1. Introduction
Left bundle branch area pacing (LBBAP) has developed rapidly over the last few years. The feasibility and safety of this promising pacing modality have been shown not only in small to medium studies [
1,
2,
3,
4] but also in large multicenter registers [
5]. The main advantage of LBBAP is the provision of better ventricular synchrony than in conventional right ventricular pacing (RVP) [
6]. The superior outcomes of LBBAP compared to RVP in heart failure hospitalization and all-cause mortality rates, as well as in various parameters of cardiac function, have been shown in a few studies [
7,
8,
9]. The mechanism underlying these results is fast activation of the left ventricle by left bundle branch (LBB) fibres or via quick capture of the left side of the septal myocardium. This may not only prevent the development of pacing-induced cardiomyopathy [
10,
11], but may also improve ventricular synchrony, restoring impaired conduction in patients with left bundle branch block (LBBB). Individuals with right bundle branch block (RBBB) may benefit from a reduction in right ventricular activation delay due to the capture of the septal myocardium. These resynchronizing effects ensure the efficacy of LBBAP in cardiac resynchronization therapy (CRT). Improvement in the NYHA functional class, left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD) and left ventricular volumes have been shown in recent studies [
12,
13,
14,
15,
16]. However, detailed data on the impact of LBBAP on the parameters of cardiac function in bradycardia patients, especially with preserved LVEF, as well as on some follow-up issues, are still limited.
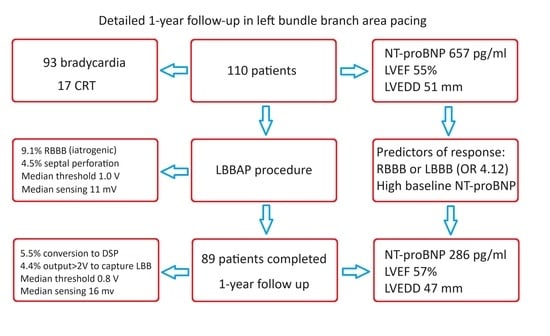
The aim of this study was to evaluate LBBAP during a one-year observation period. We assessed echocardiographic response, changes in the N-terminal prohormone of the brain natriuretic peptide (NT-proBNP) serum level and electrical parameters. Moreover, we indicated the factors associated with better outcomes in heart function parameters. Furthermore, we conducted a detailed analysis of acute and follow-up complications and conditions that required special attention or management.
2. Materials and Methods
2.1. Study Design and Population
The studied population consisted of 110 patients who underwent successful LBBAP device implantation between March 2021 and June 2022. No preselection was applied—LBBAP was performed as the primary approach for all pacing indications. There were no exclusion criteria besides the inability to achieve LBBAP. All consecutive patients who had received an LBBAP device and had been operated on by the authors within the indicated period of time were included in the study. Patients were observed for a one-year period. Outpatient control visits were performed 1, 6 and 12 months after implantation.
2.2. LBBAP Lead Implantation
A lumenless (SelectSecure 3830, Medtronic, Minneapolis, MN, USA) lead was delivered by a corresponding fixed shape catheter (C315-HIS, Medtronic) to the right ventricle and allocated towards the interventricular septum. The initial position was determined using fluoroscopy and pace mapping. Regarding fluoroscopy, we used a simplified method similar to Zhang et al., targeting a wide area of the septum from approximately 2 cm behind the tricuspid summit to about half of the distance to the apex [
17]. To confirm the appropriate position, unipolar tip pacing was performed—we followed the criterion of QRS polarity discordance in leads aVL (positive) and aVR (negative). Recording of the His bundle potential was not required. After determining the initial site, lead rotations were started. The depth of the penetration was monitored by observation of fixation beats [
18] and we repeated the unipolar tip pacing until the terminal R-wave in lead V1 appeared. Electrocardiographic and electrical measurements were then performed. If the parameters were acceptable, the delivery catheter was removed.
