
Which Factors Are Associated with Persistence of Depressive and Anxiety Symptoms in Patients Affected by Atopic Dermatitis despite 2-Year Treatment with Dupilumab?

 ,
,  , , , ,
, , , ,  and
and 
Abstract
1. Introduction
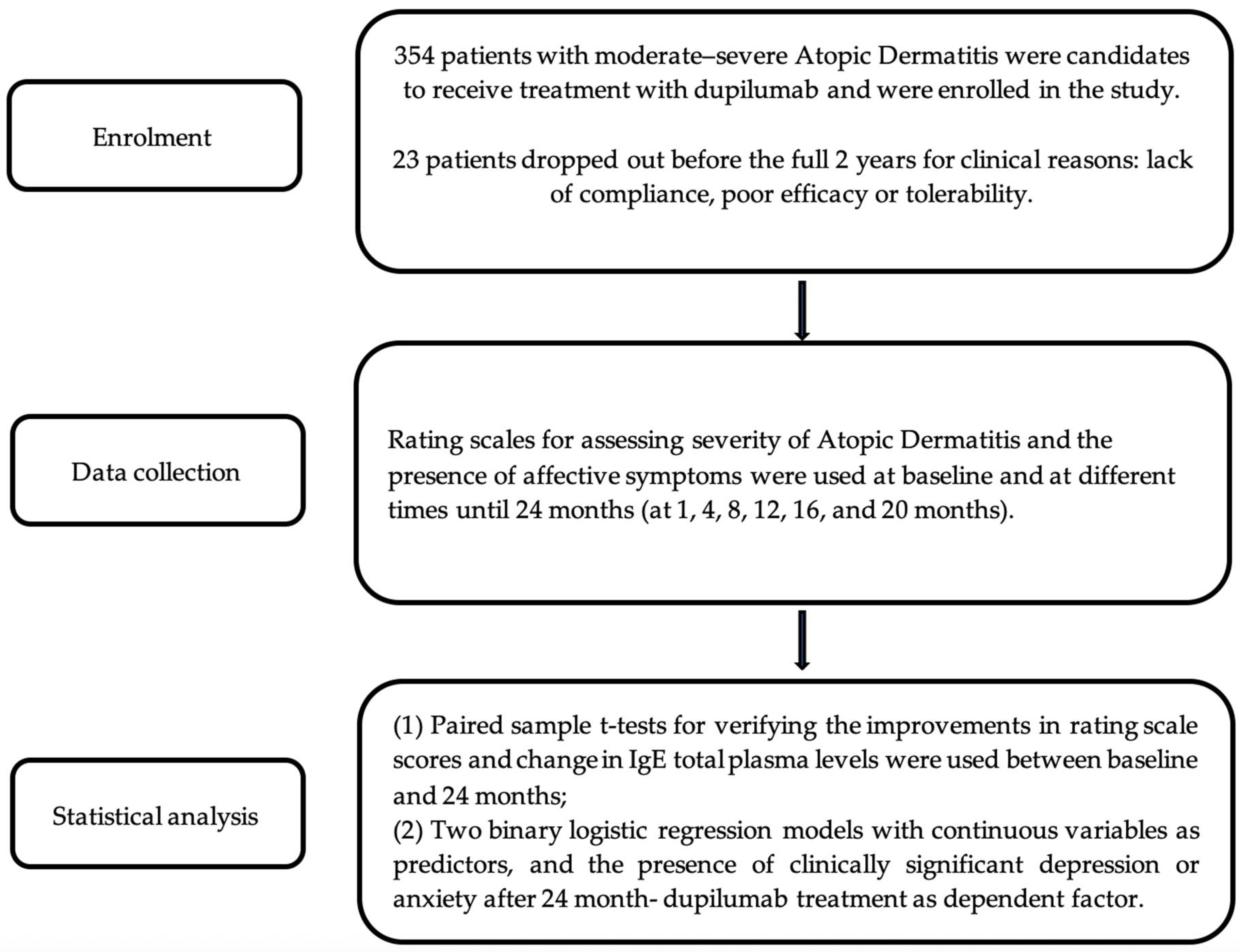
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ständer, S. Atopic Dermatitis. N. Engl. J. Med. 2021, 384, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.; Jaworski, J.C.; Simpson, E.L.; Boguniewicz, M.; Russell, J.J.; Block, J.K.; Tofte, S.; Dunn, J.D.; Feldman, S.R.; Clark, A.R.; et al. Major Comorbidities of Atopic Dermatitis: Beyond Allergic Disorders. Am. J. Clin. Dermatol. 2018, 19, 821–838. [Google Scholar] [CrossRef] [PubMed]
- Radtke, S.; Grossberg, A.L.; Wan, J. Mental health comorbidity in youth with atopic dermatitis: A narrative review of possible mechanisms. Pediatr. Dermatol. 2023, 40, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Kauppi, S.; Jokelainen, J.; Timonen, M.; Tasanen, K.; Huilaja, L. Atopic dermatitis and the risk of eating disorders: A population-based cohort study. J. Am. Acad. Dermatol. 2022, 87, 474–476. [Google Scholar] [CrossRef] [PubMed]
- Fan, R.; Chen, G.; Leasure, A.C.; Johnson, M.C.; Damsky, W.; Cohen, J.M. Association of atopic dermatitis with schizophrenia and schizoaffective disorder. Arch. Dermatol. Res. 2023, 315, 2731–2733. [Google Scholar] [CrossRef] [PubMed]
- Pilz, A.C.; Durner, V.; Schielein, M.C.; Schuster, B.; Beckmann, J.; Biedermann, T.; Eyerich, K.; Zink, A. Addictions in patients with atopic dermatitis: A cross-sectional pilot study in Germany. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 84–90. [Google Scholar] [CrossRef]
- Ferrucci, S.M.; Tavecchio, S.; Nicolini, G.; Angileri, L.; Ceresa, A.; Del Tordello, G.; Berti, E.; Marzano, A.V.; Buoli, M. Mental health in patients affected by atopic dermatitis: Which effects of treatment with dupilumab? Int. Clin. Psychopharmacol. 2023, 39, 201–205. [Google Scholar] [CrossRef]
- Cheng, C.M.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Su, T.P.; Li, C.T.; Yang, A.C.; Chang, W.H.; Chen, T.J.; Tsai, S.J.; et al. Risk of developing major depressive disorder and anxiety disorders among adolescents and adults with atopic dermatitis: A nationwide longitudinal study. J. Affect. Disord. 2015, 178, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Vinh, N.M.; Trang, V.T.T.; Dac Thuy, L.N.; Tam, H.T.X.; Hang, L.T.T.; Bac, P.V. The anxiety and depression disorder in adults with atopic dermatitis: Experience of a dermatology hospital. Dermatol. Rep. 2022, 15, 9524. [Google Scholar] [CrossRef]
- Ferrucci, S.M.; Tavecchio, S.; Angileri, L.; Surace, T.; Berti, E.; Buoli, M. Factors Associated with Affective Symptoms and Quality of Life in Patients with Atopic Dermatitis. Acta Derm. Venereol. 2021, 101, adv00590. [Google Scholar] [CrossRef]
