Abstract
Background: We retrospectively investigated the effects of the severity and classification of sleep-disordered breathing (SDB) on left ventricular (LV) function in patients with ST-segment elevation myocardial infarction (STEMI). Methods: A total of 115 patients with STEMIs underwent a sleep study using a multichannel frontopolar electroencephalography recording device (Sleep Profiler) one week after STEMI onset. We evaluated LV global longitudinal strain (LV-GLS) using two-dimensional echocardiography at one week and seven months. Patients were classified as no SDB (AHI < 5 events/h), obstructive SDB (over 50% of apnea events are obstructive), and central SDB (over 50% of apnea events are central). Due to the device’s limitations in distinguishing obstructive from central hypopnea, SDB classification was based on apnea index percentages. Results: The obstructive apnea index (OAI) was significantly associated with LV-GLS at one week (r = 0.24, p = 0.027) and seven months (r = 0.21, p = 0.020). No such correlations were found for the central apnea index and SDB classification. Multivariable regression analysis showed that the OAI was independently associated with LV-GLS at one week (β = 0.24, p = 0.002) and seven months (β = 0.20, p = 0.008). Conclusions: OAI is associated with persistent LV dysfunction assessed by LV-GLS in STEMI.
1. Introduction
Among patients with ST-segment elevation myocardial infarction (STEMI), those with sleep-disordered breathing (SDB) have a higher incidence of adverse cardiovascular events than those without SDB [1,2]. There are two main types of SDB: obstructive sleep apnea (OSA) and central sleep apnea (CSA). OSA was reported to be associated with left ventricular (LV) remodeling and infarct size after STEMI [3,4]. CSA was also reported as the prognostic factor of acute myocardial infarctions (AMI) [5,6,7]. However, the effect of CSA on LV function and structure following STEMIs remains unclear [4].
Recent studies have revealed that left ventricular global longitudinal strain (LV-GLS) measured by two-dimensional echocardiography (2DE) after STEMI is the most promising marker of LV dysfunction and a superior predictor of outcome compared to the conventional echocardiographic parameters of LV function, such as LV ejection fraction (LVEF) or the wall motion score index [8,9]. LV-GLS is useful in patients with STEMIs with preserved LVEF [10] but also in ischemic cardiomyopathy with reduced LVEF [11]; LV-GLS values represent total LV myocardial function, which includes infarct damage [8].
However, the effect of SDB on LV function assessed by LV-GLS after STEMI has yet to be investigated. This study aimed to identify the association between the severity and the type of SDB with serial LV-GLS after the first STEMI. Our findings would be beneficial for classifying more severely ill STEMI patients with SDB at an early stage.
2. Materials and Methods
2.1. Study Design
This study was a retrospective observational study. Between December 2016 and January 2020, 378 consecutive patients hospitalized for STEMIs at our medical center were recruited. We analyzed patients with a first incident of STEMI who underwent a sleep study and 2DE one week and 7 (±2) months after the onset of STEMI to examine the influence of SDB on LV dysfunction after STEMIs.
Patients meeting any of the following criteria were excluded: in-hospital death, active cancer, treated SDB, chronic obstructive pulmonary disease, interstitial pneumonia, significant valvular heart disease, history of cardiomyopathy, history of open-heart surgery, indication for surgical revascularization, pacemaker rhythm, chronic atrial fibrillation, hemodynamic instability, unfeasible follow-up (e.g., residing in a distant location), inability to provide informed consent, refusal to undergo a sleep study, incomplete sleep data, inadequate image quality, lost to follow-up, no second echocardiography, and no EchoPAC data at second echocardiography. The eligibility criteria were met by 115 patients who were enrolled in the study (Figure 1). The study protocol was approved by the Ethics Committee of Yokohama City University (F221200035, 1 December 2023), and the study complied with the provisions of the Declaration of Helsinki. The ethics committee waived the requirement for individual informed consent because of the retrospective nature of the study and the availability of the patient data.
