
Association between Unplanned Conversion and Patient Survival after Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Propensity Score Matched Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Variables
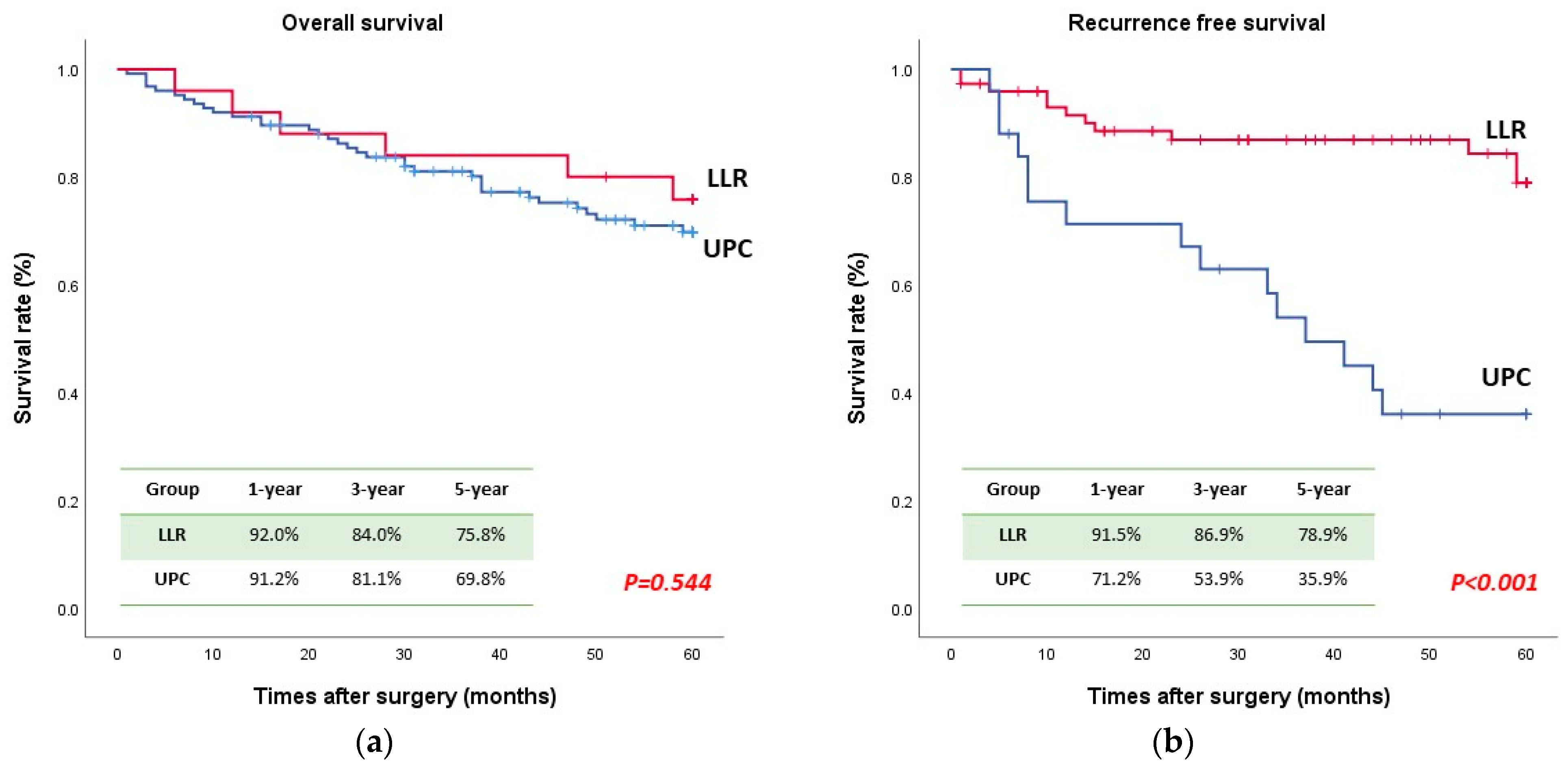
2.2. Survival Outcomes
2.3. Statistical Analysis
3. Results
3.1. Demographic and Disease Characteristics
3.2. Surgical and Oncological Outcomes
3.3. Survival Analysis
3.4. Univariate and Multivariable Analysis of Risk Factors Associated with Poor OS and RFS
3.5. Risk Factors Associated with UPC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korean Liver Cancer Association (KLCA) and National Cancer Center (NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 583–705. [Google Scholar] [CrossRef]
- Hendi, M.; Lv, J.; Cai, X.J. Current status of laparoscopic hepatectomy for the treatment of hepatocellular carcinoma: A systematic literature review. Medicine 2021, 100, e27826. [Google Scholar] [CrossRef] [PubMed]
- Haney, C.M.; Studier-Fischer, A.; Probst, P.; Fan, C.; Müller, P.C.; Golriz, M.; Diener, M.K.; Hackert, T.; Müller-Stich, B.P.; Mehrabi, A.; et al. A systematic review and meta-analysis of randomized controlled trials comparing laparoscopic and open liver resection. HPB 2021, 23, 1467–1481. [Google Scholar] [CrossRef] [PubMed]
- Halls, M.C.; Cipriani, F.; Berardi, G.; Barkhatov, L.; Lainas, P.; Alzoubi, M.; D’Hondt, M.; Rotellar, F.; Dagher, I.; Aldrighetti, L.; et al. Conversion for unfavorable intraoperative events results in significantly worst outcomes during laparoscopic liver resection: Lessons learned from a multicenter review of 2861 cases. Ann. Surg. 2018, 268, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Wexner, S.D.; Safar, B.; Jobanputra, S.; Jin, H.; Li, V.K.; Nogueras, J.J.; Weiss, E.G.; Sands, D.R. Conversion in laparoscopic surgery: Does intraoperative complication influence outcome? Surg. Endosc. 2009, 23, 2454–2458. [Google Scholar] [CrossRef] [PubMed]
- Lof, S.; Korrel, M.; van Hilst, J.; Moekotte, A.L.; Bassi, C.; Butturini, G.; Boggi, U.; Dokmak, S.; Edwin, B.; Falconi, M.; et al. European Consortium on Minimally Invasive Pancreatic Surgery (E-MIPS). Outcomes of Elective and Emergency Conversion in Minimally Invasive Distal Pancreatectomy for Pancreatic Ductal Adenocarcinoma: An International Multicenter Propensity Score-matched Study. Ann. Surg. 2019, 274, e1001–e1007. [Google Scholar] [CrossRef]
