
Outcomes of Severe ARDS COVID-19 Patients Denied for Venovenous ECMO Support: A Prospective Observational Comparative Study
 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Decision-Making Process, ECMO Criteria, and Initial ECMO Management
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
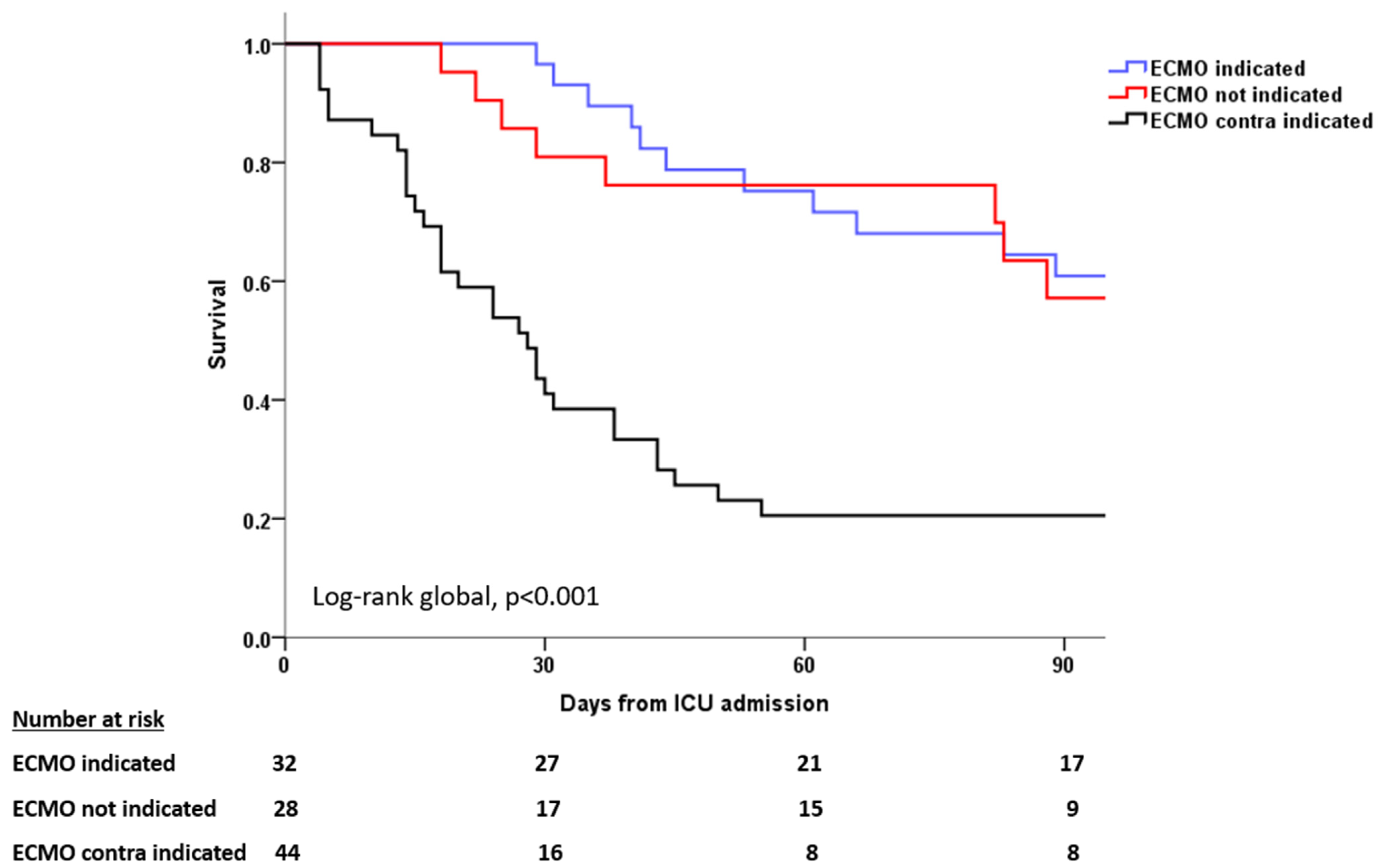
3.2. Outcomes and Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | acute respiratory distress syndrome |
| COVID-19 | coronavirus disease 2019 |
| ELSO | extracorporeal life support organization |
| ICU | intensive care unit |
| IQR | inter quartile range |
| NMBA | neuromuscular blocking agents |
| PEEP | positive end-expiratory pressure |
| P/F ratio | PaO2 to FiO2 ratio |
| RS | respiratory system |
| SOFA score | sequential organ failure assessment score |
| VV-ECMO | venovenous extracorporeal membrane oxygenation |
References
- Extracorporeal Membrane Oxygenation|ECMO. Extracorporeal Membrane Oxygenation (ECMO) in COVID-19. Available online: https://www.elso.org/covid-19.aspx (accessed on 1 December 2023).
