
Associating Appendicitis with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Novel Insight into an Unexpected Connection


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
2.3. Study Outcomes and Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Sample
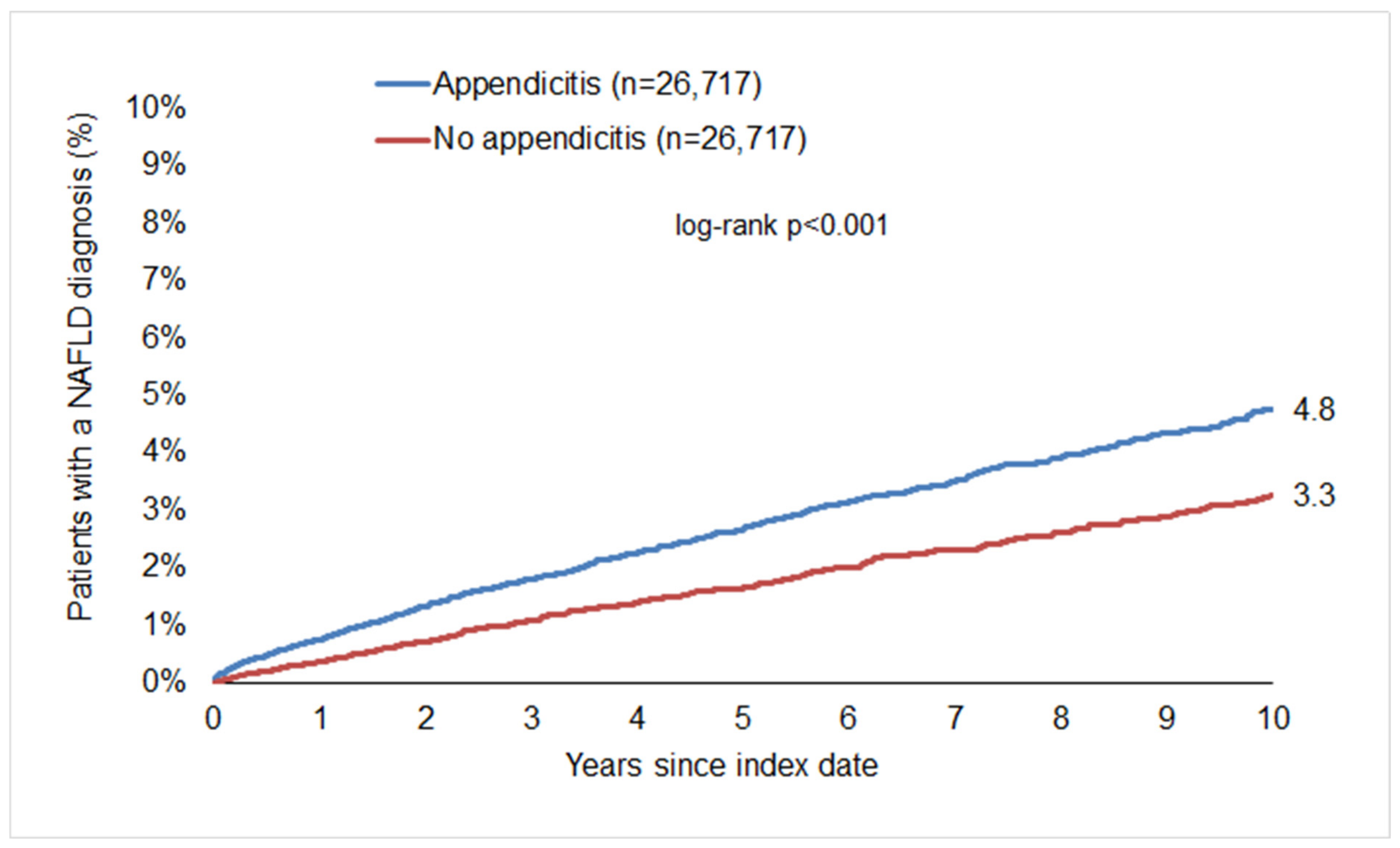
3.2. Association of Appendicitis with a Subsequent Diagnosis of MASLD
3.3. Age- and Sex-Stratified Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lang, S.; Farowski, F.; Martin, A.; Wisplinghoff, H.; Vehreschild, M.J.G.T.; Krawczyk, M.; Nowag, A.; Kretzschmar, A.; Scholz, C.; Kasper, P.; et al. Prediction of Advanced Fibrosis in Non-Alcoholic Fatty Liver Disease Using Gut Microbiota-Based Approaches Compared with Simple Non-Invasive Tools. Sci. Rep. 2020, 10, 9385. [Google Scholar] [CrossRef]
- Demir, M.; Lang, S.; Martin, A.; Farowski, F.; Wisplinghoff, H.; Vehreschild, M.J.G.T.; Krawczyk, M.; Nowag, A.; Scholz, C.J.; Kretzschmar, A.; et al. Phenotyping Non-Alcoholic Fatty Liver Disease by the Gut Microbiota: Ready for Prime Time? J. Gastroenterol. Hepatol. 2020, 35, 1969–1977. [Google Scholar] [CrossRef]
- Demir, M.; Lang, S.; Hartmann, P.; Duan, Y.; Martin, A.; Miyamoto, Y.; Bondareva, M.; Zhang, X.; Wang, Y.; Kasper, P.; et al. The Fecal Mycobiome in Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2022, 76, 788–799. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; Vigliotti, C.; Witjes, J.; Le, P.; Holleboom, A.G.; Verheij, J.; Nieuwdorp, M.; Clément, K. Gut Microbiota and Human NAFLD: Disentangling Microbial Signatures from Metabolic Disorders. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 279–297. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute Appendicitis: Modern Understanding of Pathogenesis, Diagnosis, and Management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Téoule, P.; de Laffolie, J.; Rolle, U.; Reißfelder, C. Acute Appendicitis in Childhood and Adolescence-an Everyday Clinical Challenge. Dtsch Arztebl Int 2020. Dtsch. Arztebl. Int. 2020, 117, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Di Mitri, M.; Parente, G.; Bonfiglioli, G.; Thomas, E.; Bisanti, C.; Cordola, C.; Vastano, M.; Cravano, S.; Collautti, E.; Di Carmine, A.; et al. IL-6 Serum Levels Can Enhance the Diagnostic Power of Standard Blood Tests for Acute Appendicitis. Childrens 2022, 9, 1425. [Google Scholar] [CrossRef]