- Mungo, B.; Papageorge, C.M.; Stem, M.; Molena, D.; Lidor, A.O. The impact of operative approach on postoperative complications following colectomy for colon caner. World J. Surg. 2017, 41, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Clancy, C.; O’Leary, D.P.; Burke, J.P.; Redmond, H.P.; Coffey, J.C.; Kerin, M.J.; Myers, E. A meta-analysis to determine the oncological implications of conversion in laparoscopic colorectal cancer surgery. Color. Dis. 2015, 17, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.; Cho, J.Y.; Han, H.-S.; Yoon, Y.-S.; Lee, H.W.; Lee, J.S.; Lee, B.; Kim, M.; Jo, Y. Risk factors and long-term implications of unplanned conversion during laparoscopic liver resection for hepatocellular carcinoma located in anterolateral liver segments. J. Minim. Invasive Surg. 2021, 24, 191–199. [Google Scholar] [CrossRef]
- Yerokun, B.A.; Adam, M.A.; Sun, Z.; Kim, J.; Sprinkle, S.; Migaly, J.; Mantyh, C.R. Does conversion in laparoscopic colectomy portend an inferior oncologic outcome? Results from 104,400 patients. J. Gastrointest. Surg. 2016, 20, 1042–1048. [Google Scholar] [CrossRef]
- Franko, J.; Fassler, S.A.; Rezvani, M.; O’connell, B.G.; Harper, S.G.; Nejman, J.H.; Zebley, D.M. Conversion of laparoscopic colon resection does not affect survival in colon cancer. Surg. Endosc. 2008, 22, 2631–2634. [Google Scholar] [CrossRef] [PubMed]
- Aghayan, D.L.; Fretland, A.; Kazaryan, A.M.; Sahakyan, M.A.; Dagenborg, V.J.; Bjørnbeth, B.A.; Flatmark, K.; Kristiansen, R.; Edwin, B. Laparoscopic versus open liver resection in the posterosuperior segments: A sub-group analysis from the OSLO-COMET randomized controlled trial. HPB 2019, 21, 1485–1490. [Google Scholar] [CrossRef]
- Cho, J.Y.; Han, H.S.; Yoon, Y.S.; Shin, S.H. Feasibility of laparoscopic liver resection for tumors located in the posterosuperior segments of the liver, with a special reference to overcoming current limitations on tumor location. Surgery 2008, 144, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Xu, Z.; Sun, D.; Jiao, C.; Ji, G.; Wang, K. A comprehensive framework of the right posterior section for tailored anatomical liver resection based on three-dimensional simulation system. Ann. Transl. Med. 2022, 10, 852. [Google Scholar] [CrossRef] [PubMed]
- Troisi, R.I.; Montalti, R.; Van Limmen, J.G.; Cavaniglia, D.; Reyntjens, K.; Rogiers, X.; De Hemptinne, B. Risk factors and management of conversions to an open approach in laparoscopic liver resection: Analysis of 265 consecutive cases. HPB 2014, 16, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Terminology Committee of the International Hepato-Pancreato-Biliary Association 2000 IHPBA Brisbane 2000. Terminology of liver anatomy and resections. HPB 2000, 2, 333–339. [Google Scholar]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Ciria, R.; Padial, A.; Ayllón, M.D.; García-Gaitan, C.; Briceño, J. Fast-track protocols in laparoscopic liver surgery: Applicability and correlation with difficulty scoring systems. World J. Gastrointest. Surg. 2022, 14, 211–220. [Google Scholar] [CrossRef]
