
Antibodies against Small Ubiquitin-like Modifier Activating Enzyme May Be a Protective Factor from Rapid Progressive Interstitial Lung Disease in Patients Bearing Antibodies against Melanoma Differentiation Associated Gene 5

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Statistical Analyses
3. Results
3.1. Clinical and Laboratory Features of Anti-MDA5+-Patients
3.2. Basic Laboratory Data, Anti-SAE Antibodies, Anti-Ro52 Antibodies and the Mortality
3.3. Subgroup Analysis: Stratification by the Positivity of Anti-SAE Antibodies
3.4. Subgroup Analysis: Stratification by Diagnosis of DM or Not
3.5. Kaplan–Meier Survival Analysis of the Parent Anti-MDA5 Cohort, Anti-SAE+ and Anti-Ro52+ Groups
3.6. Univariate and Multivariate Logistic Regression Analyses for Risk Factors of RPILD in Anti-MDA5+ Patients
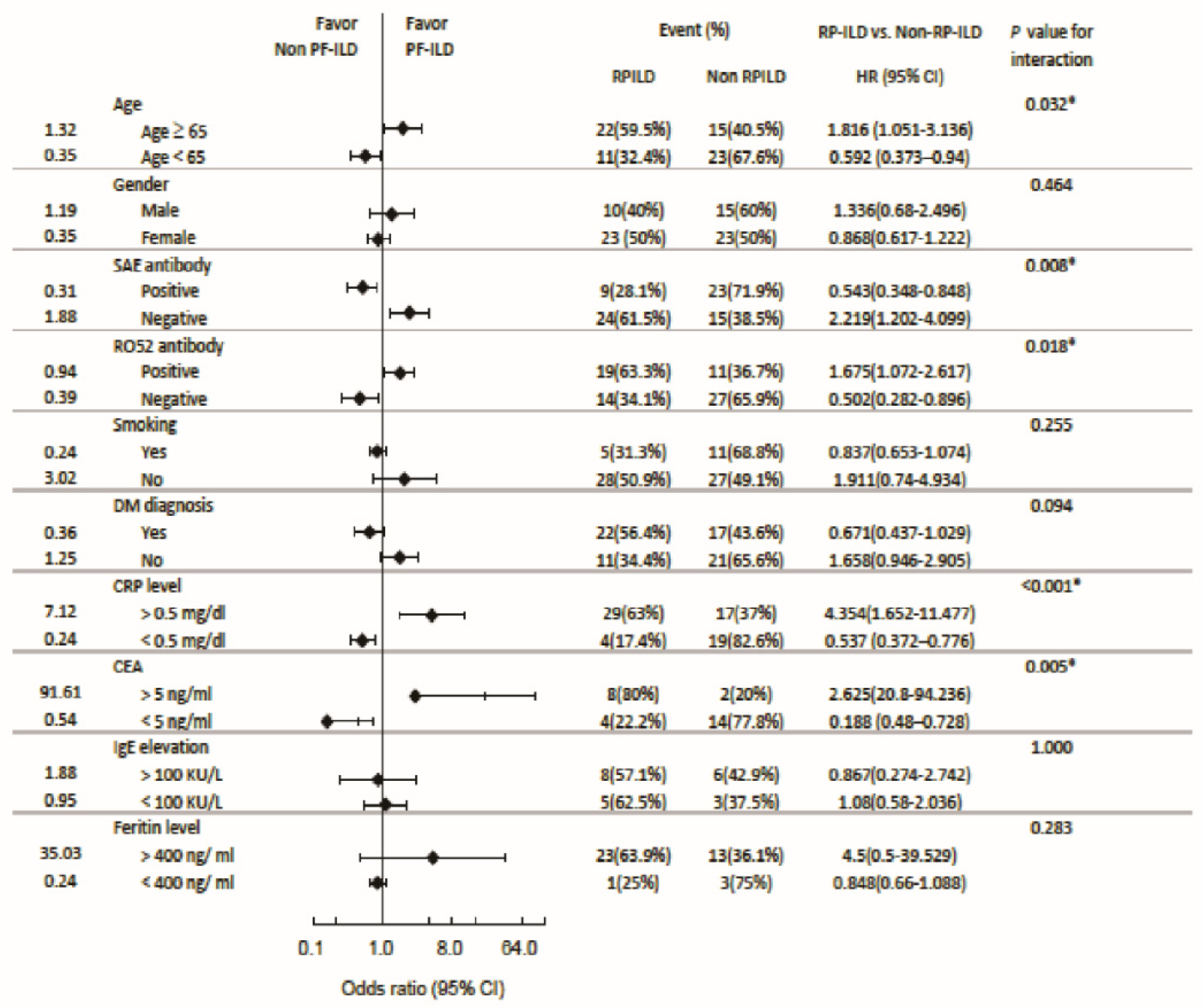
3.7. Subgroup Analysis: Odds Ratio for RPILD and Mortality
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tang, K.; Zhang, H.; Jin, H. Clinical characteristics and management of patients with clinical amyopathic dermatomyositis: A retrospective study of 64 patients at a tertiary dermatology department. Front. Med. 2021, 8, 783416. [Google Scholar] [CrossRef]
- Cao, H.; Pan, M.; Kang, Y.; Xia, Q.; Li, X.; Zhao, X.; Shi, R.; Lou, J.; Zhou, M.; Kuwana, M.; et al. Clinical manifestations of dermatomyositis and clinically amyopathic dermatomyositis patients with positive expression of anti-melanoma differentiation-associated gene 5 antibody. Arthritis Care Res. 2012, 64, 1602–1610. [Google Scholar] [CrossRef]
- Chen, Z.; Cao, M.; Plana, M.N.; Liang, J.; Cai, H.; Kuwana, M.; Sun, L. Utility of anti-melanoma differentiation-associated gene 5 antibody measurement in identifying patients with dermatomyositis and a high risk for developing rapidly progressive interstitial lung disease: A review of the literature and a meta-analysis. Arthritis Care Res. 2013, 65, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Koga, T.; Fujikawa, K.; Horai, Y.; Okada, A.; Kawashiri, S.-Y.; Iwamoto, N.; Suzuki, T.; Nakashima, Y.; Tamai, M.; Arima, K.; et al. The diagnostic utility of anti-melanoma differentiation-associated gene 5 antibody testing for predicting the prognosis of Japanese patients with DM. Rheumatology 2012, 51, 1278–1284. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Kuwana, M. Clinically amyopathic dermatomyositis. Curr. Opin. Rheumatol. 2010, 22, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Moghadam-Kia, S.; Oddis, C.V.; Sato, S.; Kuwana, M.; Aggarwal, R. Antimelanoma differentiation-associated gene 5 antibody: Expanding the clinical spectrum in north American patients with dermatomyositis. J. Rheumatol. 