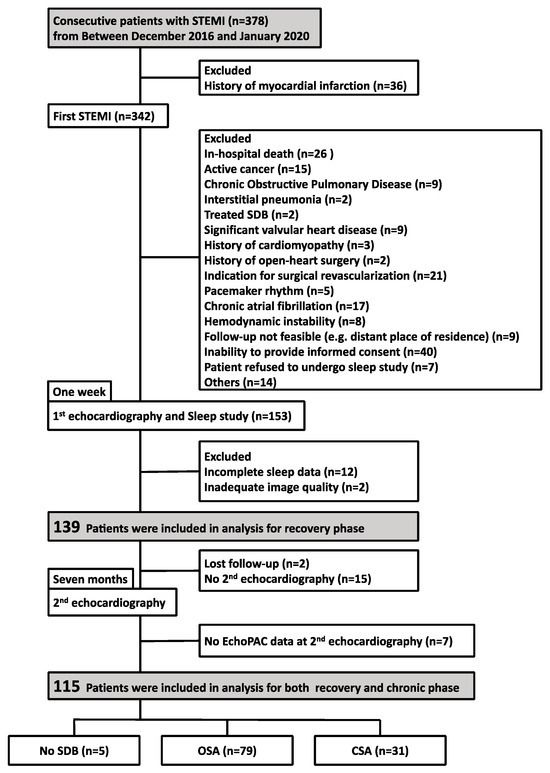
Figure 1.
Study flow chart. Footnotes: CSA, central sleep apnea; OSA, obstructive sleep apnea; SDB, sleep-disordered breathing; STEMI, ST-segment elevation myocardial infarction.
2.2. Clinical, Laboratory, and Instrumental Data
STEMI was defined as chest pain lasting at least 30 min with new ST-segment elevation and an elevated cardiac troponin I level > 99th percentile of a standard population reference [12]. The following criteria were used to define ST-segment elevation: new ST-segment elevation at J in at least two contiguous leads of 0.2 mV in men or 0.15 mV in women in leads V2–V3, or 0.1 mV in other leads. New left bundle branch block was also considered as STEMI. Treatment of all patients followed the current guidelines of the Japanese Circulation Society [13]. For one week, a sleep study using multichannel frontopolar electroencephalography recordings was performed using a forehead-worn recording device (Sleep Profiler, Advanced Brain Monitoring, Carlsbad, CA, USA) (Figure 2) [14,15]. Sleep profilers are ambulatory sleep electroencephalography (EEG) devices that can assess sleep architecture and continuity with acceptable comparability to the gold standard laboratory procedure of polysomnography [14]. The Sleep Profiler was applied to the forehead at approximately 9:00 p.m., and the device was removed in the morning at a convenient time. Recordings were transferred to the portal, and software was used to verify signal quality and automatic staging visually. The portable monitor recorded the nasal pressure, chest movements, snoring, body position, activity, pulse oximetry, heart rate, and oxygen saturation signals. The data from the Sleep Profiler were manually scored using 11 sleep technicians blinded to the clinical data. All technicians had more than three years of experience performing these analyses. Definitions and scoring methods were based on the American Academy of Sleep Medicine (AASM) version 2.1 [16] Apnea and hypopnea events were quantified, and SDB severity was assessed using the frequency of apnea and hypopnea events per hour of sleep (AI [apnea index]; HI [hypopnea index]) [16]. Obstructive and central AI scores were computed separately. We defined the obstructive apnea index (OAI) and central apnea index (CAI) as the mean number of obstructive apneas and central apnea. Since the Sleep Profiler®︎ cannot discriminate between obstructive and central sleep disturbance for hypopnea, the classification was based on the percentage of apnea index. The patients were divided into three groups based on the following specifications: no SDB (AHI < 5 events/h), an OSA-dominant group (≥50% of apnea events obstructive), or a CSA-dominant group (>50% of apnea events central) [16].
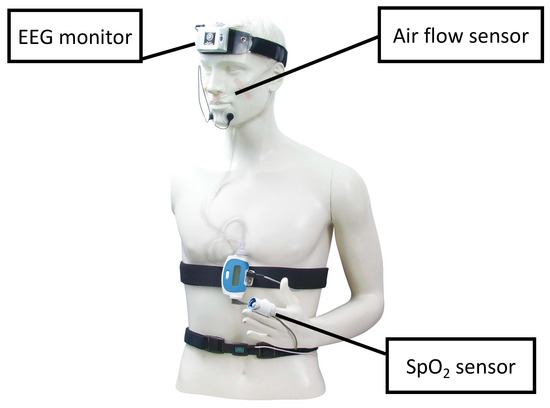
Figure 2.