- Wang, Z.-Y.; Chen, Q.L.; Sun, L.L.; He, S.P.; Luo, X.F.; Huang, L.S.; Huang, J.H.; Xiong, C.M.; Zhong, C. Laparoscopic versus open major liver resection for hepatocellular carcinoma: Systematic review and meta-analysis of comparative cohort studies. BMC Cancer 2019, 19, 1047. [Google Scholar] [CrossRef]
- Cheung, T.T.; Dai, W.C.; Tsang, S.H.; Chan, A.C.; Chok, K.S.; Chan, S.C.; Lo, C.M. Pure Laparoscopic Hepatectomy Versus Open Hepatectomy for Hepatocellular Carcinoma in 110 Patients With Liver Cirrhosis: A Propensity Analysis at a Single Center. Ann. Surg. 2016, 264, 612–620. [Google Scholar] [CrossRef]
- Han, H.-S.; Shehta, A.; Ahn, S.; Yoon, Y.-S.; Cho, J.Y.; Choi, Y. Laparoscopic versus open liver resection for hepatocellular carcinoma: Case-matched study with propensity score matching. J. Hepatol. 2015, 63, 643–650. [Google Scholar] [CrossRef]
- Lee, J.Y.; Rho, S.Y.; Han, D.H.; Choi, J.S.; Choi, G.H. Unplanned conversion during minimally invasive liver resection for hepatocellular carcinoma: Risk factors and surgical outcomes. Ann. Surg. Treat Res. 2020, 98, 23–30. [Google Scholar] [CrossRef]
- Costi, R.; Scatton, O.; Haddad, L.; Randone, B.; Andraus, W.; Massault, P.P.; Soubrane, O. Lessons learned from the first 100 laparoscopic liver resections: Not delaying conversion may allow reduced blood loss and operative time. J. Laparoendosc. Adv. Surg. Tech. 2012, 22, 425–431. [Google Scholar] [CrossRef]
- Bodur, M.S.; Tomas, K.; Topaloğlu, S.; Oğuz, Ş.; Küçükaslan, H.; Dohman, D.; Karabulut, E.; Çalık, A. Effects of intraoperative blood loss during liver resection on patients’ outcome: A single- center experience. Turk. J. Med. Sci. 2021, 51, 1388–1395. [Google Scholar] [CrossRef]
- Stiles, Z.E.; Glazer, E.S.; Deneve, J.L.; Shibata, D.; Behrman, S.W.; Dickson, P.V. Long-Term Implications of Unplanned Conversion During Laparoscopic Liver Resection for Hepatocellular Carcinoma. Ann. Surg. Oncol. 2019, 26, 282–289. [Google Scholar] [CrossRef]
- Katz, S.C.; Shia, J.; Liau, K.H.; Gonen, M.; Ruo, L.; Jarnagin, W.R.; Fong, Y.; D’Angelica, M.I.; Blumgart, L.H.; DeMatteo, R.P. Operative blood loss independently predicts recurrence and survival after resection of hepatocellular carcinoma. Ann. Surg. 2009, 249, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.H.; Lee, D.; Jung, K.W.; Won, Y.J.; Cho, H. Cause of death and cause-specific mortality for primary liver cancer in South Korea: A nationwide population-based study in hepatitis B virus-endemic area. Clin. Mol. Hepatol. 