- Tran, A.; Fernando, S.M.; Rochwerg, B.; Barbaro, R.P.; Hodgson, C.L.; Munshi, L.; MacLaren, G.; Ramanathan, K.; Hough, C.L.; Brochard, L.J.; et al. Prognostic factors associated with mortality among patients receiving venovenous extracorporeal membrane oxygenation for COVID-19: A systematic review and meta-analysis. Lancet Respir. Med. 2023, 11, 235–244. [Google Scholar] [CrossRef]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Parzy, G.; Daviet, F.; Puech, B.; Sylvestre, A.; Guervilly, C.; Porto, A.; Hraiech, S.; Chaumoitre, K.; Papazian, L.; Forel, J.M. Venous Thromboembolism Events Following Venovenous Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Syndrome Coronavirus 2 Based on CT Scans. Crit. Care Med. 2020, 48, e971–e975. [Google Scholar] [CrossRef] [PubMed]
- Vaquer, S.; de Haro, C.; Peruga, P.; Oliva, J.C.; Artigas, A. Systematic review and meta-analysis of complications and mortality of veno-venous extracorporeal membrane oxygenation for refractory acute respiratory distress syndrome. Ann. Intensive Care 2017, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- Chommeloux, J.; Valentin, S.; Winiszewski, H.; Adda, M.; Pineton de Chambrun, M.; Moyon, Q.; Mathian, A.; Capellier, G.; Guervilly, C.; Levy, B.; et al. One-Year Mental and Physical Health Assessment in Survivors After ECMO for COVID-19-related ARDS. Am. J. Respir. Crit. Care Med. 2022, 207, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Puri, N.; Damuth, E.; Potestio, C.; Peterson, L.N.; Ledane, J.; Rackley, C.R.; King, C.S.; Conrad, S.A.; Green, A. Extracorporeal Membrane Oxygenation for COVID-19: Comparison of Outcomes to Non-COVID-19-Related Viral Acute Respiratory Distress Syndrome from the Extracorporeal Life Support Organization Registry. Crit. Care Explor. 2023, 5, e0861. [Google Scholar] [CrossRef] [PubMed]
- Supady, A.; DellaVolpe, J.; Taccone, F.S.; Scharpf, D.; Ulmer, M.; Lepper, P.M.; Halbe, M.; Ziegeler, S.; Vogt, A.; Ramanan, R.; et al. Outcome Prediction in Patients with Severe COVID-19 Requiring Extracorporeal Membrane Oxygenation—A Retrospective International Multicenter Study. Membranes 2021, 11, 170. [Google Scholar] [CrossRef] [PubMed]
- Gannon, W.D.; Stokes, J.W.; Gong, W.; Lindsell, C.J.; Tonna, J.E.; Bacchetta, M.; Rice, T.W.; Semler, M.W.; Casey, J.D. Predicting Mortality for Patients Eligible for Extracorporeal Membrane Oxygenation for COVID-19. Am. J. Respir. Crit. Care Med. 2022, 206, 628–632. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Guervilly, C.; Bousquet, G.; Arnaud, L.; Gragueb-Chatti, I.; Daviet, F.; Adda, M.; Forel, J.M.; Dignat-George, F.; Papazian, L.; Roch, A.; et al. Microvesicles Are Associated with Early Veno Venous ECMO Circuit Change during Severe ARDS: A Prospective Observational Pilot Study. J. Clin. Med. 2023, 12, 7281. [Google Scholar] [CrossRef] [PubMed]