2017, 44, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Vinik, O.; Shojania, K.; Yeung, J.; Shupak, R.; Nimmo, M.; Avina-Zubieta, J.A. Clinical spectrum and therapeutics in Canadian patients with anti-melanoma differentiation-associated gene 5 (MDA5)-positive dermatomyositis: A case-based review. Rheumatol. Int. 2019, 39, 1971–1981. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Li, W.; Xie, Q.; Yin, G. Rituximab in the treatment of interstitial lung diseases related to anti-melanoma differentiation-associated gene 5 dermatomyositis: A systematic review. Front. Immunol. 2022, 12, 820163. [Google Scholar] [CrossRef] [PubMed]
- Ye, S.; Chen, X.-x.; Lu, X.-y.; Wu, M.-f.; Deng, Y.; Huang, W.-q.; Guo, Q.; Yang, C.-d.; Gu, Y.-y.; Bao, C.-d.; et al. Adult clinically amyopathic dermatomyositis with rapid progressive interstitial lung disease: A retrospective cohort study. Clin. Rheumatol. 2007, 26, 1647–1654. [Google Scholar] [CrossRef]
- Li, Y.; Gao, X.; Li, Y.; Jia, X.; Zhang, X.; Xu, Y.; Gan, Y.; Li, S.; Chen, R.; He, J.; et al. Predictors and mortality of rapidly progressive interstitial lung disease in patients with idiopathic inflammatory myopathy: A series of 474 patients. Front. Med. 2020, 7, 363. [Google Scholar] [CrossRef]
- Shirakashi, M.; Nakashima, R.; Tsuji, H.; Tanizawa, K.; Handa, T.; Hosono, Y.; Akizuki, S.; Murakami, K.; Hashimoto, M.; Yoshifuji, H.; et al. Efficacy of plasma exchange in anti-MDA5-positive dermatomyositis with interstitial lung disease under combined immunosuppressive treatment. Rheumatology 2020, 59, 3284–3292. [Google Scholar] [CrossRef]
- Kato, H.; Takeuchi, O.; Sato, S.; Yoneyama, M.; Yamamoto, M.; Matsui, K.; Uematsu, S.; Jung, A.; Kawai, T.; Ishii, K.J.; et al. Differential roles of MDA5 and RIG-I helicases in the recognition of RNA viruses. Nature 2006, 441, 101–105. [Google Scholar] [CrossRef]
- Miner, J.J.; Diamond, M.S. MDA5 and autoimmune disease. Nat. Genet. 2014, 46, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Nishina, N.; Sato, S.; Masui, K.; Gono, T.; Kuwana, M. Seasonal and residential clustering at disease onset of anti-MDA5-associated interstitial lung disease. RMD Open 2020, 6, e001202. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Richeldi, L.; Thomson, C.C.; Inoue, Y.; Johkoh, T.; Kreuter, M.; Lynch, D.A.; Maher, T.M.; Martinez, F.J.; et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: An official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2022, 205, e18–e47. [Google Scholar] [CrossRef] [PubMed]
- Tzilas, V.; Tzouvelekis, A.; Ryu, J.H.; Bouros, D. 2022 update on clinical practice guidelines for idiopathic pulmonary fibrosis and progressive pulmonary fibrosis. Lancet Respir. Med. 2022, 10, 729–731. [Google Scholar] [CrossRef]