2022, 28, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Matsuda, M.; Ohkura, Y.; Kawamura, Y.; Inoue, M.; Hashimoto, M.; Ikeda, K.; Kumada, H.; Watanabe, G. Factors associated with early cancer-related death after curative hepatectomy for solitary small hepatocellular carcinoma without macroscopic vascular invasion. J. Hepatobiliary Pancreat. Sci. 2014, 21, 142–147. [Google Scholar] [CrossRef]
- Liu, B.; Teng, F.; Fu, H.; Guo, W.Y.; Shi, X.M.; Ni, Z.J.; Gao, X.G.; Ma, J.; Fu, Z.R.; Ding, G.S. Excessive intraoperative blood loss independently predicts recurrence of hepatocellular carcinoma after liver transplantation. BMC Gastroenterol. 2015, 15, 138. [Google Scholar] [CrossRef] [PubMed]
- Harada, N.; Shirabe, K.; Maeda, T.; Kayashima, H.; Ishida, T.; Maehara, Y. Blood transfusion is associated with recurrence of hepatocellular carcinoma after hepatectomy in Child-Pugh class A patients. World J. Surg. 2015, 39, 1044–1051. [Google Scholar] [CrossRef]
- Rajendran, L.; Ivanics, T.; Claasen, M.P.; Muaddi, H.; Sapisochin, G. The management of post-transplantation recurrence of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 1–16. [Google Scholar] [CrossRef]
- Chok, K.S.; Ng, K.K.; Poon, R.T.; Lo, C.M.; Fan, S.T. Impact of postoperative complications on long-term outcome of curative resection for hepatocellular carcinoma. Br. J. Surg. 2009, 96, 81–87. [Google Scholar] [CrossRef]
- Zhou, Y.M.; Zhang, X.F.; Li, B.; Sui, C.J.; Yang, J.M. Postoperative complications affect early recurrence of hepatocellular carcinoma after curative resection. BMC Cancer 2015, 15, 689. [Google Scholar] [CrossRef]
- Farid, S.G.M.; Aldouri, A.F.; Morris-Stiff, G.F.; Khan, A.Z.F.; Toogood, G.J.F.; Lodge, J.P.A.F.; Prasad, K.R.F. Correlation between postoperative infective complications and long-term outcomes after hepatic resection for colorectal liver metastasis. Ann. Surg. 2010, 251, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Han, H.-S.; Choi, Y.; Yoon, Y.-S.; Kim, S.; Choi, J.K.; Jang, J.S.; Kwon, S.U.; Kim, H. Association of Remnant Liver Ischemia With Early Recurrence and Poor Survival After Liver Resection in Patients With Hepatocellular Carcinoma. JAMA Surg. 2017, 152, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Van Zee, K.J.; DeForge, L.E.; Fischer, E.; Marano, M.A.; Kenney, J.S.; Remick, D.G.; Lowry, S.F.; Moldawer, L.L. IL-8 in septic shock, endotoxemia, and after IL-1 administration. J. Immunol. 1991, 146, 3478–3482. [Google Scholar] [CrossRef] [PubMed]