- Mcgowan, D.R.; Sims, H.M.; Zia, K.; Uheba, M.; Shaikh, I.A. The Value of Biochemical Markers in Predicting a Perforation in Acute Appendicitis. ANZ J. Surg. 2013, 83, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Giordano, S.; Pääkkönen, M.; Salminen, P.; Grönroos, J.M. Elevated Serum Bilirubin in Assessing the Likelihood of Perforation Inacute Appendicitis: A Diagnostic Meta-Analysis. Int. J. Surg. 2013, 11, 795–800. [Google Scholar] [CrossRef]
- Song, M.Y.; Ullah, S.; Yang, H.Y.; Ahmed, M.R.; Saleh, A.A.; Liu, B.R. Long-Term Effects of Appendectomy in Humans: Is It the Optimal Management of Appendicitis? Expert. Rev. Gastroenterol. Hepatol. 2021, 15, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jang, E.J.; Jo, J.; Park, S.J.; Ryu, H.G. Long-Term Impacts of Appendectomy Associated with Increased Incidence of Inflammatory Bowel Disease, Infection, and Colorectal Cancer. Int. J. Color. Dis. 2021, 36, 1643–1652. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, T.; Fonnes, S.; Rosenberg, J. Long-Term Complications of Appendectomy: A Systematic Review. Scand. J. Surg. 2018, 107, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Girard-Madoux, M.J.H.; Gomez de Agüero, M.; Ganal-Vonarburg, S.C.; Mooser, C.; Belz, G.T.; Macpherson, A.J.; Vivier, E. The Immunological Functions of the Appendix: An Example of Redundancy? Semin. Immunol. 2018, 36, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Heindl, S.E.; Tsouklidis, N. Appendectomy as a Potential Predisposing Factor for the Development of Recurrent and Fulminant Clostridium Difficile. Cureus 2020, 12, e10091. [Google Scholar] [CrossRef]
- Jördens, M.S.; Luedde, M.; Roderburg, C.; Demir, M.; Luedde, T.; Kostev, K.; Loosen, S.H. Pulmonary Hypertension Is Associated with an Increased Incidence of NAFLD: A Retrospective Cohort Study of 18,910 Patients. J. Intern. Med. 2021, 290, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Kostev, K.; Keitel, V.; Tacke, F.; Roderburg, C.; Luedde, T. An Elevated FIB-4 Score Predicts Liver Cancer Development: A Longitudinal Analysis from 29,999 NAFLD Patients. J. Hepatol. 2021, 76, 247–248. [Google Scholar] [CrossRef]