- Tarricone, E.; Ghirardello, A.; Rampudda, M.; Bassi, N.; Punzi, L.; Doria, A. Anti-SAE antibodies in autoimmune myositis: Identification by unlabelled protein immunoprecipitation in an Italian patient cohort. J. Immunol. Methods 2012, 384, 128–134. [Google Scholar] [CrossRef]
- Ge, Y.; Lu, X.; Shu, X.; Peng, Q.; Wang, G. Clinical characteristics of anti-SAE antibodies in Chinese patients with dermatomyositis in comparison with different patient cohorts. Sci. Rep. 2017, 7, 188. [Google Scholar] [CrossRef] [PubMed]
- So, H.; So, J.; Lam, T.T.-O.; Wong, V.T.-L.; Ho, R.; Li, W.L.; Mok, C.C.; Lau, C.S.; Tam, L.-S. Performance of the 2017 European Alliance of Associations for Rheumatology/American College of Rheumatology classification criteria in patients with idiopathic inflammatory myopathy and anti–melanoma differentiation–associated protein 5 positivity. Arthritis Rheumatol. 2022, 74, 1588–1592. [Google Scholar] [CrossRef] [PubMed]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 1975, 292, 344–347. [Google Scholar] [CrossRef]
- Bohan, A.; Peter, J.B. Polymyositis and dermatomyositis (second of two parts). N. Engl. J. Med. 1975, 292, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, I.E.; Tjärnlund, A.; Bottai, M.; Werth, V.P.; Pilkington, C.; de Visser, M.; Alfredsson, L.; Amato, A.A.; Barohn, R.J.; Liang, M.H.; et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and jvenile idiopathic inflammatory myopathies and their major subgroups. Ann. Rheum. Dis. 2017, 76, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Takezaki, S.; Kobayashi, I.; Iwata, N.; Mori, M.; Nagai, K.; Nakano, N.; Miyoshi, M.; Kinjo, N.; Murata, T.; et al. Clinical and laboratory features of fatal rapidly progressive interstitial lung disease associated with juvenile dermatomyositis. Rheumatology 2015, 54, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Graney, B.A.; Fischer, A. Interstitial pneumonia with autoimmune features. Ann. Am. Thorac. Soc. 2019, 16, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Guo, L.; Fu, Y.; Wang, K.; Zhang, D.; Xu, W.; Chen, Z.; Ye, S. Interstitial lung disease in anti-MDA5 positive dermatomyositis. Clin. Rev. Allergy Immunol. 2021, 60, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, H.; Nakashima, R.; Hosono, Y.; Imura, Y.; Yagita, M.; Yoshifuji, H.; Hirata, S.; Nojima, T.; Sugiyama, E.; Hatta, K.; et al. Multicenter prospective study of the efficacy and safety of combined immunosuppressive therapy with high-dose glucocorticoid, tacrolimus, and cyclophosphamide in interstitial lung diseases accompanied by anti-melanoma differentiation-associated gene 5-positive dermatomyositis. Arthritis Rheumatol. 2020, 72, 488–498. [Google Scholar] [PubMed]
- So, H.; Wong, V.T.L.; Lao, V.W.N.; Pang, H.T.; Yip, R.M.L. Rituximab for refractory rapidly progressive interstitial lung disease related to anti-MDA5 antibody-positive amyopathic dermatomyositis. Clin. Rheumatol. 2018, 37, 1983–1989. [Google Scholar] [CrossRef]