- Berardi, G.; Muttillo, E.M.; Colasanti, M.; Mariano, G.; Meniconi, R.L.; Ferretti, S.; Guglielmo, N.; Angrisani, M.; Lucarini, A.; Garofalo, E.; et al. Challenging Scenarios and Debated Indications for Laparoscopic Liver Resections for Hepatocellular Carcinoma. Cancers 2023, 15, 1493. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Unmatched | After Applying PSM | |||||
|---|---|---|---|---|---|---|
| Variables | UPC (N = 29) | LLR (N = 222) | p Value | UPC (N = 25) | LLR (N = 120) | p Value |
| Demographic data | ||||||
| Age (years) | 62.1 ± 10.5 | 61.2 ± 10.1 | 0.569 | 61.9 ± 10.5 | 61.4 ± 10.2 | 0.742 |
| Male (n [%]) | 22 (75.9%) | 171 (77.0%) | 0.820 | 18 (72.0%) | 94 (75.2%) | 0.802 |
| BMI (kg/m2) | 24.8 ± 3.2 | 24.8 ± 3.3 | 0.929 | 24.8 ± 3.4 | 24.6 ± 3.1 | 0.659 |
| HTN (n [%]) | 14 (48.3%) | 101 (45.5%) | 0.844 | 13 (52.0%) | 57 (45.6%) | 0.662 |
| Diabetes (n [%]) | 10 (34.5%) | 65 (29.3%) | 0.666 | 9 (36.0%) | 38 (30.4%) | 0.639 |
| Prior abdominal surgery (n [%]) | 6 (20.7%) | 70 (31.5%) | 0.286 | 6 (24.0%) | 29 (23.2%) | 1.000 |
| Preoperative data | ||||||
| Etiology (n [%]) | 0.451 | 0.607 | ||||
| Hepatitis B | 16 (55.2%) | 148 (67.0%) | 14 (56.0%) | 82 (66.1%) | ||
| Hepatitis C | 2 (6.9%) | 12 (5.4%) | 2 (8.0%) | 9 (7.3%) | ||
| MELD score | 7.9 ± 1.3 | 7.7 ± 2.1 | 0.590 | 7.9 ± 1.2 | 7.9 ± 2.4 | 0.550 |
| Child-Pugh score | 0.001 | 0.262 | ||||
| A | 24 (82.8%) | 218 (98.2%) | 23 (92.0%) | 121 (96.8%) | ||
| B | 5 (17.2%) | 4 (1.8%) | 2 (8.0%) | 4 (3.2%) | ||
| Bilirubin (mg/dL) | 0.8 ± 0.5 | 0.8 ± 0.4 | 0.695 | 0.7 ± 0.5 | 0.8 ± 0.4 | 0.477 |
| ALT (IU/L) | 43.4 ± 26.6 | 46.5 ± 83.1 | 0.524 | 43.9 ± 28.3 | 49.8 ± 102.8 | 0.503 |
| AST (IU/L) | 49.4 ± 29.2 | 48.7 ± 87.3 | 0.725 | 50.1 ± 31.2 | 55.2 ± 111.7 | 0.513 |
| Albumin (g/dL) | 3.9 ± 0.6 | 4.2 ± 0.4 | 0.003 | 4.0 ± 0.5 | 4.1 ± 0.5 | 0.976 |
| INR | 1.1 ± 0.1 | 1.1 ± 0.1 | 0.983 | 1.1 ± 0.1 | 1.1 ± 0.1 | 0.648 |
| Platelet count (×103/μL) | 156.0 ± 50.7 | 187.1 ± 67.7 | 0.262 | 157.4 ± 49.8 | 177.4 ± 72.1 | 0.190 |
| Prior TACE (n [%]) | 8 (27.6%) | 49 (22.2%) | 0.448 | 7 (28.0%) | 32 (25.8%) | 0.807 |
| Prior RFA (n [%]) | 2 (6.9%) | 25 (11.3%) | 0.750 | 2 (8.0%) | 11 (8.8%) | 1.000 |
| AFP (ng/mL) | 191.9 ± 604.0 | 474.8 ± 2369.8 | 0.318 | 103.5 ± 298.4 | 298.3 ± 1061.8 | 0.128 |
| Preoperative Tumor size (cm) | 4.2 ± 2.8 | 3.3 ± 2.2 | 0.013 | 4.0 ± 2.5 | 3.2 ± 2.1 | 0.139 |
| Variables | UPC (N = 25) | LLR (N = 120) | p Value |
|---|---|---|---|
| Operation type (n [%]) | 0.369 | ||
| Right hemihepatectomy | 8 (32.0%) | 14 (11.2%) | |
| Right anterior sectionectomy | 0 | 1 (6.4%) | |