2.3. Device Programming
The pacemakers were programmed conventionally with a few exceptions. Firstly, decisions on whether to promote intrinsic conduction or ventricular pacing in patients with preserved atrioventricular conduction were individualized. In patients with a narrow native QRS complex and normal PR interval, longer AV delays were set to avoid pacing. In individuals with bundle branch block or a prolonged PR interval, we programmed short AV delays to achieve the resynchronization effect. Secondly, in the case of dissimilarity in the capture thresholds of the septal myocardium and LBB, the ventricular output was set manually to ensure conduction system capture or minimum adapted amplitude was increased accordingly. The CRT devices were programmed individually to achieve maximal narrowing of the QRS complexes. This included adjustment of the AV delay and choosing a bipolar (to achieve anodal capture) or unipolar configuration of the LBBAP lead. In the case of a prominent RBBB pattern during LBBAP, additional pacing from the right ventricular lead was used.
2.4. Data Collection
Echocardiography and NT-proBNP serum level measurement were performed prior to implantation and 12 months after the procedure (at the third control visit). Vivid T8 and T9 (GE Healthcare, Chicago, IL, USA) ultrasound machines were used. To assess the echocardiographic response, LVEF, LVEDD and left atrial dimension (LAD) were measured in a two-dimensional presentation. We also assessed the distance from the base of the anterior mitral cusp to the tip of the LBBAP lead in an apical four-chamber view. Heart function response was defined as meeting at least two of the following criteria: (1) a reduction of at least 50% in the NT-proBNP level, (2) an increase of at least 5 percentage points in LVEF, (3) a decrease of at least 5 mm in LVEDD and (4) a decrease of at least 5 mm in LAD.
Standard electrical parameters (capture threshold, sensing and impedance) were measured intraprocedurally, the next day and at every control visit (1, 6 and 12 months after implantation). Complications were noted at any time they were revealed. Pacing-induced cardiomyopathy (PICM) was defined as a drop in LVEF of at least 10 percentage points in the case of a high ventricular pacing burden after the exclusion of alternative causes (coronary artery disease, valvular heart disease, alcohol addiction, etc.). The electrocardiographic parameters required in LBBAP were measured at a high sweep speed with digital callipers (R-wave peak time in lead V6 (V6-RWPT), V6-V1 interpeak interval, paced and native QRS duration). The criteria for LBB capture were used according to recent EHRA consensus [
19].
2.5. Statistical Analysis
In the case of normally distributed variables, the results were reported as means and standard deviations; otherwise they were reported as medians and interquartile ranges. Student’s t-test for paired samples or the Wilcoxon signed-rank test if necessary were used to compare the NT-proBNP and echocardiographic parameters before implantation and after 12 months. To identify the factors associated with changes in the cardiac function parameters, Student’s t-test for independent samples, the Mann–Whitney U test and correlation coefficients (Pearson’s and Spearman’s) were applied. Univariable and multivariable logistic regression analyses were performed to find the predictors of heart function response. To compare the electrical parameters at subsequent visits, a Friedman test was conducted. Statistical analysis was performed using PSPP 1.6.2 software. A two-sided p-value < 0.05 was considered statistically significant.
4. Discussion
The major findings of this study are as follows: (1) LBBAP device implantation leads to a notable improvement in heart function parameters after a one-year follow-up, both in CRT and bradycardia patients, (2) a higher baseline NT-proBNP level and the presence of either RBBB or LBBB predict particularly positive heart function responses, (3) the electrical parameters of LBBAP leads are satisfactory and stable, (4) most severe complications of LBBAP device implantation are not related to the LBBAP lead, (5) the most frequent complications are iatrogenic RBBB, which usually subsides, and conversion to deep septal pacing (loss of LBBAP) and (6) some patients require switching off or modification of the auto-threshold algorithms to maintain an optimal type of capture.
The efficiency of LBBAP in CRT patients has already been proven in small to medium studies. An echocardiographic response has been shown in the general CRT population, in patients with RBBB and in those with PICM indications, as well as in those with LBBAP-optimized CRT [
12,
13,
14,
15,
16]. Our results are consistent with these findings, showing a significant improvement in NT-proBNP level, LVEF and LAD in the non-selected CRT population, despite the small group studied. We revealed a strong correlation between the distance from the base of the anterior mitral cusp to the tip of the LBBAP lead and a change in LVEF. This finding suggests that proximal left bundle branch capture in the basal part of the septum may enhance the effect of CRT.