Sleep apnea testing using the Sleep Profiler. All subjects underwent polysomnography for one week with a Sleep Profiler, which is a wireless, self-application, ambulatory EEG sleep monitoring. Footnotes: EEG, electroencephalogram.
A standardized 2DE study was performed by experienced sonographers using commercially available ultrasound systems (Vivid q, Vivid E9, or VividE95; GE Healthcare, Chicago, IL, USA) with 3.5 MHz or M5S transducers at the same time as the sleep study, one week and 7 (±2) months after the onset of STEMI. It is recognized that LV remodeling after AMI is generally considered to be substantially complete in approximately 90% of cases at approximately six months after onset [17,18]. Thus, we adopted 2DE at seven months to evaluate LV functional recovery. Standard 2D, color, continuous-wave, pulsed-wave, and Doppler images were acquired and stored in cine-loop format. Two-dimensional parasternal long-axis images determined LV cavity dimensions and wall thickness. The following LV diastolic parameters were measured: peak early (E) and late (A) diastolic velocities and E-wave deceleration times by pulsed-wave Doppler of transmitral flow. Tissue Doppler images of the left ventricle were obtained in the apical four-chamber view at the end of expiration, and the peak early diastolic myocardial velocity (E’) was measured at the base of the septum and the base of the lateral mitral annulus. The ratio of peak transmitral E-wave/septal e’ (E/e’ sep), the ratio of peak transmitral E-wave/lateral e’ (E/e’ lat), and the mean of E/e’ sep and E/e’ lat (E/e’ mean) were assessed. LVEF and left atrial volume were measured using the disk-summation method in the apical four-chamber and two-chamber views. LV end-diastolic and end-systolic volume and left atrial volume were indexed to body surface area.
Two-dimensional echocardiographic data were also analyzed offline (EchoPAC PC; GE Healthcare) by an experienced investigator blinded to baseline clinical data. LV-GLS analysis was performed by speckle tracking in three apical windows: apical longitudinal long-axis views, four-chamber views, and two-chamber views. A semi-automated function tracked the ventricular endocardium, and manual point-and-click adjustments were made if the tracking was inaccurate. Every projection covered six segments, resulting in 18 segments for the LV-GLS calculation. LV-GLS was calculated by the software as the average of the systolic longitudinal strain peaks of the three apical views. If systolic longitudinal strain peaks could only be assessed in two of the three apical views, the average of the longitudinal strain peaks in the two views was used to calculate the LV-GLS. Exclusions of segments due to obscuration by rib artifacts or lung tissue were made at the discretion of the analyses.
2.3. Statistical Analyses
Categorical variables are expressed as frequencies and percentages, and continuous data are expressed as the mean ± standard deviation or as medians and interquartile ranges. The groups of patients with no SDB, OSA, or CSA were compared using the Kruskal–Wallis test for continuous variables and a chi-square test or Fisher’s exact test for categorical variables. Univariate regression analyses were performed to predict the LV-GLS at 1 week and 7 months. Peak creatine kinase muscle and brain isoenzyme (CK-MB) (IU/l) levels, reperfusion within 12 h from onset of STEMI, culprit left descending artery, multi-vessel disease, age, final thrombolysis in myocardial infarction (TIMI) flow grade = 3, initial TIMI flow grade ≥ 2, AHI, OSA predominance, CSA-predominant, OAI, CAI, and CSR, all of which were considered important predictors of LV function, were included [19,20]. Next, univariate predictors of LV-GLS with p < 0.05 were entered into a multiple regression analysis using a forward stepwise algorithm (Models I, II, and III). AHI and apnea indexes were analyzed separately to avoid multicollinearity. All statistical analyses were performed using JMP pro 15.0 software (SAS Institute, Cary, NC, USA). For all analyses, p < 0.05 was considered to indicate statistical significance. The datasets produced or analyzed during this study are not publicly available due to privacy and ethical restrictions. These data are available from the corresponding author on reasonable request.
3. Results
3.1. Baseline Characteristics of Subjects
Table 1 shows the characteristics of the patients. The patients had an average age of 65 years (±11), and the majority were male (87%). The median peak CK-MB level was 198 IU/L (124–363). Differences in patient characteristics among the three groups were not observed, except that the frequency of females was relatively high in the CSA group. Sleep parameters in the three groups are shown in Table 1. Sleep stage did not vary amongst the four groups but showed less N3 stage overall. CSR was significantly more frequent in the CSA group.