- Gillon, S.A.; Rowland, K.; Shankar-Hari, M.; Camporota, L.; Glover, G.W.; Wyncoll, D.L.A.; Barrett, N.A.; Ioannou, N.; Meadows, C.I.S. Acceptance and transfer to a regional severe respiratory failure and veno-venous extracorporeal membrane oxygenation (ECMO) service: Predictors and outcomes. Anaesthesia 2018, 73, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Lebreton, G.; Pineton de Chambrun, M.; Hékimian, G.; Chommeloux, J.; Bréchot, N.; Luyt, C.-E.; Leprince, P.; Combes, A.; Schmidt, M. Outcomes of Patients Denied ECMO During the COVID-19 Pandemic in Greater Paris, France. Am. J. Respir. Crit. Care Med. 2021, 204, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Landoll, M.; Pequignot, B.; Langouet, E.; Amalric, M.; Mekontso-Dessap, A.; Chiscano-Camon, L.; Surman, K.; Finnerty, D.; et al. Comparative outcomes of extracorporeal membrane oxygenation for COVID-19 delivered in experienced European centres during successive SARS-CoV-2 variant outbreaks (ECMO-SURGES): An international, multicentre, retrospective cohort study. Lancet Respir. Med. 2023, 11, 163–175, Erratum in Lancet Respir. Med. 2023, 11, E25. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Dres, M.; Guervilly, C.; Richard, J.C.; Sonneville, R.; Winiszewski, H.; Muller, G.; Beduneau, G.; et al. Prone Positioning During Extracorporeal Membrane Oxygenation in Patients with Severe ARDS: The PRONECMO Randomized Clinical Trial. JAMA 2023, 330, 2343–2353. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Zogheib, E.; Rozé, H.; Repesse, X.; Lebreton, G.; Luyt, C.E.; Trouillet, J.L.; Bréchot, N.; Nieszkowska, A.; Dupont, H.; et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013, 39, 1704–1713. [Google Scholar] [CrossRef]
- Schmidt, M.; Bailey, M.; Sheldrake, J.; Hodgson, C.; Aubron, C.; Rycus, P.T.; Scheinkestel, C.; Cooper, D.J.; Brodie, D.; Pellegrino, V.; et al. Predicting Survival after Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) Score. Am. J. Respir. Crit. Care Med. 2014, 189, 1374–1382. [Google Scholar] [CrossRef]
- Pappalardo, F.; Pieri, M.; Greco, T.; Patroniti, N.; Pesenti, A.; Arcadipane, A.; Ranieri, V.M.; Gattinoni, L.; Landoni, G.; Holzgraefe, B.; et al. Predicting mortality risk in patients undergoing venovenous ECMO for ARDS due to influenza A (H1N1) pneumonia: The ECMOnet score. Intensive Care Med. 2013, 39, 275–281. [Google Scholar] [CrossRef]
- Pratt, E.H.; Morrison, S.; Green, C.L.; Rackley, C.R. Ability of the respiratory ECMO survival prediction (RESP) score to predict survival for patients with COVID-19 ARDS and non-COVID-19 ARDS: A single-center retrospective study. J. Intensive Care 2023, 11, 37. [Google Scholar] [CrossRef]
- Provaznik, Z.; Philipp, A.; Müller, T.; Kostiantyn, K.; Lunz, D.; Schmid, C.; Floerchinger, B. Outcome after veno-venous extracorporeal membrane oxygenation in elderly compared to younger patients: A 14-year retrospective observational study. Artif. Organs 2023, 47, 882–890. [Google Scholar] [CrossRef]
