchanan, F.F.; Myles, P.S.; Cicuttini, F. Patient sex and its influence on general anaesthesia. Anaesth. Intensive Care 2009, 37, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Leonowens, C.; Ivaturi, V.D.; Lohmer, L.L.; Curd, L.; Ossig, J.; Schippers, F.; Petersen, K.U.; Stoehr, T.; Schmith, V. Population pharmacokinetic/pharmacodynamic modeling for remimazolam in the induction and maintenance of general anesthesia in healthy subjects and in surgical subjects. J. Clin. Anesth. 2020, 66, 109899. [Google Scholar] [CrossRef] [PubMed]
- Wiltshire, H.R.; Kilpatrick, G.J.; Tilbrook, G.S.; Borkett, K.M. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): Part II. Population pharmacokinetic and pharmacodynamic modeling and simulation. Anesth. Analg. 2012, 115, 284–296. [Google Scholar] [CrossRef]
- Zhou, Y.; Zhang, L.; Cao, L.; Chen, M.; Zhang, W. Effect of gender factor on potency of remimazolam inhibiting responses to laryngeal mask airway insertion. Chin. J. Anesthesiol. 2021, 95, 1109–1111. [Google Scholar]
- Lenzmeier, B.; Moore, R.L.; Cordts, P.; Garrett, N. Menstrual cycle-related variations in postoperative analgesia with the preemptive use of N-methyl D-aspartate antagonist ketamine: A pilot study. Dimens. Crit. Care Nurs. 2008, 27, 271–276. [Google Scholar] [CrossRef]
- Erden, V.; Yangn, Z.; Erkalp, K.; Delatioglu, H.; Bahceci, F.; Seyhan, A. Increased progesterone production during the luteal phase of menstruation may decrease anesthetic requirement. Anesth. Analg. 2005, 101, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Fu, F.; Chen, X.; Feng, Y.; Shen, Y.; Feng, Z.; Bein, B. Propofol EC50 for inducing loss of consciousness is lower in the luteal phase of the menstrual cycle. Br. J. Anaesth. 2014, 112, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Leslie, K.; Sessler, D.I.; Schroeder, M.; Walters, K. Propofol blood concentration and the Bispectral Index predict suppression of learning during propofol/epidural anesthesia in volunteers. Anesth. Analg. 1995, 81, 1269–1274. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Singh, H.; White, P.F. Electroencephalogram bispectral analysis predicts the depth of midazolam-induced sedation. Anesthesiology 1996, 84, 64–69. [Google Scholar] [CrossRef] [PubMed]
- McKay, I.D.; Voss, L.J.; Sleigh, J.W.; Barnard, J.P.; Johannsen, E.K. Pharmacokinetic-pharmacodynamic modeling the hypnotic effect of sevoflurane using the spectral entropy of the electroencephalogram. Anesth. Analg. 2006, 102, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and safety of remimazolam versus propofol for general anesthesia: A multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J. Anesth. 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Wei, A.; Ma, S.; Dou, Y.; Wang, X.; Wu, J.; Zhou, S.; Deng, Y.; Liu, X.; Li, D.; Yang, M. The safety and efficacy of remimazolam tosylate combined with propofol in upper gastrointestinal endoscopy: A multicenter, randomized clinical trial. PLoS ONE 2023, 18, e0282930. [Google Scholar] [CrossRef]
- Stasiowski, M.J.; Dulawa, A.; Krol, S.; Marciniak, R.; Kaspera, W.; Niewiadomska, E.; Krawczyk, L.; Ladzinski, P.; Grabarek, B.O.; Jalowiecki, P. Polyspikes and Rhythmic Polyspikes During Volatile Induction of General Anesthesia With Sevoflurane Result in Bispectral Index Variations. Clin. EEG Neurosci. 2023, 54, 289–304. [Google Scholar] [CrossRef]