- Kurasawa, K.; Arai, S.; Namiki, Y.; Tanaka, A.; Takamura, Y.; Owada, T.; Arima, M.; Maezawa, R. Tofacitinib for refractory interstitial lung diseases in anti-melanoma differentiation-associated 5 gene antibody-positive dermatomyositis. Rheumatology 2018, 57, 2114–2119. [Google Scholar] [CrossRef]
- McPherson, M.; Economidou, S.; Liampas, A.; Zis, P.; Parperis, K. Management of MDA-5 antibody positive clinically amyo9athic dermatomyositis associated interstitial lung disease: A systematic review. Semin. Arthritis Rheum. 2022, 53, 151959. [Google Scholar] [CrossRef]
- You, H.; Wang, L.; Wang, J.; Lv, C.; Xu, L.; Yuan, F.; Li, J.; Wu, M.; Zhou, S.; Da, Z.; et al. Time-dependent changes in RPILD and mortality risk in anti-MDA5+ DM patients: A cohort study of 272 cases in China. Rheumatology 2023, 62, 1216–1226. [Google Scholar] [CrossRef]
- Zhu, D.; Qiao, J.; Tang, S.; Pan, Y.; Li, S.; Yang, C.; Fang, H. Elevated carcinoembryonic antigen predicts rapidly progressive interstitial lung disease in clinically amyopathic dermatomyositis. Rheumatology 2021, 60, 3896–3903. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Ye, L.; Chen, F.; Shen, Y.; Lu, X.; Wang, G.; Shu, X. Different multivariable risk factors for rapid progressive interstitial lung disease in anti-MDA5 positive dermatomyositis and anti-synthetase syndrome. Front. Immunol. 2022, 13, 845988. [Google Scholar] [CrossRef] [PubMed]
- So, J.; So, H.; Wong, V.T.-L.; Ho, R.; Wu, T.Y.; Wong, P.C.-H.; Tam, L.H.-P.; Ho, C.; Lam, T.T.-O.; Chung, Y.K.; et al. Predictors of rapidly progressive interstitial lung disease and mortality in patients with autoantibodies against melanoma differentiation-associated protein 5 dermatomyositis. Rheumatology 2022, 61, 4437–4444. [Google Scholar] [CrossRef]
- Peterson, L.K.; Jaskowski, T.D.; La’Ulu, S.L.; Tebo, A.E. Antibodies to small ubiquitin-like modifier activating enzyme are associated with a diagnosis of dermatomyositis: Results from an unselected cohort. Immunol. Res. 2018, 66, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Bodoki, L.; Nagy-Vincze, M.; Griger, Z.; Betteridge, Z.; Szöllősi, L.; Dankó, K. Four dermatomyositis-specific autoantibodies-anti-TIF1γ, anti-NXP2, anti-SAE and anti-MDA5-in adult and juvenile patients with idiopathic inflammatory myopathies in a Hungarian cohort. Autoimmun. Rev. 2014, 13, 1211–1219. [Google Scholar] [CrossRef]
- Muro, Y.; Sugiura, K.; Akiyama, M. Low prevalence of anti-small ubiquitin-like modifier activating enzyme antibodies in dermatomyositis patients. Autoimmunity 2013, 46, 279–284. [Google Scholar] [CrossRef]
- 37 Shao, C.; Sun, Y.; Huang, H.; Zhang, Z.; Pan, R.; Xu, K.; Zhang, X.; Zhang, Y.; Xu, Z. Myositis specific antibodies are associated with isolated anti-Ro-52 associated interstitial lung disease. Rheumatology 2022, 61, 1083–1091. [Google Scholar] [CrossRef]