- Fabrazzo, M.; Cipolla, S.; Signoriello, S.; Camerlengo, A.; Calabrese, G.; Giordano, G.M.; Argenziano, G.; Galderisi, S. A systematic review on shared biological mechanisms of depression and anxiety in comorbidity with psoriasis, atopic dermatitis, and hidradenitis suppurativa. Eur. Psychiatry 2021, 64, e71. [Google Scholar] [CrossRef] [PubMed]
- Benzecry, V.; Pravettoni, V.; Segatto, G.; Marzano, A.V.; Ferrucci, S. Type 2 Inflammation: Atopic Dermatitis, Asthma, and Hypereosinophilia Successfully Treated with Dupilumab. J. Investig. Allergol. Clin. Immunol. 2021, 31, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Caldiroli, A.; Capuzzi, E.; Barkin, J.L.; Grassi, S.; Esposito, C.M.; Auxilia, A.M.; Russo, S.; Tagliabue, I.; Carnevali, G.S.; Mucci, F.; et al. Is there an association between inflammatory/anti-oxidant markers and the presence of psychotic symptoms or severity of illness in mood and psychotic disorders? A multi-centric study on a drug-free sample. Brain Behav. Immun. Health 2022, 22, 100453. [Google Scholar] [CrossRef] [PubMed]
- Amadio, P.; Macchi, C.; Favero, C.; Zarà, M.; Solazzo, G.; Dioni, L.; Sandrini, L.; Vigna, L.; Greco, M.F.; Buoli, M.; et al. Brain-Derived Neurotrophic Factor and Extracellular Vesicle-Derived miRNAs in an Italian Cohort of Individuals with Obesity: A Key to Explain the Link Between Depression and Atherothrombosis. Front. Cardiovasc. Med. 2022, 9, 906483. [Google Scholar] [CrossRef] [PubMed]
- D’Cunha, N.M.; Sergi, D.; Lane, M.M.; Naumovski, N.; Gamage, E.; Rajendran, A.; Kouvari, M.; Gauci, S.; Dissanayka, T.; Marx, W.; et al. The Effects of Dietary Advanced Glycation End-Products on Neurocognitive and Mental Disorders. Nutrients 2022, 14, 2421. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.Y.; Kim, M.J.; Hong, J.K.; Noh, H.H.; Park, K.Y.; Lee, M.K.; Seo, S.J. In vivo quantitative analysis of advanced glycation end products in atopic dermatitis-Possible culprit for the comorbidities? Exp. Dermatol. 2020, 29, 1012–1016. [Google Scholar] [CrossRef]
- Stingeni, L.; Belloni Fortina, A.; Baiardini, I.; Hansel, K.; Moretti, D.; Cipriani, F. Atopic Dermatitis and Patient Perspectives: Insights of Bullying at School and Career Discrimination at Work. J. Asthma Allergy 2021, 14, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Chatrath, S.; Lei, D.; Yousaf, M.; Chavda, R.; Gabriel, S.; Silverberg, J.I. Longitudinal course and predictors of depressive symptoms in atopic dermatitis. J. Am. Acad. Dermatol. 2022, 87, 582–591. [Google Scholar] [CrossRef] [PubMed]
- Dieris-Hirche, J.; Gieler, U.; Petrak, F.; Milch, W.; Te Wildt, B.; Dieris, B.; Herpertz, S. Suicidal Ideation in Adult Patients with Atopic Dermatitis: A German Cross-sectional Study. Acta Derm. Venereol. 2017, 97, 1189–1195. [Google Scholar] [CrossRef]