- Labenz, C.; Huber, Y.; Michel, M.; Nagel, M.; Galle, P.R.; Kostev, K.; Schattenberg, J.M. Impact of NAFLD on the Incidence of Cardiovascular Diseases in a Primary Care Population in Germany. Dig. Dis. Sci. 2020, 65, 2112–2119. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Nakano, M.; Murohisa, T.; Imai, Y.; Tamano, M.; Hiraishi, H. Association Between Appendectomy and Fibrosis Progression in Nonalcoholic Fatty Liver Disease. Gastroenterol. Res. 2013, 6, 17–25. [Google Scholar] [CrossRef]
- Andreu-Ballester, J.C.; Pérez-Griera, J.; Ballester, F.; Colomer-Rubio, E.; Ortiz-Tarín, I.; Peñarroja Otero, C. Secretory Immunoglobulin A (SIgA) Deficiency in Serum of Patients with GALTectomy (Appendectomy and Tonsillectomy). Clin. Immunol. 2007, 123, 289–297. [Google Scholar] [CrossRef]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Prior to Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Variable | Proportion Among Appendicitis Patients (n, %) n = 27,052 | Proportion Among Non-Appendicitis Patients (n, %) n = 3,118,063 | p-Value | Proportion among Appendicitis Patients (n, %) n = 26,717 | Proportion Among Non-Appendicitis Patients (n, %) n = 26,717 | p-Value |
| Age (Mean, SD) | 40.6 (17.9) | 51.6 (19.5) | <0.001 | 40.5 (17.9) | 40.6 (17.9) | 0.855 |
| Age 18–30 | 10,264 (37.9) | 561,734 (18.0) | 10,155 (38.0) | 10,082 (37.7) | 0.926 | |
| Age 31–40 | 4758 (17.6) | 452,655 (14.5) | 4687 (17.5) | 4760 (17.8) | ||
| Age 41–50 | 4767 (15.4) | 484,665 (15.5) | <0.001 | 4185 (15.4) | 4128 (15.5) | |
| Age 51–60 | 3640 (13.5) | 547,496 (17.6) | 3609 (13.5) | 3592 (13.4) | ||
| Age > 60 | 4223 (15.6) | 1,071,513 (34.4) | 4141 (15.5) | 4155 (15.6) | ||
| Female | 15,149 (56.0) | 1,677,793 (53.8) | <0.001 | 14,950 (56.0) | 14,906 (55.8) | 0.702 |
| Male | 11,903 (44.0) | 1,440,270 (46.2) | 11,767 (44.0) | 11,811 (44.2) | ||
| Obesity diagnosis | 2179 (8.1) | 245,839 (7.9) | 0.300 | 1994 (7.5) | 1982 (7.4) | 0.843 |
| Number of physician visits per year during the follow-up (Mean, SD) | 6.0 (3.9) | 5.7 (4.3) | <0.001 | 6.0 (3.9) | 6.0 (3.9) | 1.000 |
| Charlson Comorbidity Score (CCS) (Mean, SD) | 1.1 (1.6) | 1.4 (1.9) | <0.001 | 1.0 (1.5) | 1.0 (1.5) | 0.439 |
| CCS 0 | 12,459 (46.1) | 1,306,208 (41.9) | 12,418 (46.5) | 12,522 (46.9) | 0.918 | |
| CCS 1 | 8081 (29.9) | 811,788 (26.0) | 8043 (30.1) | 7963 (29.8) | ||
| CCS 2 | 3173 (11.7) | 412,356 (13.1) | <0.001 | 3128 (11.7) | 3129 (11.7) | |
| CCS 3 | 1510 (5.6) | 235,214 (7.5) | 1471 (5.5) | 1464 (5.5) | ||
| CCS > 3 | 1829 (6.8) | 352,497 (11.3) | 1657 (6.2) | 1639 (6.1) | ||
