
Reassessing Trabeculectomy: A Long-Term Study with Stringent Success Criteria

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 390, 2183–2193. [Google Scholar] [CrossRef] [PubMed]
- Cvenkel, B.; Kolko, M. Current Medical Therapy and Future Trends in the Management of Glaucoma Treatment. J. Ophthalmol. 2020, 2020, 6138132. [Google Scholar] [CrossRef]
- Dietlein, T.S.; Hermann, M.M.; Jordan, J.F. The Medical and Surgical Treatment of Glaucoma. Dtsch. Arztebl. Int. 2009, 106, 597–605, quiz 606. [Google Scholar] [CrossRef] [PubMed]
- Landers, J.; Martin, K.; Sarkies, N.; Bourne, R.; Watson, P. A Twenty-Year Follow-up Study of Trabeculectomy: Risk Factors and Outcomes. Ophthalmology 2012, 119, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Lusthaus, J.A.; Kubay, O.; Karim, R.; Wechsler, D.; Booth, F. Primary Trabeculectomy with Mitomycin C: Safety and Efficacy at 2 Years: Trabeculectomy with Mitomycin C. Clin. Exp. Ophthalmol. 2010, 38, 831–838. [Google Scholar] [CrossRef]
- Luebke, J.; Neuburger, M.; Jordan, J.F.; Wecker, T.; Boehringer, D.; Cakir, B.; Reinhard, T.; Anton, A. Bleb-Related Infections and Long-Term Follow-up after Trabeculectomy. Int. Ophthalmol. 2019, 39, 571–577. [Google Scholar] [CrossRef]
- Beckers, H.J.M.; Kinders, K.C.; Webers, C.A.B. Five-Year Results of Trabeculectomy with Mitomycin C. Graefe’s Arch. Clin. Exp. Ophthalmol. 2003, 241, 106–110. [Google Scholar] [CrossRef]
- Ehrnrooth, P.; Lehto, I.; Puska, P.; Laatikainen, L. Long-Term Outcome of Trabeculectomy in Terms of Intraocular Pressure. Acta Ophthalmol. Scand. 2002, 80, 267–271. [Google Scholar] [CrossRef]
- Sihota, R.; Angmo, D.; Ramaswamy, D.; Dada, T. Simplifying “Target” Intraocular Pressure for Different Stages of Primary Open-Angle Glaucoma and Primary Angle-Closure Glaucoma. Indian J. Ophthalmol. 2018, 66, 495. [Google Scholar] [CrossRef]
- The Advanced Glaucoma Intervention Study (AGIS): 7. The Relationship between Control of Intraocular Pressure and Visual Field Deterioration. Am. J. Ophthalmol. 2000, 130, 429–440. [CrossRef]