- Cavagna, L.; Meloni, F.; Meyer, A.; Sambataro, G.; Belliato, M.; de Langhe, E.; Cavazzana, I.; Pipitone, N.; Triantafyllias, K.L.; Mosca, M.; et al. Clinical spectrum time course in non-Asian patients positive for anti-MDA5 antibodies. Clin. Exp. Rheumatol. 2022, 40, 274–283. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients (n = 71) | RPILD * (n = 33) | Non RPILD (n = 38) | Concurrent Anti-SAE Abs (n = 32) | Concurrent Anti-Ro52 Abs (n = 30) | Mortality (n = 17) | |
|---|---|---|---|---|---|---|
| Male (%) | 25 (35.2%) | 10 (30.3%) | 15 (39.5%) | 14 (43.8%) | 6 (20%) | 6 (35.3%) |
| Female (%) | 46 (64.8%) | 23 (69.7%) | 23 (60.5%) | 18 (56.3%) | 24 (80%) | 11 (64.7%) |
| Mean age (S.D. **) | 63.4 (13.9) | 65.5 (11.1) (p = 0.239) | 61.6 (15.8) (p = 0.238) | 64.5 (14.2) (p = 0.546) | 60.9 (13.5) (p = 0.192) | 67.1 (9.4) (p = 0.21) |
| DM/PM (%) | 39 (55%) | 22 (56.4%) | 17 (43.6%) | 8 (25%) | 22 (73.3%) | 14 (82.4%) |
| AST (S.D.**) U/L | 79.8 (105.9) | 97.9 (126.5) | 63.6 (82.0) | 61.0 (89.5) (p = 0.194) | 106.1 (132.5) (p = 0.086) | 107.9 (82.8) (p = 0.209) |
| LDH (S.D. **) U/L | 411.8 (179.7) | 427.5 (205.7) | 397.0 (152.9) | 360.8 (127.3) (p = 0.043) | 448.1 (218.7) (p = 0.139) | 508.3 (237.5) (p = 0.009) |
| CK (S.D. **), U/L | 928.1 (2318.8) | 504.2 (847.4) | 1279.3 (3015.2) | 832.4 (2931.7) (p = 0.926) | 959.3 (1732.9) (p = 0.059) | 629.8 (1084.8) (p = 0.234) |
| Myoglobulin (S.D. **), ng/mL | 574.5 (851.6) | 548.1 (819.1) | 606.8 (938. 9) | 157.6 (122.4) (p = 0.11) | 582.4 (854.6) (p = 0.968) | 448.3 (693.6) (p = 0.602) |
| CRP (S.D.**) mg/dL | 4.17 (6.80) | 6.03 (8.18) | 2.46 (4.74) | 4.25 (6.18) (p = 0.937) | 3.36 (6.56) (p = 0.405) | 8.78 (8.97) (p = 0.001) |
| ESR (S.D.**) mm/h | 50.0 (35.9) | 56.2 (36.6) | 44.5 (34.9) | 47.5 (35.3) (p = 0.634) | 50.4 (32.8) (p = 0.94) | 61.3 (34.4) (p = 0.18) |
| Albumin (S.D. **), g/dL | 3.32 (0.79) | 3.11 (0.82) | 3.56 (0.69) | 3.57 (0.84) (p = 0.037) | 3.10 (0.74) (p = 0.098) | 2.58 (0.43) (p = <0.001) |
| CA-153(S.D. **), U/mL | 19.9 (17.8) | 32.9 (18.8) | 10.1 (9.2) | 10.5 (10.5) (p = 0.087) | 26.1 (7.8) (p = 0.517) | 29.0 (12.8) (p = 0.339) |
| CEA (S.D. **), ng/mL | 7.8 (7.4) | 12.5 (8.4) | 4.2 (3.9) | 6.9 (6.7) (p = 0.569) | 11.0 (9.8) (p = 0.239) | 15.2 (8.6) (p = 0.001) |
| IgE (S.D. **), KU/L | 260.7 (306.8) | 310.9 (378.1) | 188.1 (150.3) | 298.1 (402.8) (p = 0.58) | 155.1 (215.9) (p = 0.335) | 392.0 (491.9) (p = 0.176) |
| Ferritin (S.D. **) ng/mL | 1722.2 (1920.2) | 2449.8 (2152.8) | 630.8 (602.0) | 1063.3 (1338.1) (p = 0.076) | 2245.4 (1982.7) (p = 0.120) | 3178.2 (2147.4) (p < 0.001) |
| Smoking (%) | 16 (22.5%) | 5 (15.2%) | 11 (28.9%) | 9 (56.3%) | 4 (25%) | 2 (11.8%) |