- Kamei, K.; Hirose, T.; Yoshii, N.; Tanaka, A. Burden of illness, medication adherence, and unmet medical needs in Japanese patients with atopic dermatitis: A retrospective analysis of a cross-sectional questionnaire survey. J. Dermatol. 2021, 48, 1491–1498. [Google Scholar] [CrossRef]
- Seegräber, M.; Srour, J.; Walter, A.; Knop, M.; Wollenberg, A. Dupilumab for treatment of atopic dermatitis. Expert Rev. Clin. Pharmacol. 2018, 11, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Thaçi, D.; Hamilton, J.D.; Graham, N.M.; Bieber, T.; Rocklin, R.; Ming, J.E.; Ren, H.; Kao, R.; Simpson, E.; et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N. Engl. J. Med. 2014, 371, 130–139. [Google Scholar] [CrossRef]
- Tavecchio, S.; Angileri, L.; Pozzo Giuffrida, F.; Germiniasi, F.; Marzano, A.V.; Ferrucci, S. Efficacy of Dupilumab on Different Phenotypes of Atopic Dermatitis: One-Year Experience of 221 Patients. J. Clin. Med. 2020, 9, 2684. [Google Scholar] [CrossRef]
- Benedetti, F.; Mazza, M.; Cavalli, G.; Ciceri, F.; Dagna, L.; Rovere-Querini, P. Can Cytokine Blocking Prevent Depression in COVID-19 Survivors? J. Neuroimmune Pharmacol. 2021, 16, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, O. Investigational Drugs for the Treatment of Depression (Part 1): Monoaminergic, Orexinergic, GABA-Ergic, and Anti-Inflammatory Agents. Front. Pharmacol. 2022, 13, 884143. [Google Scholar] [CrossRef] [PubMed]
- Merola, J.F.; Chiou, A.S.; During, E.; Costanzo, A.; Foley, P.; Alfalasi, A.; Gogate, S.; Pinter, A.; Dodiuk-Gad, R.; Simon, D.; et al. Dupilumab significantly improves sleep in adults with atopic dermatitis: Results from the 12-week placebo-controlled period of the 24-week phase 4 randomized double-blinded placebo-controlled DUPISTAD study. Br. J. Dermatol. 2023, 189, 685–694. [Google Scholar] [CrossRef]
- Piraccini, B.M.; Ohyama, M.; Craiglow, B.; Bewley, A.; Ding, Y.; Chen, Y.F.; Dutronc, Y.; Pierce, E.; Durand, F.; Mostaghimi, A. Scalp hair regrowth is associated with improvements in health-related quality of life and psychological symptoms in patients with severe alopecia areata: Results from two randomized controlled trials. J. Dermatolog. Treat. 2023, 34, 2227299. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.; Chandran, A.; Zografos, L.; Zlateva, G. Evaluation of the impact of fibromyalgia on patients’ sleep and the content validity of two sleep scales. Health Qual. Life Outcomes 2009, 7, 64. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.; Vyas, J.; Finlay, A.Y. Counting the Burden: Atopic Dermatitis and Health-related Quality of Life. Acta Derm. Venereol. 2020, 100, adv00161. [Google Scholar] [CrossRef]