Table 1.
Baseline characteristics.
3.2. Relationship between SDB and 2DE Parameters
Table 2 presents the baseline and follow-up 2DE parameters. The three groups demonstrated no significant differences in baseline LV end-diastolic volume index (LVEDVI), LVEF, LV-GLS, or other parameters. Next, we examined the relationship between the two apnea indices and the echocardiographic parameters (Table 3). The OAI was significantly associated with E/A, E/e’, and LV-GLS at one week. However, the CAI was not associated with these parameters. At seven months, the OAI was significantly associated with LVEDVI, LVESVI, E/A, and LV-GLS, whereas the CAI was not.
Table 2.
Two-dimensional echocardiography at one week and seven months.
Table 3.
The relationship between apnea index and echocardiographic parameters.
We have shown the relationship between LV functional improvement and sleep parameters. LV functional improvement was defined as the absolute difference between chronic and recovery LV-GLS greater than the median (0.9). We found no significant association between LV functional improvement and sleep parameters (Table 4).
Table 4.
The association between LV-GLS improvement and sleep parameters.
3.3. Multiple Regression Analyses for the Prediction of LV-GLS at One Week and Seven Months
The apnea index was hypothesized to be associated with LV-GLS after STEMI, and univariate and multiple regression analyses were performed to predict LV-GLS at one week and seven months. Regression analysis identified OAI and AHI as independent predictors of LV-GLS at one week (Models II and III in Table 5) (β coefficient = 0.24, p = 0.002; and β coefficient = 0.26, p < 0.001, respectively). OAI and AHI were also independent predictors of LV-GLS at seven months in a similar analysis (Models II and III in Table 6) (β coefficient = 0.20, p = 0.008; and β coefficient = 0.22, p = 0.004, respectively).
Table 5.
Univariate and multiple regression analyses for the prediction of LV-GLS at 1 week.
Table 6.
Univariate and multiple regression analyses for the prediction of LV-GLS at seven months.
4. Discussion
This study investigated the effect of SDB on LV function, assessed using LV-GLS after the first STEMI. Our results showed that OAI and AHI were independent predictors of persistent LV dysfunction assessed using LV-GLS after the first STEMI, whereas the classifications of SDB and CAI were not. This is the first study to demonstrate the effect of OAI on LV function measured by LV-GLS, a superior cardiac function index compared to conventional indices [8,9], after STEMI. In addition, the study presents the novel finding that obstructive apnea severity, rather than SDB classification, is associated with reduced LV systolic function after STEMI.
There have been reports of the relationship between OSA and cardiac functional recovery after STEMIs. OSA adversely affects cardiac function through increased cardiac afterload [21], stimulation of sympathetic nerve activity [21], and induction of myocardial ischemia due to hypoxia [22]. In the early setting after STEMI, the heart may be vulnerable and susceptible to the adverse effects of OSA, including endothelial dysfunction and increased cardiac workload [23]. Indeed, previous studies have shown that patients with STEMI and OSA experience prolonged myocardial ischemia [24], less salvaged myocardium [3], and adverse LV remodeling [24] compared to those without OSA. These factors increase the risk of persistent LV dysfunction.
Our study showed that OAI was significantly associated with E/e’ at one week, which is the parameter of LV filling pressure. The association between OAI and E/e’ at seven months also approached significance (p = 0.057). A previous study demonstrated that obstructive apnea induces elevation of the LV filling pressure by increasing the LV afterload [25,26]. Increased LV wall stress induced by high LV filling pressure enhances myocardial cell death due to the architectural rearrangement of myocytes [27]. These results suggest that a continuous increase in LV wall stress caused by a high OAI may have induced persistent LV systolic dysfunction after STEMI.
In our study, OAI significantly correlated with a persistent decrease in LV-GLS. In contrast, CAI did not influence the LV-GLS. This mechanism can be explained as follows: the key pathophysiological differences between patients with CSA and OSA are reported to be negative intrathoracic pressure swings in the OSA group owing to respiratory effort against the occluded pharynx, raised blood pressure in the OSA cohort, and arousals [23]. In reality, increased LV transmural pressure in patients with OSA was reported to promote spherical cardiac remodeling and thinning of the LV wall in the region of the myocardial infarction [4]. Therefore, it is reasonable that OAI, but not CAI, is associated with persistent deterioration of LV function after STEMI.