| Malignancy (%) | 15 (21.1%) | 11 (73.3%) | 4 (26.7%) | 5 (33.3%) | 2 (13.3%) | 6 (35.3%) |
| Other CTD *** (%) | 27 (38%) | 10 (41.7%) | 14 (58.3%) | 13 (54.2%) | 13 (54.2%) | 2 (11.8%) |
| Anti-SAE antibody (%) | 32 (45.1%) | 9 (28.1%) | 23 (71.9%) | 5 (15.6%) | 3 (17.6%) | |
| Anti-Ro52 antibody (%) | 30 (42.3%) | 19 (63.3%) | 11 (36.7%) | 5 (15.6%) | 11 (64.7%) | |
| Mortality (%) | 17 (23.9%) | 17 (100%) | 0 (0) | 3 (17.6%) | 11 (64.7%) |
| Anti-SAE-Positive (N = 32) | Anti-SAE-Negative (N = 39) | |||||||
|---|---|---|---|---|---|---|---|---|
| RP-ILD (N = 9, 28.1%) | Non-RP-ILD (N = 23, 71.9%) | p-Value | OR *** (C.I.#) | RP-ILD (N = 23, 59%) | Non-RP-ILD (N = 16, 41%) | p-Value | OR *** (C.I. #) | |
| LDH (S.D. **) U/L | 376.22 (112.3) | 353.9 (135.6) | 0.670 | 0.441 (p = 0.442, 0.057–3.421) | 456.43 (230.4) | 439.94 (165.1) | 0.807 | 3.385 (p = 0.55, 0.279–41.087) |
| CRP (S.D. **) mg/dL | 8.23 (8.9) | 2.547 (3.7) | 0.018 * | 2.667 (p = 0.427, 0.521–13.655) | 5.40 (8.04) | 2.26 (5.9) | 0.192 | 17.111 (p = 0.04, 1.832–159.802 *) |
| Albumin (S.D. **), g/dL | 3.31 (1.1) | 3.67 (0.75) | 0.358 | 1.905 (p = 0.659, 0.321–11.312) | 3.05 (0.8) | 3.33 (0.5) | 0.352 | 1.583 (p = 0.634, 0.23–10.904) |
| CEA (S.D. **), ng/mL | 11.45 (9.6) | 5.15 (4.7) | 0.116 | 3 (p = 0.505, 0.14–64.262) | 13.02 (8.4) | 2.67 (1.6) | 0.012 * | 35 (p = 0.026, 1.743–702.993 *) |
| Ferritin (S.D. **) ng/mL | 2581.25 (2103.6) | 557.32 (343.2) | 0.004 * | 0.597 (p = 1.00, 0.773–1.087) | 2423.49 (2215.2) | 851.15 (1137.4) | 0.186 | 19 (p = 0.032, 1.146–314.971*) |
| CK (S.D. **), U/L | 157.29 (99.6) | 1068.7 (3395.8) | 0.49 | 0.489 (p = 0.662, 0.76–3.145) | 620.86 (972.5) | 1492.6 (2436.2) | 0.144 | 0.791 (p = 0.749, 0.211–2.972) |
| AST (S.D. **) U/L | 48.38 (38.1) | 65.86 (103.1) | 0.647 | 1.067 (p = 0.647, 0.161–7.056) | 118.43 (143.2) | 58.19 (38.8) | 0.111 | 2.411 (p = 0.209, 0.652–8.92) |
| Myoglobulin (S.D. **), ng/mL | 92.5 (130.8) | 183.68 (123.4) | 0.423 | 0.25 (p = 0.524, 0.07–8.56) | 6 (66.7%) | 3 (33.3%) | 0.439 | 0.667 (p = 0.646, 0.047–9.472) |
| ESR (S.D. **) mm/h | 48.14 (29.8) | 47.3 (37.8) | 0.958 | 1.333 (p = 0.546, 0.235–7.556) | 58.25 (39.8) | 42.38 (30.4) | 0.231 | 1.333 (p = 0.465, 0.235–7.556) |
| IgE (S.D. **) KU/L | 468.96 (567.1) | 155.72 (117.2) | 0.215 | 0.75 (p = 0.652, 0.064–8.834) | 212.1 (179.7) | 252.91 (215.8) | 0.756 | 0.75 (p = 0.721, 0.064–8.834) |
| anti-Ro52 antibodies (+) | 2 (22.2%) | 7 (77.8%) | - | 0.653 (p = 0.501, 0.107–3.971) | 2 (22.2%) | 7 (77.8%) | - | 0.653 (p = 0.179, 0.107–3.971) |
| Smoking | 2 (22.2%) | 7 (77.8%) | - | 0.653 (p = 0.501, 0.107–3.971) | 2 (22.2%) | 7 (77.8%) | - | 0.653 (p = 0.415, 0.107–3.971) |