- Deatrick, K.B.; Mazzeffi, M.A.; Galvagno, S.M., Jr.; Tesoriero, R.B.; Kaczoroswki, D.J.; Herr, D.L.; Dolly, K.; Rabinowitz, R.P.; Scalea, T.M.; Menaker, J. Outcomes of Venovenous Extracorporeal Membrane Oxygenation When Stratified by Age: How Old Is Too Old? ASAIO J. 2020, 66, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Strassmann, S.; Merten, M.; Bein, T.; Windisch, W.; Meybohm, P.; Weber-Carstens, S. High In-Hospital Mortality Rate in Patients with COVID-19 Receiving Extracorporeal Membrane Oxygenation in Germany: A Critical Analysis. Am. J. Respir. Crit. Care Med. 2021, 204, 991–994. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, R.H.; Ogino, M.T.; Brodie, D.; McMullan, D.M.; Lorusso, R.; MacLaren, G.; Stead, C.M.; Rycus, P.; Fraser, J.F.; Belohlavek, J.; et al. Initial ELSO guidance document: ECMO for COVID-19 patients with severe cardiopulmonary failure. ASAIO J. 2020, 66, 472–474. [Google Scholar] [CrossRef] [PubMed]
- Hermann, M.; Laxar, D.; Krall, C.; Hafner, C.; Herzog, O.; Kimberger, O.; Koenig, S.; Kraft, F.; Maleczek, M.; Markstaller, K.; et al. Duration of invasive mechanical ventilation prior to extracorporeal membrane oxygenation is not associated with survival in acute respiratory distress syndrome caused by coronavirus disease 2019. Ann. Intensive Care 2022, 12, 6. [Google Scholar] [CrossRef]
- Snyder, M.; Njie, B.Y.; Grabenstein, I.; Viola, S.; Abbas, H.; Bhatti, W.; Lee, R.; Traficante, R.; Yeung, S.Y.A.; Chow, J.H.; et al. Functional recovery in a cohort of ECMO and non-ECMO acute respiratory distress syndrome survivors. Crit. Care 2023, 27, 440. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| VV-ECMO Indicated (n = 32) | VV-ECMO Not Indicated (n = 28) | VV-ECMO Contra-Indicated (n = 44) | p | |
|---|---|---|---|---|
| Age, years | 59 (55–62) | 53 (47–60) | 66 (60–69) | <0.001 |
| Male | 29 (90) | 19 (68) | 36 (82) | 0.08 |
| Body mass index, kg/m2 | 30.9 (25.7–33.7) | 30.1 (27.1–35.0) | 28.7 (26.1–36.7) | 0.97 |
| Comorbidities | ||||
| Hypertension | 13 (40) | 8 (28) | 19 (43) | 0.44 |
| Diabetes | 9 (28) | 7 (25) | 19 (43) | 0.20 |
| Chronic lung disease | 8 (25) | 3 (11) | 9 (20) | 0.36 |
| Cardiomyopathy | 4 (12) | 4 (14) | 9(20) | 0.61 |
| Immunocompromised | 4 (12) | 1 (4) | 3 (7) | 0.41 |
| SOFA score at call | 6 (4–8) | 4 (4–7) | 7 (4–8) | 0.01 |
| Duration of mechanical ventilation prior call, days | 4.5 (1–7) | 2.5 (1–7) | 7 (3–17) | 0.002 |
| Respiratory parameters at time of call | ||||
| FiO2, % | 100 (100–100) | 80 (70–100) | 100 (85–100) | <0.001 |
| PEEP, cmH2O | 12 (10–15) | 12 (10–14) | 10 (9–14) | 0.17 |
| Tidal volume, mL/kg/PBW | 6.2 (5.5–6.8) | 6.1 (5.8–6.7) | 6.1 (5.8–6.7) | 0.68 |
| Respiratory rate, cycles/min | 30 (24–32) | 28 (22–29) | 30 (26–32) | 0.01 |
| Plateau pressure, cmH2O | 32 (27–35) | 30 (25–32) | 30 (28–31) | 0.25 |
| Driving pressure, cmH2O | 17 (13–24) | 16 (13–21) | 19 (15–22) | 0.32 |
| RS static compliance, mL/cmH2O | 25 (17–28) | 25 (17–32) | 20 (16–25) | 0.09 |
| Arterial blood gas at time of call | ||||
| pH | 7.29 (7.25–7.36) | 7.38 (7.33–7.45) | 7.31 (7.25–7.39) | 0.001 |
| PaO2:FiO2, mmHg | 71 (56–84) | 100 (75–130) | 70 (61–91) | 0.004 |
| PaCO2, mmHg | 60 (56–72) | 53 (45–60) | 63 (56–67) | 0.001 |