| Right posterior sectionectomy | 3 (12.0%) | 16 (13.3%) | |
| Segmentectomy | 3 (12.0%) | 35 (28.0%) | |
| Tumorectomy | 11 (44.0%) | 54 (43.2%) | |
| Operative parameters | |||
| Operation time (min) | 337.2 ± 203.1 | 302.7 ± 173.2 | 0.254 |
| Estimated blood loss (mL) | 3172.1 ± 4527.0 | 809.4 ± 1026.4 | <0.001 |
| Transfusion (n [%]) | 12 (48.0%) | 31 (24.8%) | 0.028 |
| Pringle maneuver (n [%]) | 15 (62.8%) | 65 (52.0%) | 0.379 |
| Pringle maneuver (min) | 40.5 ± 2.5 | 40.9 ± 27.9 | 0.783 |
| Postoperative data | |||
| Hospital stays (days) | 14.8 ± 18.3 | 8.9 ± 8.3 | 0.015 |
| C-D complications (n [%]) | 0.042 | ||
| IIIa | 6 (24.0%) | 13 (11.8%) | |
| IIIb | 1 (4.0%) | 4 (3.6%) | |
| IV | 0 | 2 (1.8%) | |
| V | 0 | 1 (0.9%) | |
| Pathologic data | |||
| R0 resection rate (n [%]) | 23 (92.0%) | 119 (95.2%) | 0.621 |
| Surgical margin (cm) | 0.9 ± 1.2 | 0.6 ± 0.8 | 0.523 |
| Microvascular invasion (n [%]) | 10 (40.0%) | 61 (48.8%) | 0.512 |
| Serosal invasion (n [%]) | 7 (28.0%) | 31 (24.8%) | 0.802 |
| Tumor stage | 0.701 | ||
| I | 11 (44.0%) | 60 (48.0%) | |
| II | 11 (44.0%) | 54 (43.2%) | |
| III | 2 (8.0%) | 5 (4.0%) | |
| IV | 1 (4.0%) | 2 (1.6%) | |
| Total necrosis | 0 | 4 (3.2%) |
| Overall Survival | Disease Free Survival | |||||
|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||
| Risk Factor | p Value | HR (95% CI) | p Value | p Value | HR (95% CI) | p Value |
| Age, ≥65 (years) | 0.027 | 0.385 | ||||
| Male, | 0.420 | 0.776 | ||||
| BMI < 18.5 kg/m2, | 0.022 | 2.073 (1.055–4.072) | 0.034 | 0.961 | ||
| Previous abdominal surgery | 0.065 | |||||
| Preop. TACE | 0.578 | 0.384 | ||||
| Preop. RFA | 0.574 | 0.407 | ||||
| Child-Pugh score B | 0.503 | |||||
| Albumin < 3.5 g/dL | 0.016 | 3.497 (1.600–7.646) | 0.002 | 0.172 | ||
| Platelet count < 100 (×103/μL) | 0.481 | 0.001 | 2.081 (1.161–3.730) | 0.014 | ||
| Cirrhosis | 0.439 | 0.286 | ||||
| Tumor size > 5 cm | 0.024 | 0.943 (0.472–1.885) | 0.868 | 0.849 | ||
| Operation type | 0.706 | 0.027 | ||||
| LLR | Reference | |||||
| UPC | 2.203 (1.045–4.643) | 0.038 | ||||
| Operation time > 300 min | 0.012 | 2.840 (1.121–7.194) | 0.028 | 0.325 | ||
| Intraoperative blood loss > 1000 mL | 0.002 | 1.379 (0.510–3.726) | 0.527 | <0.001 | 2.194 (1.119–4.299) | 0.022 |
| Intraoperative transfusion | 0.002 | 0.768 (0.275–2.146) | 0.614 | <0.001 | 1.353 (0.701–2.609) | 0.368 |
| Resection margin (R1) | 0.666 | 0.062 | ||||
| Microvascular invasion | <0.001 | 2.503 (1.022–6.798) | 0.042 | 0.002 | 2.401 (1.344–4.288) | 0.003 |
| Serosal invasion | 0.760 | 0.873 | ||||
| pT | ||||||
| 1 | Reference | Reference | ||||