Previous studies have shown mixed results on the relationship between the severity and classification of SDB and LV function after STEMIs, partly because of differences in the definition of SDB and the techniques for assessing cardiac function. Buchner et al. reported that patients with SDB had significantly lower LVEFs 3 months after the onset of STEMIs, as assessed by cardiac magnetic resonance imaging, than patients without SDB (LVEF = 48% vs. LVEF = 54%, p = 0.023) [3]. They reported that both OSA and CSA were associated with less myocardial salvage and a minor reduction in infarct size. However, in their study, the effects of OSA and CSA on LV functional recovery were not separately investigated. Additionally, LVEF, which is inferior to LV-GLS as a prognostic marker of STEMI, was used as a parameter for LV systolic function. Fisser et al. reported that increased LV transmural pressures in patients with OSA, but not in patients with CSA, may cause spherical cardiac remodeling and thinning of the LV wall [4]. Their study assessed spherical remodeling, calculated according to the sphericity index, by cardiac magnetic resonance imaging at baseline and three months after AMI. In contrast to CSA, OSA severity was independently associated with increased systolic sphericity index. Their results are consistent with ours in that only OSA, and not CSA, affects cardiac function. Our findings enhance the results of Fisser et al.’s study and provide a deeper understanding of the relationship between the OSA severity and LV functional recovery after STEMIs because we examined LV function using LV-GLS, the most promising marker of LV dysfunction and a superior predictor of outcome compared to the conventional LV functional parameters [8,9].
Previous studies have classified SDB according to the ratio of the central hypo-apnea index and obstructive hypo-apnea index to total AHI, and the influence of SDB on cardiac function was discussed by SDB classification (OSA-dominant or CSA-dominant) [3]. However, CSA and OSA can coexist [28,29]. In other words, even in patients classified as having CSA, the OAI may be high in some cases if the AHI is high. Therefore, to evaluate the relationship between SDB and STEMI, it may be beneficial to assess each apnea index rather than simply classify SDB into two types.
The results from the current study indicate that OAI influences LV function in the chronic phase after STEMI. A decreased LV systolic function during this phase could be a poor prognostic factor [30]. Hence, more aggressive treatment with high-dose renin-angiotensin system inhibitors, beta-blockers, or sodium-glucose cotransporter-2 inhibitors and closer follow-up of patients with high OAI early after the onset of STEMI may be required. In our study, AHI was also an independent factor associated with recovery and chronic-phase LV systolic dysfunction. However, measurement of AHI alone may not identify OAI, a potential therapeutic factor associated with cardiac dysfunction in AMI. Therefore, not only AHI but also CAI and OAI should be assessed separately in patients with STEMI.
Our results may have important implications when considering the indication for continuous positive airway pressure (CPAP) therapy in STEMI complicated by SDB. Determining the indications for CPAP during STEMI recovery is often difficult. Recent randomized controlled trials have failed to demonstrate the beneficial prognostic impact of CPAP treatment in the primary or secondary setting of AMI [31,32]. In the present study, we demonstrated that the OAI predicts impaired recovery of LV-GLS. This indicates that relief from OSA may have facilitated the recovery of LV function. CPAP treatment in patients with high OAI may improve LV function after STEMI.
Study Limitations
This study had several limitations. Firstly, this was a single-center retrospective study, and only patients experiencing a first STEMI who consented to a sleep study and for whom echocardiography could be performed in both the recovery and chronic phases were included. Therefore, the current study is limited by a small sample size. Thus, the potential relationship between CSA and cardiac function may not have been fully explored. However, our detailed analysis of the relationship between SDB and cardiac function using LV-GLS is novel and sets this study apart from its predecessors. We believe that further research involving a larger patient cohort is needed to investigate these associations. Secondly, our study showed that OAI was negatively associated with LV-GLS in both the recovery and chronic phases. However, OAI was not associated with LV-GLS recovery (Table 4). The study included patients eligible for a sleep study with no cardiovascular events up to the time of the chronic phase echocardiogram. Consequently, the patient cohort was small, and the infarct size was relatively modest. These factors may have prevented us from elucidating the relationship between sleep parameters and LV-GLS recovery in STEMI. Future studies involving larger patient populations may be able to investigate the relationship between sleep parameters and LV-GLS recovery in STEMI. Thirdly, all sleep studies were performed using Sleep Profiler rather than conventional polysomnography, the accepted gold standard for determining the presence and severity of SDB. Fourthly, since the Sleep Profiler cannot discriminate between obstructive hypopnea and central hypopnea, the classification was based on the percentage of the apnea index. The classification of hypopneas as central or obstructive is often difficult and has not been clearly defined in clinical studies [33]. Therefore, we believe that the fact that we were only able to examine obstructive and central apneas in this study does not diminish the significance of the study. However, for further understanding of the pathophysiology, it would be desirable to include hypopneas in future studies. Finally, because of this device limitation, we could not evaluate whether obstructive or hypopnea affected cardiac functions as obstructive apnea does.