- Pariser, D.M.; Simpson, E.L.; Gadkari, A.; Bieber, T.; Margolis, D.J.; Brown, M.; Nelson, L.; Mahajan, P.; Reaney, M.; Guillemin, I.; et al. Evaluating patient-perceived control of atopic dermatitis: Design, validation, and scoring of the Atopic Dermatitis Control Tool (ADCT). Curr. Med. Res. Opin. 2020, 36, 367–376. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Thyssen, J.P.; Fahrbach, K.; Mickle, K.; Cappelleri, J.C.; Romero, W.; Cameron, M.C.; Myers, D.E.; Clibborn, C.; Di Bonaventura, M. Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: A systematic literature review and network meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Cork, M.J.; Eckert, L.; Simpson, E.L.; Armstrong, A.; Barbarot, S.; Puig, L.; Girolomoni, G.; de Bruin-Weller, M.; Wollenberg, A.; Kataoka, Y.; et al. Dupilumab improves patient-reported symptoms of atopic dermatitis, symptoms of anxiety and depression, and Health-related quality of life in moderate-to-severe atopic dermatitis: Analysis of pooled data from the randomized trials SOLO 1 and SOLO 2. J. Dermatolog. Treat. 2020, 31, 606–614. [Google Scholar] [CrossRef]
- Koya, T.; Sakai, N.; Sasaki, T.; Shinbori, K.; Nagai, A.; Kimura, Y.; Toyama, M.; Hayashi, M.; Saito, A.; Nishiyama, Y.; et al. Effect of Dupilumab on Depression in Asthma with Eosinophilic Chronic Rhinosinusitis in the Japanese Population. Int. Arch. Allergy Immunol. 2022, 183, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Ghani, H.; Jamgochian, M.; Pappert, A.; Rahman, R.; Cubeli, S. The Psychosocial Burden Associated with and Effective Treatment Approach for Atopic Dermatitis: A Literature Review. J. Drugs Dermatol. 2021, 20, 1046–1050. [Google Scholar] [PubMed]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef] [PubMed]
- Buoli, M.; Serati, M.; Grassi, S.; Pergoli, L.; Cantone, L.; Altamura, A.C.; Bollati, V. The role of clock genes in the etiology of Major Depressive Disorder. J. Affect. Disord. 2018, 234, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Rani, T.; Behl, T.; Sharma, N.; Makeen, H.A.; Albratty, M.; Alhazmi, H.A.; Meraya, A.M.; Bhatia, S.; Bungau, S.G. Exploring the role of biologics in depression. Cell. Signal. 2022, 98, 110409. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Dhar, A.K.; Samanta, M.K.; Suttee, A. Effects of Current Psychotropic Drugs on Inflammation and Immune System. Adv. Exp. Med. Biol. 2023, 1411, 407–434. [Google Scholar] [CrossRef]
- Plank, P.M.; Hinze, C.A.; Campbell, V.; Konwert, S.; Welte, T.; Drick, N.; Kayser, M.Z.; Suhling, H.; Fuge, J. Relationship Between the Response to Antibody Therapy and Symptoms of Depression and Anxiety Disorders in Patients with Severe Asthma. J. Asthma Allergy 2023, 16, 421–431. [Google Scholar] [CrossRef]
- Mesjasz, A.; Zawadzka, M.; Chałubiński, M.; Trzeciak, M. Is Atopic Dermatitis Only a Skin Disease? Int. J. Mol. Sci. 2023, 24, 837. [Google Scholar] [CrossRef]