| Anti-SAE-Positive Anti-SAE-Negative | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mortality (N = 3, 9.4%) | Non-Mortality (N = 29, 90.6%) | p-Value | LR (C.I.) | Mortality (N = 14, 35.9%) | Non-Mortality (N = 25, 64.1%) | p-Value | LR (C.I.) | |
| RPILD | 3 (33.3%) | 6(66.7%) | - | 8.455 (p = 0.004 * 0.101–0.422) | 14 (60.9%) | 9 (39.1%) | - | 20.131 (p < 0.001, 0.213–0.607 *) |
| LDH (S.D. **) U/L | 392.67 (183.8) | 19 (86.4%) | 0.656 | 1.311 (p = 0.252 0.645–0.972) | 402.92 (245.9) | 402.92 (163.4) | 0.054 | 2.906 (p = 0.088, 0.752–1.018) |
| CRP (S.D. **) mg/dL | 11.68 (7.4) | 3.42 (5.6) | 0.025 * | 4.493 (p = 0.034 * 0.292–0.678) | 8.16 (9.4) | 1.84 (4.7) | 0.008 * | 8.236 (p = 0.04, 0.52–0.89 *) |
| Albumin (S.D. **) g/dL | 2.4 (0.529) | 3.73 (0.8) | 0.007 * | 5.194 (p = 0.023 * 0.221–0.657) | 2.62 (0.4) | 3.54 (0.6) | 0.000 * | 8.388 (p = 0.004*, 0.455–0.919) |
| CEA (S.D. **) ng/mL | 11.95 (12.4) | 6.12 (5.8) | 0.272 | 1.827 (p = 0.177 0.351–345.1) | 16.5 (8.2) | 4.19 (4) | 0.002 * | 7.664 (p = 0.06 *, 0.132–0.84) |
| Ferritin (S.D. **) ng/mL | 3038.33 (2320.3) | 607.53 (375.1) | 0.001 * | 0.43 (p = 0.512 0.789–1.08) | 3208.14 (2200.4) | 696.04 (789) | 0.002 * | 5.868 (p = 0.015 *, 0.467–0.905) |
| CK (S.D. **) U/L | 91.33 (45.8) | 925.04 (3104) | 0.651 | 3.394 (p = 0.065 0.375–1.783) | 754 (1175.3) | 1129.9 (2054.4) | 0.549 | 1.463 (p = 0.226, 0.586–9.291)) |
| AST (S.D. **, U/L | 53.67 (64.6) | 61.88 (92.9) | 0.884 | 0.145 (p = 0.704 0.128–21.732) | 119.5 (83.5) | 79.28 (129.8) | 0.304 | 8.289 (p = 0.004 *, 1.648–49.137) |
| Myoglobulin (S.D. **), ng/mL | 124.3 (120.3) | 183.9 (110.4) | 0.184 | 2.969 (p = 0.085 0.028–1.997) | 512.34 (723.1) | 1133.4 (1219.3) | 0.279 | 0.034 (p = 0.853, 0.118–13.24) |
| ESR (S.D. **) mm/h | 86.5 (3.5) | 44.4 (34.9) | 0.106 | 2.776 (p = 0.096 0.319–1.722) | 57.08 (35.6) | 49.1 (37.9) | 0.556 | 0.075 (p = 0.784, 0.278–5.454) |
| IgE (S.D. **) KU/L | 1053.5 (369.8) | 130.24 (106.6) | 0.000 * | 2.055 (p = 0.152 0.15–0.455) | 127.36 (149.8) | 303.12 (172.6) | 0.108 | 2.284 (p = 0.131, 0.008–2.181) |
| anti-Ro52 antibodies (+) | 0 (0%) | 9 (100%) | - | 2.1 (p = 0.147 0.54–3.88) | 0 (0%) | 9 (100%) | - | 2.076 (p = 0.15, 0.642–12.926) |
| Smoking (+) | 1 (11.1%) | 8 (88.9%) | - | 0.043 (p = 0.836 0.104–16.55) | 1 (11.1%) | 8 (88.9%) | - | 1.949 (p = 0.163, 0.026–2.269) |
| Non-DM with Anti-MDA5 | DM with Anti-MDA5 | p-Value | |
|---|---|---|---|
| Age, y/o | 64.7 (13.9) | 62.4 (13.9) | 0.480 |
| AST (S.D.), U/L | 63.83 (89.1) | 91.64 (116.6) | 0.287 |
| LDH (S.D.), U/L | 344.16 (133.9)) | 468.43 (194.7) | 0.04 * |
| Myoglobulin (S.D.), ng/mL | 212.67 (163.4) | 729.59 (981.5) | 0.223 |
| CRP (S.D.), mg/dL | 4.19 (6.9) | 4.15 (6.8) | 0.981 |
| ESR (S.D.), mm/h | 51.12 (37.6) | 49.1 (35.0) | 0.833 |
| Ferritin (S.D.), ng/mL | 959.89 (1427.2) | 2179.56 (2054.8) | 0.033 * |