| Index year 2005–2008 | 2751 (10.2) | 282,330 (9.1) | 2683 (10.0) | 2704 (10.1) | 0.127 | |
| Index year 2009–2012 | 4894 (18.1) | 391,249 (12.5) | 4787 (17.9) | 4699 (17.6) | ||
| Index year 2013–2016 | 7133 (26.4) | 661,754 (21.2) | <0.001 | 7035 (26.3) | 6855 (25.7) | |
| Index year 2017–2021 | 12,274 (45.3) | 1,782,730 (57.2) | 12,212 (45.7) | 12,459 (46.6) | ||
| Patient Group | Incidence (Cases per 1000 Patient Years) in the Appendicitis Cohort | Incidence (Cases per 1000 Patient Years) in the Non-Appendicitis Cohort | HR (95% CI) | p-Value |
|---|---|---|---|---|
| Total | 5.4 | 3.5 | 1.57 (1.39–1.78) | <0.001 |
| Age 18–30 | 2.1 | 1.4 | 1.42 (1.02–1.96) | 0.035 |
| Age 31–40 | 5.3 | 3.0 | 1.75 (1.29–2.38) | <0.001 |
| Age 41–50 | 7.2 | 4.7 | 1.54 (1.20–1.98) | <0.001 |
| Age 51–60 | 9.4 | 5.7 | 1.67 (1.30–2.14) | <0.001 |
| Age ≥ 60 | 7.4 | 5.1 | 1.53 (1.18–1.99) | 0.002 |
| Female | 4.7 | 2.7 | 1.74 (1.46–2.09) | <0.001 |
| Male | 6.2 | 4.4 | 1.44 (1.22–1.70) | <0.001 |
| Obesity | 14.1 | 9,2 | 1.58 (1.19–2.10) | 0.002 |
| No obesity | 4.7 | 3.0 | 1.57 (1.37–1.80) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roderburg, C.; Waldschmidt, D.; Leyh, C.; Krieg, S.; Krieg, A.; Luedde, T.; Loosen, S.H.; Kostev, K. Associating Appendicitis with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Novel Insight into an Unexpected Connection. J. Clin. Med. 2024, 13, 1319. https://doi.org/10.3390/jcm13051319
Roderburg C, Waldschmidt D, Leyh C, Krieg S, Krieg A, Luedde T, Loosen SH, Kostev K. Associating Appendicitis with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Novel Insight into an Unexpected Connection. Journal of Clinical Medicine. 2024; 13(5):1319. https://doi.org/10.3390/jcm13051319
Chicago/Turabian StyleRoderburg, Christoph, Dirk Waldschmidt, Catherine Leyh, Sarah Krieg, Andreas Krieg, Tom Luedde, Sven H. Loosen, and Karel Kostev. 2024. "Associating Appendicitis with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Novel Insight into an Unexpected Connection" Journal of Clinical Medicine 13, no. 5: 1319. https://doi.org/10.3390/jcm13051319
APA StyleRoderburg, C., Waldschmidt, D., Leyh, C., Krieg, S., Krieg, A., Luedde, T., Loosen, S. H., & Kostev, K. (2024). Associating Appendicitis with Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD): A Novel Insight into an Unexpected Connection. Journal of Clinical Medicine, 13(5), 1319. https://doi.org/10.3390/jcm13051319