5. Conclusions
OAI is associated with persistent LV dysfunction in patients with STEMI. Our findings would be beneficial for classifying more severely ill patients with STEMI at an early stage. Careful echocardiographic assessment and more aggressive treatment with medication should be provided to patients with STEMI and a higher OAI.
Author Contributions
N.I., T.I. and J.K. had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis, including any adverse effects. T.A., M.G., Y.H., M.H., K.O., Y.M., M.K., T.E. and K.H. contributed substantially to the study design, data analysis, interpretation, and manuscript writing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Human Ethics Review Board of Yokohama City University Medical Center (F221200035, 1 December 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lee, C.H.; Sethi, R.; Li, R.; Ho, H.H.; Hein, T.; Jim, M.H.; Loo, G.; Koo, C.Y.; Gao, X.F.; Chandra, S.; et al. Obstructive Sleep Apnea and Cardiovascular Events After Percutaneous Coronary Intervention. Circulation 2016, 133, 2008–2017. [Google Scholar] [CrossRef]
- Mazaki, T.; Kasai, T.; Yokoi, H.; Kuramitsu, S.; Yamaji, K.; Morinaga, T.; Masuda, H.; Shirai, S.; Ando, K. Impact of Sleep-Disordered Breathing on Long-Term Outcomes in Patients with Acute Coronary Syndrome Who Have Undergone Primary Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2016, 5, e003270. [Google Scholar] [CrossRef]
- Buchner, S.; Satzl, A.; Debl, K.; Hetzenecker, A.; Luchner, A.; Husser, O.; Hamer, O.W.; Poschenrieder, F.; Fellner, C.; Zeman, F.; et al. Impact of Sleep-Disordered Breathing on Myocardial Salvage and Infarct Size in Patients with Acute Myocardial Infarction. Eur. Heart J. 2014, 35, 192–199. [Google Scholar] [CrossRef]
- Fisser, C.; Götz, K.; Hetzenecker, A.; Debl, K.; Zeman, F.; Hamer, O.W.; Poschenrieder, F.; Fellner, C.; Stadler, S.; Maier, L.S.; et al. Obstructive Sleep Apnoea but Not Central Sleep Apnoea Is Associated with Left Ventricular Remodelling after Acute Myocardial Infarction. Clin. Res. Cardiol. 2021, 110, 971–982. [Google Scholar] [CrossRef]
- Florés, M.; de Batlle, J.; Sánchez-De-La-Torre, A.; Sánchez-De-La-Torre, M.; Aldomá, A.; Worner, F.; Galera, E.; Seminario, A.; Torres, G.; Dalmases, M.; et al. Central Sleep Apnoea Is Related to the Severity and Short-Term Prognosis of Acute Coronary Syndrome. PLoS ONE 2016, 11, e0167031. [Google Scholar] [CrossRef] [PubMed]
- Solin, P.; Bergin, P.; Richardson, M.; Kaye, D.M.; Walters, E.H.; Naughton, M.T. Influence of Pulmonary Capillary Wedge Pressure on Central Apnea in Heart Failure. Circulation 1999, 99, 1574–1579. [Google Scholar] [CrossRef]
- Resnick, H.E.; Redline, S.; Shahar, E.; Gilpin, A.; Newman, A.; Walter, R.; Ewy, G.A.; Howard, B.V.; Punjabi, N.M. Diabetes and Sleep Disturbances: Findings from the Sleep Heart Health Study. Diabetes Care 2003, 26, 702–709. [Google Scholar] [CrossRef]