- Diestelhorst, M.; Khalili, M.A.; Krieglstein, G.K. Trabeculectomy: A Retrospective Follow-up of 700 Eyes. Int. Ophthalmol. 1998, 22, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Reibaldi, A.; Uva, M.G.; Longo, A. Nine-Year Follow-up of Trabeculectomy with or without Low-Dosage Mitomycin-c in Primary Open-Angle Glaucoma. Br. J. Ophthalmol. 2008, 92, 1666–1670. [Google Scholar] [CrossRef] [PubMed]
- King, A.J.; Rotchford, A.P.; Alwitry, A.; Moodie, J. Frequency of Bleb Manipulations after Trabeculectomy Surgery. Br. J. Ophthalmol. 2007, 91, 873–877. [Google Scholar] [CrossRef]
- Cankaya, A.B.; Elgin, U. Comparison of the Outcome of Repeat Trabeculectomy with Adjunctive Mitomycin C and Initial Trabeculectomy. Korean J. Ophthalmol. 2011, 25, 401. [Google Scholar] [CrossRef] [PubMed]
- Eslami, Y.; Samarai, V.; Mohammadi, M.; Fakhraie, G.; Zarei, R.; Eslami, S.; Moghimi, S. Outcomes of Same-Site Re-Operation with Minimal Use of Mitomycin in Failed Trabeculectomy. Int. Ophthalmol. 2014, 34, 501–504. [Google Scholar] [CrossRef]
- Hirunpatravong, P.; Reza, A.; Romero, P.; Kim, E.A.; Nouri-Mahdavi, K.; Law, S.K.; Morales, E.; Caprioli, J. Same-Site Trabeculectomy Revision for Failed Trabeculectomy: Outcomes and Risk Factors for Failure. Am. J. Ophthalmol. 2016, 170, 110–118. [Google Scholar] [CrossRef]
- Bar-David, L.; Blumenthal, E.Z. Evolution of Glaucoma Surgery in the Last 25 Years. Rambam Maimonides Med. J. 2018, 9, e0024. [Google Scholar] [CrossRef]
- Wagner, F.M.; Schuster, A.K.-G.; Emmerich, J.; Chronopoulos, P.; Hoffmann, E.M. Efficacy and Safety of XEN®—Implantation vs. Trabeculectomy: Data of a “Real-World” Setting. PLoS ONE 2020, 15, e0231614. [Google Scholar] [CrossRef]