| 2 | 0.872 | 1.063 (0.108–10.464) | 0.985 | 0.217 | ||
| 3 | 0.289 | 2.528 (0.223–28.698) | 0.454 | 0.517 | ||
| 4 | 0.013 | 6.692 (1.119–14.698) | 0.041 | 0.299 | ||
| Major complication (C-D ≥ III) | 0.162 | 0.182 | ||||
| Hospital stay (>7 days) | 0.043 | 0.921 (0.329–2.573) | 0.875 | 0.250 | ||
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age | 0.358 | |||
| <65 years | Reference | |||
| ≥65 years | 1.442 (0.660–3.151) | |||
| Male sex | 1.067 (0.431–2.640) | 0.889 | ||
| BMI | 0.328 | |||
| <25 kg/m2 | Reference | |||
| ≥25 kg/m2 | 1.474 (0.677–3.210) | |||
| Hypertension | 1.087 (0.489–2.141) | 0.838 | ||
| Diabetes mellitus | 1.594 (0.679–3.741) | 0.285 | ||
| Previous abdominal surgery | 0.566 (0.214–1.472) | 0.267 | ||
| Previous TACE | 1.310 (0.547–3.138) | 0.544 | ||
| Previous RFA | 0.584 (0.131–2.604) | 0.480 | ||
| Albumin | 0.001 | 0.001 | ||
| <3.5 g/dL | 4.808 (1.923–12.022) | 4.873 (1.904–12.474) | ||
| ≥3.5 g/dL | Reference | |||
| Platelet count | 0.037 | |||
| <100 (×103/μL) | 1.391 (1.002–5.072) | |||
| ≥100 (×103/μL) | Reference | |||
| Cirrhosis (Preoperative Imaging) | 1.586 (0.700–3.595) | 0.269 | ||
| Tumor size | 0.240 | |||
| <3 cm | Reference | |||
| ≥3 cm | 1.593 (0.732–3.468) | 1.014 (0.230–2.679) | 0.714 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, B.; Cho, J.Y.; Han, H.-S.; Yoon, Y.-S.; Lee, H.W.; Kang, M.; Park, Y.; Kim, J. Association between Unplanned Conversion and Patient Survival after Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Propensity Score Matched Analysis. J. Clin. Med. 2024, 13, 1116. https://doi.org/10.3390/jcm13041116
Lee B, Cho JY, Han H-S, Yoon Y-S, Lee HW, Kang M, Park Y, Kim J. Association between Unplanned Conversion and Patient Survival after Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Propensity Score Matched Analysis. Journal of Clinical Medicine. 2024; 13(4):1116. https://doi.org/10.3390/jcm13041116
Chicago/Turabian StyleLee, Boram, Jai Young Cho, Ho-Seong Han, Yoo-Seok Yoon, Hae Won Lee, MeeYoung Kang, Yeshong Park, and Jinju Kim. 2024. "Association between Unplanned Conversion and Patient Survival after Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Propensity Score Matched Analysis" Journal of Clinical Medicine 13, no. 4: 1116. https://doi.org/10.3390/jcm13041116
APA StyleLee, B., Cho, J. Y., Han, H. -S., Yoon, Y. -S., Lee, H. W., Kang, M., Park, Y., & Kim, J. (2024). Association between Unplanned Conversion and Patient Survival after Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Propensity Score Matched Analysis. Journal of Clinical Medicine, 13(4), 1116. https://doi.org/10.3390/jcm13041116