| Lactates, mmol/L | 1.5 (1–2.75) | 1.4 (1.1–1.7) | 1.5 (1–2) | 0.84 |
| Concomitant or prior treatments at time of call | ||||
| Continuous NMBA infusion | 32(100) | 28 (100) | 44 (100) | - |
| Prone positioning | 31 (97) | 28 (100) | 43 (98) | 0.66 |
| Number of prone positioning sessions | 2 (1–4) | 1 (1–3) | 3 (1–4) | 0.15 |
| Inhaled nitric oxide | 21 (65) | 14 (50) | 28 (64) | 0.36 |
| Almitrine infusion | 3 (9) | 0 (0) | 5 (11) | 0.18 |
| Vasopressor infusion | 15 (47) | 10 (37) | 20 (45) | 0.63 |
| Renal replacement therapy | 2 (6) | 1 (3) | 4 (9) | 0.65 |
| VV-ECMO Indicated | VV-ECMO Not Indicated | VV-ECMO Contra–Indicated | p | |
|---|---|---|---|---|
| Death by day 60, n (%) n = 94 | 10 (32.3) | 7 (31.8) | 31 (75.6) | <0.001 |
| Lost of follow up by day 60, n (%) n = 10 | 1 (3.1) | 6 (21.4) | 3 (6.8) | 0.04 |
| Death by day 90, n (%) n = 89 | 11 (37.9) | 8 (38.1) | 31 (79.5) | <0.001 |
| Lost of follow up by day 90, n (%) n = 15 | 3 (9.4) | 7 (25) | 5 (11.4) | 0.17 |
| Withdraw life-sustaining therapy, n (%) n = 102 | 10 (31.2) | 2 (7.4) | 13 (30.2) | 0.055 |
| Duration of mechanical ventilation, days n = 99 | 39 (25–53) | 20 (12–46) | 23 (8–39) | 0.002 |
| Duration of ICU stay, days n = 100 | 53 (31–66) | 29 (22–61) | 29 (14–46) | 0.001 |
| Duration of hospital stays, days n = 93 | 66 (38–83) | 36 (24–59) | 29 (15–49) | <0.001 |
| Last follow up n = 46 | 0.023 | |||
| At home | 14 (78) | 9 (56) | 6 (50) | |
| Rehabilitation center | 4 (22) | 3 (18) | 6 (50) | |
| Still in ICU/Mechanical ventilation weaning unit | 0 (0) | 4 (25) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sylvestre, A.; Forel, J.-M.; Textoris, L.; Gragueb-Chatti, I.; Daviet, F.; Salmi, S.; Adda, M.; Roch, A.; Papazian, L.; Hraiech, S.; et al. Outcomes of Severe ARDS COVID-19 Patients Denied for Venovenous ECMO Support: A Prospective Observational Comparative Study. J. Clin. Med. 2024, 13, 1493. https://doi.org/10.3390/jcm13051493
Sylvestre A, Forel J-M, Textoris L, Gragueb-Chatti I, Daviet F, Salmi S, Adda M, Roch A, Papazian L, Hraiech S, et al. Outcomes of Severe ARDS COVID-19 Patients Denied for Venovenous ECMO Support: A Prospective Observational Comparative Study. Journal of Clinical Medicine. 2024; 13(5):1493. https://doi.org/10.3390/jcm13051493
Chicago/Turabian StyleSylvestre, Aude, Jean-Marie Forel, Laura Textoris, Ines Gragueb-Chatti, Florence Daviet, Saida Salmi, Mélanie Adda, Antoine Roch, Laurent Papazian, Sami Hraiech, and et al. 2024. "Outcomes of Severe ARDS COVID-19 Patients Denied for Venovenous ECMO Support: A Prospective Observational Comparative Study" Journal of Clinical Medicine 13, no. 5: 1493. https://doi.org/10.3390/jcm13051493
APA StyleSylvestre, A., Forel, J.-M., Textoris, L., Gragueb-Chatti, I., Daviet, F., Salmi, S., Adda, M., Roch, A., Papazian, L., Hraiech, S., & Guervilly, C. (2024). Outcomes of Severe ARDS COVID-19 Patients Denied for Venovenous ECMO Support: A Prospective Observational Comparative Study. Journal of Clinical Medicine, 13(5), 1493. https://doi.org/10.3390/jcm13051493