- Van Lancker, L.; Saravanan, A.; Abu-Bakra, M.; Reid, K.; Quijano, C.; Goyal, S.; Rodrigues, I.; Lascaratos, G.; Trikha, S.; Barwood, C.; et al. Clinical Outcomes and Cost Analysis of PreserFlo versus Trabeculectomy for Glaucoma Management in the United Kingdom. Ophthalmol. Glaucoma 2022, 6, 342–357. [Google Scholar] [CrossRef] [PubMed]
- Panarelli, J.F.; Banitt, M.R.; Gedde, S.J.; Shi, W.; Schiffman, J.C.; Feuer, W.J. A Retrospective Comparison of Primary Baerveldt Implantation versus Trabeculectomy with Mitomycin C. Ophthalmology 2016, 123, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Oberfeld, B.; El Helwe, H.; Hall, N.; Falah, H.; Chang, T.C.; Solá-Del Valle, D. Comparative Outcomes of Phacoemulsification Combined with Micro-Invasive Glaucoma Surgery plus: Schlemm Canal Microstent versus Ab Interno Trabecular Excision. J. Français D’ophtalmologie 2023, 46, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Kozera, M.; Konopińska, J.; Mariak, Z.; Rękas, M. Treatment of Open-Angle Glaucoma with iStent Implantation Combined with Phacoemulsification in Polish Caucasian Population. Clin. Ophthalmol. 2021, 15, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Dang, Y.-L.; Cen, Y.-J.; Hong, Y.; Huang, P.; Wang, N.-L.; Wang, C.; Zhang, C. Safety and Efficiency of Trabectome-Mediated Trabecular Meshwork Ablation for Chinese Glaucoma Patients: A Two-Year, Retrospective, Multicentre Study. Chin. Med. J. 2018, 131, 420–425. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
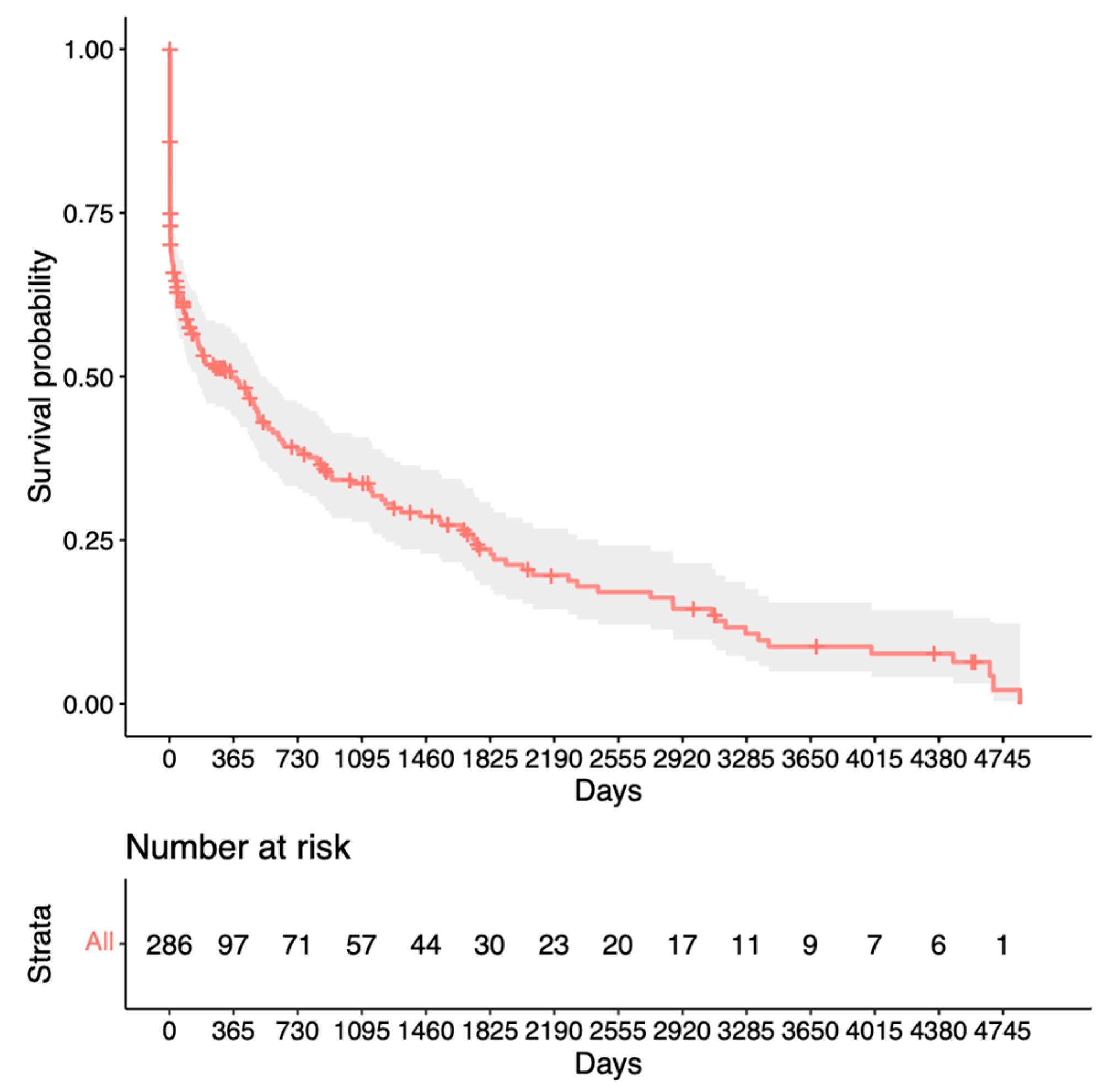
| Overview of Success Criteria | |
|---|---|
| Criterion 1 1 | IOP of ≤15 mmHg and no pressure-lowering medication |
| Criterion 2 1 | No revision surgery undertaken |
| Criterion 3 1 | No IOP-lowering surgery excluding revision surgery undertaken |
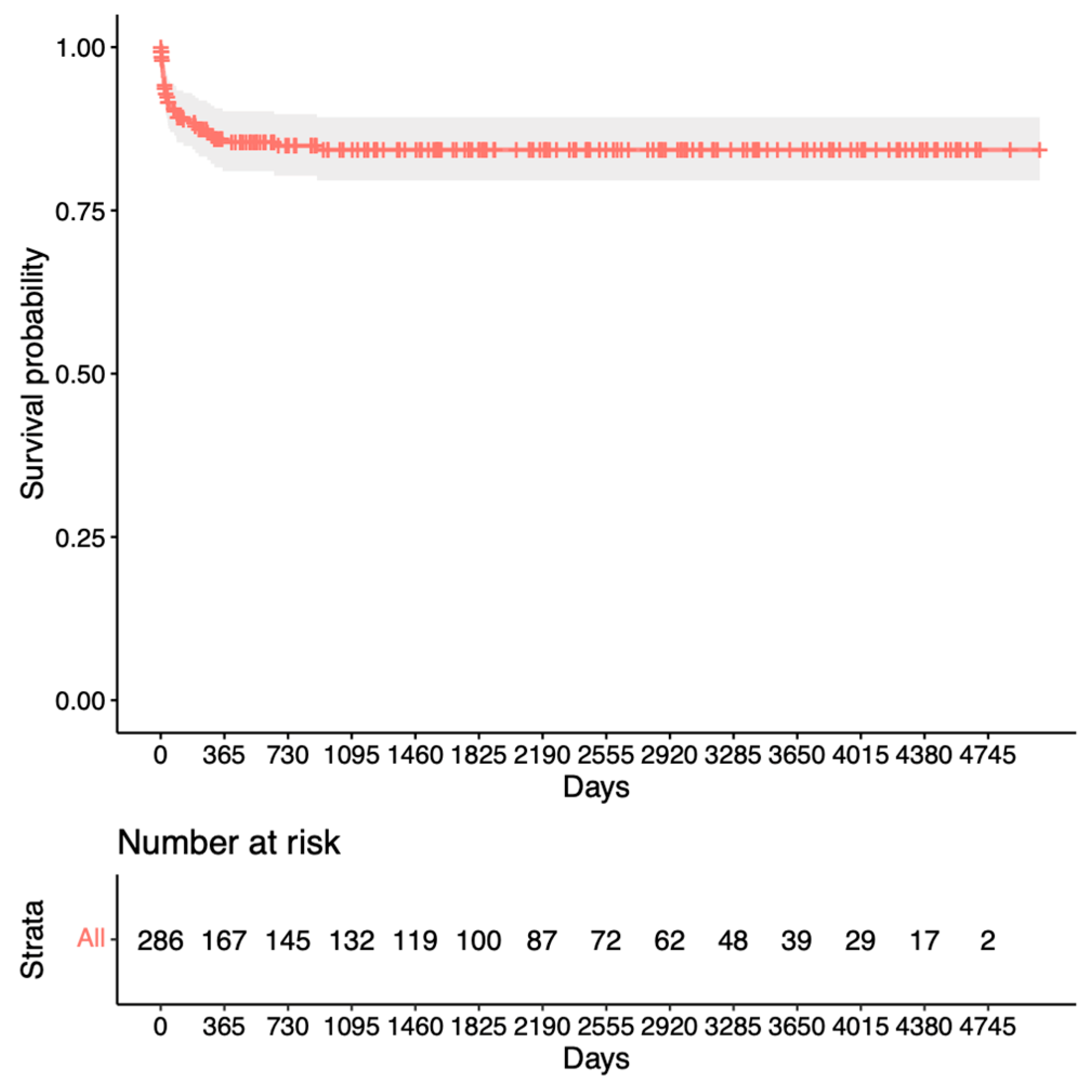
| Criterion 4 2 | No IOP-lowering surgery after revision surgery undertaken |
| Variable | |
|---|---|
| Eyes included (n) | 286 |
| Age, mean | 69.8 (±8.6) |
| Sex (female) | 57% |
| Type of glaucoma | |
| POAG 1 | 217 (75.9%) |
| PEX 2 | 58 (20.3%) |
| NTG 3 | 11 (3.8%) |