- Stone, G.W.; Selker, H.P.; Thiele, H.; Patel, M.R.; Udelson, J.E.; Ohman, E.M.; Maehara, A.; Eitel, I.; Granger, C.B.; Jenkins, P.L.; et al. Relationship Between Infarct Size and Outcomes Following Primary PCI: Patient-Level Analysis from 10 Randomized Trials. J. Am. Coll. Cardiol. 2016, 67, 1674–1683. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, N.; Kirigaya, J.; Abe, T.; Horii, M.; Toya, N.; Hanajima, Y.; Takahashi, H.; Akiyama, E.; Okada, K.; Matsuzawa, Y.; et al. Impact of Three-Dimensional Global Longitudinal Strain for Patients with Acute Myocardial Infarction. Eur. Heart J. Cardiovasc. Imaging 2020, 22, 1413–1424. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Canali, E.; Petronilli, V.; Cicogna, F.; de Luca, L.; Francone, M.; Sardella, G.; Iacoboni, C.; Agati, L. Global and Regional Longitudinal Strain Assessed by Two-Dimensional Speckle Tracking Echocardiography Identifies Early Myocardial Dysfunction and Transmural Extent of Myocardial Scar in Patients with Acute ST Elevation Myocardial Infarction and Relatively Preserved LV Function. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 805–811. [Google Scholar] [CrossRef]
- Collier, P.; Phelan, D.; Klein, A. A Test in Context: Myocardial Strain Measured by Speckle-Tracking Echocardiography. J. Am. Coll. Cardiol. 2017, 69, 1043–1056. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth Universal Definition of Myocardial Infarction. J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Kimura, T.; Ishihara, M.; Nakagawa, Y.; Nakao, K.; Miyauchi, K.; Sakamoto, T.; Tsujita, K.; Hagiwara, N.; Miyazaki, S.; et al. JCS 2018 Guideline on Diagnosis and Treatment of Acute Coronary Syndrome. Circ. J. 2019, 83, 1085–1196. [Google Scholar] [CrossRef]
- Finan, P.H.; Richards, J.M.; Gamaldo, C.E.; Han, D.; Leoutsakos, J.M.; Salas, R.; Irwin, M.R.; Smith, M.T. Validation of a Wireless, Self-Application, Ambulatory Electroencephalographic Sleep Monitoring Device in Healthy Volunteers. J. Clin. Sleep Med. 2016, 12, 1443–1451. [Google Scholar] [CrossRef] [PubMed]
- Levendowski, D.J.; Ferini-Strambi, L.; Gamaldo, C.; Cetel, M.; Rosenberg, R.; Westbrook, P.R. The Accuracy, Night-to-Night Variability, and Stability of Frontopolar Sleep Electroencephalography Biomarkers. J. Clin. Sleep Med. 2017, 13, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Sakane, K.; Miyoshi, T.; Doi, M.; Hirohata, S.; Kaji, Y.; Kamikawa, S.; Ogawa, H.; Hatanaka, K.; Kitawaki, T.; Kusachi, S.; et al. Association of New Arterial Stiffness Parameter, the Cardio-Ankle Vascular Index, with Left Ventricular Diastolic Function. J. Atheroscler. Thromb. 2008, 15, 261–268. [Google Scholar] [CrossRef]
- Roman, M.J.; Ganau, A.; Saba, P.S.; Pini, R.; Pickering, T.G.; Devereux, R.B. Impact of Arterial Stiffening on Left Ventricular Structure. Hypertension 2000, 36, 489–494. [Google Scholar] [CrossRef]
- Usui, K.; Bradley, T.D.; Spaak, J.; Ryan, C.M.; Kubo, T.; Kaneko, Y.; Floras, J.S. Inhibition of Awake Sympathetic Nerve Activity of Heart Failure Patients with Obstructive Sleep Apnea by Nocturnal Continuous Positive Airway Pressure. J. Am. Coll. Cardiol. 2005, 45, 2008–2011. [Google Scholar] [CrossRef]
- Peled, N.; Abinader, E.G.; Pillar, G.; Sharif, D.; Lavie, P. Nocturnal Ischemic Events in Patients with Obstructive Sleep Apnea Syndrome and Ischemic Heart Disease: Effects of Continuous Positive Air Pressure Treatment. J. Am. Coll. Cardiol. 1999, 34, 1744–1749. [Google Scholar] [CrossRef]
- Hetzenecker, A.; Buchner, S.; Greimel, T.; Satzl, A.; Luchner, A.; Debl, K.; Husser, O.; Hamer, O.W.; Fellner, C.; Riegger, G.A.J.; et al. Cardiac Workload in Patients with Sleep-Disordered Breathing Early after Acute Myocardial Infarction. Chest 2013, 143, 1294–1301. [Google Scholar] [CrossRef]