Importantly, a lower but still significant improvement in the NT-proBNP level and some echocardiographic end-points was also noted in the bradycardia patients. Although LVEF did not increase in this group, the positive response in the NT-proBNP level, LVEDD and LAD may suggest that the left ventricular end-diastolic pressure decreased. The mechanism underlying this improvement in the bradycardia patients seems to be complex. Subjects with a high-grade atrioventricular block benefit from an increase in heart rate and restoration of atrioventricular synchrony without significant impairment in intraventricular synchrony [
6]. However, an improvement was also noted in patients with sick sinus syndrome. Several factors may contribute to this effect. The first is release from bradycardia (by atrial pacing or occasional ventricular pacing). Moreover, patients with bundle branch block or first-degree atrioventricular block may benefit from the resynchronizing effect of LBBAP (pacing was promoted in 29% of patients with sick sinus syndrome). Finally, better general treatment due to regular follow-up visits may also influence the results. However, quantification of the contributions of individual mechanisms is hard to assess without a direct comparison of LBBAP and RVP.
Bednarek et al. [
10] showed that LVEF increased in bradycardia patients with baseline LVEF below 50%, while it was stable in individuals with preserved LVEF, and they concluded that LBBAP prevents PICM in patients with preserved LVEF and improves left ventricle function in subjects with depressed LVEF. Our results are, in general, consistent with these findings. However, on the one hand, the outcomes of the present study suggest that patients with preserved LVEF also receive a benefit in heart function (improvement in NT-proBNP, LVEDD and LAD), but on the other hand it should be emphasized that we noted a case of presumed PICM. Since we found that shorter V6-RWPT, confirmed left bundle branch capture and greater narrowing of the QRS complex were related to better outcomes in some echocardiographic end-points, particular attention may be paid to achieving satisfactory results in these parameters, especially in patients with any evidence of a heart function impairment, because this population is particularly prone to PICM [
20] (the patient who developed PICM had a relatively high baseline NT-proBNP level).
Our results showed that the presence of either RBBB or LBBB predicts a positive heart function response in the unselected LBBAP population as well as in the bradycardia indication group (with an even greater odds ratio). The possible explanation of this phenomenon is the dualistic nature of LBBAP. LBB capture provides quick activation of the left ventricle, while concomitant myocardial septal capture ensures faster propagation to the right ventricle than in native conduction with RBBB. This effect may be further enhanced by ring capture [
14]. An improvement in ventricular synchrony in the case of nonspecific intraventricular conduction delay, usually associated with ventricular hypertrophy or scar, remains a challenge.
It has already been shown that the electrical parameters in LBBAP are satisfactory and stable in short-term follow-up [
5,
11]. We noticed that the pacing parameters significantly improved between implantation and the next day. Regarding the capture threshold, this constantly increased after the initial decrease. This suggests that the capture threshold still requires long-term observation. Special attention should be paid to identifying a possible dissimilarity in the capture thresholds of the myocardium and left bundle branch. Four patients from the studied group required individual programming of the pacing output to maintain non-selective LBB capture, since the LBB pacing threshold was notably greater than the myocardial one and the default auto-threshold settings led to a loss of it and, in consequence, to an increase in V6-RWPT and QRS duration, as well as to worse ventricular synchrony [
6]. Therefore, electrocardiographic evaluation of QRS morphology at different pacing outputs at control visits is needed to reveal potential transitions of capture types and provide the adequate programming of devices.
The cumulative number of complications observed in our study seems to be relatively high. However, most of the major complications were general and not directly related to the LBBAP lead. The case of possible PICM has been noted, but it would presumably also have occurred if RVP had been used instead of LBBAP. This thesis may be supported by our observation that three patients with baseline PICM improved after upgrading from RVP to LBBAP. Moreover, the prevalence of PICM during RVP is more than 10% [
20]. On the other hand, most of the minor complications are linked with LBBAP. We reported iatrogenic RBBB in 9.1% of patients intraprocedurally and in 3.3% after one year. The prevalence of this complication may be even higher—19.9% and 6.3%, respectively [
11]—while septal perforation occurs in up to 14.4% of patients, usually without further repercussions [
19]. The most frequent complication in the follow-up period was the conversion to deep septal pacing, which was noted in 5.5% of cases. Nevertheless, the electrocardiographic effect of this modality is still better than in RVP.






{kind=link}
{kind=link}