| Preoperative IOP 4 in mmHg, mean | 26.1 (±7.6) |
| Followup time in days, mean | 1841 (±1567.2) |
| Followup time after revisional surgery, mean | 1432 (±917.1) |
| Diabetes | 26 (9%) |
| Anticoagulation | 54 (19%) |
| Complication | n |
|---|---|
| Bleb leakage | 30 (10.5%) |
| Macular edema | 2 (0.7%) |
| Aqueous misdirection | 2 (0.7%) |
| Hyphema | 13 (4.5%) |
| Authors | Eyes | MFU (Years) | Pre-OP IOP (mmHg) | Success Criteria | Success Rates | ||
|---|---|---|---|---|---|---|---|
| 1 Year | 5 Years | MFU | |||||
| Beckers et al. [7] | 60 | 5.5 | 22.3 | ≤15/no meds | 83.4% | 60% | 60% |
| Lusthaus et al. [5] | 60 | 3 | 25.3 | ≤18 + no meds | 50% | N/A | 33% |
| Ehrnrooth et al. [8] | 138 | 3.5 | 24.6 | ≤21 + no therapy | 63% | N/A | 45% |
| Diestelhorst et al. [11] | 700 | 1.4 | 28.5 | <21 + * | 61% | 37.8% | 60% |
| Present study | 286 | 5 | 26.1 | ≤15 + no meds | 55% | 25% | 25% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braun, P.; Böhringer, D.; Jordan, J.; Reich, M.; Keye, P.; Reinhard, T.; Lübke, J. Reassessing Trabeculectomy: A Long-Term Study with Stringent Success Criteria. J. Clin. Med. 2024, 13, 1629. https://doi.org/10.3390/jcm13061629
Braun P, Böhringer D, Jordan J, Reich M, Keye P, Reinhard T, Lübke J. Reassessing Trabeculectomy: A Long-Term Study with Stringent Success Criteria. Journal of Clinical Medicine. 2024; 13(6):1629. https://doi.org/10.3390/jcm13061629
Chicago/Turabian StyleBraun, Philip, Daniel Böhringer, Jens Jordan, Michael Reich, Philip Keye, Thomas Reinhard, and Jan Lübke. 2024. "Reassessing Trabeculectomy: A Long-Term Study with Stringent Success Criteria" Journal of Clinical Medicine 13, no. 6: 1629. https://doi.org/10.3390/jcm13061629
APA StyleBraun, P., Böhringer, D., Jordan, J., Reich, M., Keye, P., Reinhard, T., & Lübke, J. (2024). Reassessing Trabeculectomy: A Long-Term Study with Stringent Success Criteria. Journal of Clinical Medicine, 13(6), 1629. https://doi.org/10.3390/jcm13061629