| CA-153 (S.D.), U/mL | 21.4 (26.3) | 19.08 (12.9) | 0.826 |
| CEA (S.D.), ng/mL | 7.75 (6.47) | 7.78 (8.1) | 0.99 |
| IgE (S.D.), KU/L | 296.5 (369.7) | 208.9 (192.2) | 0.524 |
| Alb (S.D.), g/dL | 3.46 (0.82) | 3.22 (0.76) | 0.278 |
| CK (S.D.), U/L | 755.8 (2839) | 1039.2 (1772.1) | 0.657 |
| Anti-RO52 antibody | 8 (26.7%) | 22 (73.3%) | 0.009 * |
| Anti-SAE antibody | 24 (75%) | 8 (25%) | <0.001 * |
| RPILD | 11 (33.3%) | 22 (66.7%) | 0.094 |
| Mortality # | 3 (17.6%) | 14(82.4%) | 0.012 * |
| Variable | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI of OR | p Value | OR | 95% CI of OR | p Value | |
| Female | 1.500 | 0.559–4.025 | 0.421 | 0.494 | 0.057–4.311 | 0.523 |
| High AST * | 2.267 | 0.850–6.045 | 0.102 | 3.858 | 0.493–3.172 | 0.198 |
| High LDH ** | 1.609 | 0.351–7.377 | 0.54 | 0.254 | 0.01–6.357 | 0.404 |
| High Ferritin *** | 5.308 | 0.5–56.391 | 0.166 | 10.713 | 0368–312.028 | 0.168 |
| Ro52 | 3.331 | 1.245–8.91 | 0.017 § | 2.198 | 0.116–41.489 | 0.599 |
| SAE | 0.245 | 0.9–0.668 | 0.006 § | 0.058 | 0.004–0.829 | 0.036 § |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-C.; Chen, W.-S.; Sun, Y.-S.; Lai, C.-C.; Yang, Y.-Y.; Chou, W.-R.; Liao, H.-T.; Tsai, C.-Y.; Chou, C.-T. Antibodies against Small Ubiquitin-like Modifier Activating Enzyme May Be a Protective Factor from Rapid Progressive Interstitial Lung Disease in Patients Bearing Antibodies against Melanoma Differentiation Associated Gene 5. J. Clin. Med. 2024, 13, 725. https://doi.org/10.3390/jcm13030725
Tsai H-C, Chen W-S, Sun Y-S, Lai C-C, Yang Y-Y, Chou W-R, Liao H-T, Tsai C-Y, Chou C-T. Antibodies against Small Ubiquitin-like Modifier Activating Enzyme May Be a Protective Factor from Rapid Progressive Interstitial Lung Disease in Patients Bearing Antibodies against Melanoma Differentiation Associated Gene 5. Journal of Clinical Medicine. 2024; 13(3):725. https://doi.org/10.3390/jcm13030725
Chicago/Turabian StyleTsai, Hung-Cheng, Wei-Sheng Chen, Yi-Syuan Sun, Chien-Chih Lai, Ying-Ying Yang, Wen-Ru Chou, Hsien-Tzung Liao, Chang-Youh Tsai, and Chung-Tei Chou. 2024. "Antibodies against Small Ubiquitin-like Modifier Activating Enzyme May Be a Protective Factor from Rapid Progressive Interstitial Lung Disease in Patients Bearing Antibodies against Melanoma Differentiation Associated Gene 5" Journal of Clinical Medicine 13, no. 3: 725. https://doi.org/10.3390/jcm13030725
APA StyleTsai, H.-C., Chen, W.-S., Sun, Y.-S., Lai, C.-C., Yang, Y.-Y., Chou, W.-R., Liao, H.-T., Tsai, C.-Y., & Chou, C.-T. (2024). Antibodies against Small Ubiquitin-like Modifier Activating Enzyme May Be a Protective Factor from Rapid Progressive Interstitial Lung Disease in Patients Bearing Antibodies against Melanoma Differentiation Associated Gene 5. Journal of Clinical Medicine, 13(3), 725. https://doi.org/10.3390/jcm13030725