- Nakashima, H.; Muto, S.; Amenomori, K.; Shiraishi, Y.; Nunohiro, T.; Suzuki, S. Impact of Obstructive Sleep Apnea on Myocardial Tissue Perfusion in Patients with ST-Segment Elevation Myocardial Infarction. Circ. J. 2011, 75, 890–896. [Google Scholar] [CrossRef]
- Arzt, M.; Hetzenecker, A.; Steiner, S.; Buchner, S. Sleep-Disordered Breathing and Coronary Artery Disease. Can. J. Cardiol. 2015, 31, 909–917. [Google Scholar] [CrossRef]
- Raut, S.; Gupta, G.; Narang, R.; Ray, A.; Pandey, R.M.; Malhotra, A.; Sinha, S. The Impact of Obstructive Sleep Apnoea Severity on Cardiac Structure and Injury. Sleep Med. 2021, 77, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Arzt, M.; Oldenburg, O.; Graml, A.; Schnepf, J.; Erdmann, E.; Teschler, H.; Schoebel, C.; Woehrle, H. Prevalence and Predictors of Sleep-Disordered Breathing in Chronic Heart Failure: The SchlaHF-XT Registry. ESC Heart Fail 2022, 9, 4100–4111. [Google Scholar] [CrossRef] [PubMed]
- Cheng, W.; Li, B.; Kajstura, J.; Li, P.; Wolin, M.S.; Sonnenblick, E.H.; Hintze, T.H.; Olivetti, G.; Anversa, P. Stretch-Induced Programmed Myocyte Cell Death. J. Clin. Investig. 1995, 96, 2247–2259. [Google Scholar] [CrossRef] [PubMed]
- Arzt, M.; Hetzenecker, A.; Lévy, P. Obstructive Sleep Apnoea in Acute Coronary Syndrome: The Invisible Threat? Eur. Respir. J. 2017, 49, 1602539. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.J.; Nothofer, G.; Priegnitz, C.; Anduleit, N.; Treml, M.; Kehl, V.; Galetke, W. Long-Term Auto-Servoventilation or Constant Positive Pressure in Heart Failure and Coexisting Central with Obstructive Sleep Apnea. Chest 2012, 142, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Pusalavidyasagar, S.S.; Olson, E.J.; Gay, P.C.; Morgenthaler, T.I. Treatment of Complex Sleep Apnea Syndrome: A Retrospective Comparative Review. Sleep Med. 2006, 7, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Chew, D.S.; Heikki, H.; Schmidt, G.; Kavanagh, K.M.; Dommasch, M.; Bloch Thomsen, P.E.; Sinnecker, D.; Raatikainen, P.; Exner, D.v. Change in Left Ventricular Ejection Fraction Following First Myocardial Infarction and Outcome. JACC Clin. Electrophysiol. 2018, 4, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-de-la-Torre, M.; Sánchez-de-la-Torre, A.; Bertran, S.; Abad, J.; Duran-Cantolla, J.; Cabriada, V.; Mediano, O.; Masdeu, M.J.; Alonso, M.L.; Masa, J.F.; et al. Effect of Obstructive Sleep Apnoea and Its Treatment with Continuous Positive Airway Pressure on the Prevalence of Cardiovascular Events in Patients with Acute Coronary Syndrome (ISAACC Study): A Randomised Controlled Trial. Lancet Respir. Med. 2020, 8, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Peker, Y.; Glantz, H.; Eulenburg, C.; Wegscheider, K.; Herlitz, J.; Thunström, E. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Disease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am. J. Respir. Crit. Care Med. 2016, 194, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Javaheri, S.; Rapoport, D.M.; Schwartz, A.R. Distinguishing central from obstructive hypopneas on a clinical polysomnogram. J. Clin. Sleep Med. 2023, 19, 823–834. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).