- Choi, B.M.; Lee, J.S.; Kim, K.M.; Bang, J.Y.; Lee, E.K.; Noh, G.J. Frequency and characteristics of patients with bispectral index values of 60 or higher during the induction and maintenance of general anesthesia with remimazolam. Sci. Rep. 2023, 13, 9992. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Parameters | Men (n = 28) | Women (n = 27) | p Value |
|---|---|---|---|
| Age (years) | 41.5 (29.5, 49.0) | 50.0 (35.5, 54.0) | 0.206 |
| Weight (kg) | 77.2 ± 9.6 | 61.5 ± 6.9 | <0.001 |
| Height (cm) | 173.9 ± 6.9 | 159.1 ± 5.5 | <0.001 |
| BMI (kg/m2) | 25.9 (24.0, 27.1) | 24.6 (22.3, 26.1) | 0.072 |
| ASA PS class | 0.701 | ||
| I | 21 (75.0) | 18 (66.7) | |
| II | 7 (25.0) | 9 (33.3) |
| Parameters | Men (n = 28) | Women (n = 27) | p Value |
|---|---|---|---|
| Modified Dixon’s up-and-down method | |||
| ED50, mg/kg | 0.28 ± 0.02 | 0.18 ± 0.02 | <0.001 |
| Isotonic regression method | |||
| ED50 (83% CI), mg/kg | 0.30 (0.27–0.32) * | 0.20 (0.15–0.23) | |
| ED95 (95% CI), mg/kg | 0.35 (0.34–0.35) * | 0.29 (0.25–0.30) |
| Time | Men (n = 14) | Women (n = 14) | p Value |
|---|---|---|---|
| Mean arterial pressure | |||
| T0 | 101.00 ± 11.86 | 108.07 ± 17.80 | 0.227 |
| T1 | 90.43 ± 15.85 * | 88.79 ± 13.27 * | 0.769 |
| T2 | 85.50 ± 12.79 * | 82.21 ± 14.12 * | 0.524 |
| T3 | 83.14 ± 12.11 * | 79.71 ± 12.65 * | 0.470 |
| T4 | 80.64 ± 12.04 * | 79.36 ± 11.56 * | 0.775 |
| T5 | 85.07 ± 12.90 * | 82.29 ± 13.60 * | 0.583 |
| T6 | 86.93 ± 15.15 * | 88.00 ± 15.70 * | 0.856 |
| Heart rate | |||
| T0 | 68.93 ± 13.20 | 68.64 ± 10.95 | 0.951 |
| T1 | 75.14 ± 14.39 * | 68.79 ± 9.24 | 0.176 |
| T2 | 73.43 ± 10.39 | 63.43 ± 9.40 * | 0.013 |
| T3 | 72.64 ± 10.72 | 62.29 ± 9.86 * | 0.013 |
| T4 | 75.50 ± 11.59 * | 63.36 ± 10.80 * | 0.008 |
| T5 | 78.07 ± 10.09 * | 67.50 ± 9.04 | 0.007 |
| T6 | 77.57 ± 9.58 * | 68.79 ± 10.21 | 0.027 |
| Bispectral index | |||
| T0 | 96.86 ± 1.29 | 94.14 ± 3.46 | 0.011 |
| T1 | 61.79 ± 9.46 * | 61.36 ± 12.29 * | 0.918 |
| T2 | 60.64 ± 6.42 * | 64.07 ± 10.58 * | 0.309 |
| T3 | 58.50 ± 5.60 * | 63.21 ± 8.61 * | 0.098 |
| T4 | 56.86 ± 4.66 * | 64.50 ± 8.77 * | 0.008 |
| T5 | 58.36 ± 4.65 * | 65.57 ± 7.67 * | 0.006 |
| T6 | 56.71 ± 5.54 * | 61.86 ± 7.85 * | 0.056 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.-Y.; Park, S.-Y.; Moon, J.-Y.; Park, J.-H.; Joe, H.-B. The Effect of Sex on the Remimazolam Dosage Required for Successful i-gel Supraglottic Airway Insertion with Remifentanil in Non-Paralyzed Patients: An Up-and-Down Sequential Allocation Trial. J. Clin. Med. 2024, 13, 670. https://doi.org/10.3390/jcm13030670
Oh J-Y, Park S-Y, Moon J-Y, Park J-H, Joe H-B. The Effect of Sex on the Remimazolam Dosage Required for Successful i-gel Supraglottic Airway Insertion with Remifentanil in Non-Paralyzed Patients: An Up-and-Down Sequential Allocation Trial. Journal of Clinical Medicine. 2024; 13(3):670. https://doi.org/10.3390/jcm13030670
Chicago/Turabian StyleOh, Ju-Yeon, Sung-Yong Park, Jung-Yoon Moon, Ji-Hyun Park, and Han-Bum Joe. 2024. "The Effect of Sex on the Remimazolam Dosage Required for Successful i-gel Supraglottic Airway Insertion with Remifentanil in Non-Paralyzed Patients: An Up-and-Down Sequential Allocation Trial" Journal of Clinical Medicine 13, no. 3: 670. https://doi.org/10.3390/jcm13030670