- Glaus, J.; Cui, L.; Hommer, R.; Merikangas, K.R. Association between mood disorders and BMI/overweight using a family study approach. J. Affect. Disord. 2019, 248, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Iodice, S.; Ceresa, A.; Esposito, C.M.; Mucci, F.; Conti, D.M.; Pergoli, L.; Tarantini, L.; Vigna, L.; Bollati, V.; Buoli, M.; et al. The Independent Role of Body Mass Index (BMI) and Severity of Depressive Symptoms on Biological Changes of Women Affected by Overweight/Obesity. Int. J. Environ. Res. Public Health 2021, 18, 2923. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Guo, Z.; Yang, Y.; Liao, Y.; Shi, Y.; Zhang, L.J. Emerging Roles of Adipose Tissue in the Pathogenesis of Psoriasis and Atopic Dermatitis in Obesity. JID Innov. 2021, 2, 100064. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, J.; Moitinho-Silva, L.; Sander, N.; Harder, I.; Häsler, R.; Rodriguez, E.; Haufe, E.; Kleinheinz, A.; Abraham, S.; Heratizadeh, A.; et al. Dupilumab but not cyclosporine treatment shifts the microbiome toward a healthy skin flora in patients with moderate-to-severe atopic dermatitis. Allergy 2023, 78, 2290–2300. [Google Scholar] [CrossRef]
- Baurecht, H.; Welker, C.; Baumeister, S.E.; Weidnger, S.; Meisinger, C.; Leitzmann, M.F.; Emmert, H. Relationship between atopic dermatitis, depression and anxiety: A two-sample Mendelian randomization study. Br. J. Dermatol. 2021, 185, 781–786. [Google Scholar] [CrossRef]
- Buoli, M.; Capuzzi, E.; Caldiroli, A.; Ceresa, A.; Esposito, C.M.; Posio, C.; Auxilia, A.M.; Capellazzi, M.; Tagliabue, I.; Surace, T.; et al. Clinical and Biological Factors Are Associated with Treatment-Resistant Depression. Behav. Sci. 2022, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: Modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Fracas, E.; Costantino, A.; Vecchi, M.; Buoli, M. Depressive and Anxiety Disorders in Patients with Inflammatory Bowel Diseases: Are There Any Gender Differences? Int. J. Environ. Res. Public Health 2023, 20, 6255. [Google Scholar] [CrossRef]
- Verma, R.; Balhara, Y.P.; Gupta, C.S. Gender differences in stress response: Role of developmental and biological determinants. Ind. Psychiatry J. 2011, 20, 4–10. [Google Scholar] [CrossRef]
- Heck, A.L.; Handa, R.J. Sex differences in the hypothalamic-pituitary-adrenal axis’ response to stress: An important role for gonadal hormones. Neuropsychopharmacology 2019, 44, 45–58. [Google Scholar] [CrossRef]
- Shah, B.; Levenson, J.L. Use of psychotropic drugs in the dermatology patient: When to start and stop? Clin. Dermatol. 2018, 36, 748–755. [Google Scholar] [CrossRef] [PubMed]
- Senra, M.S.; Wollenberg, A. Psychodermatological aspects of atopic dermatitis. Br. J. Dermatol. 2014, 170, 38–43. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Buoli, M.; Posio, C.; Di Taranto, R.; Lo Muscio, A.; Cumbo, E.; Ostuzzi, S.; Caporali, R. COVID-19 related poor mental health and sleep disorders in rheumatic patients: A citizen science project. BMC Psychiatry 2021, 21, 385. [Google Scholar] [CrossRef] [PubMed]
- Sieniawska, J.; Lesiak, A.; Ciążyński, K.; Narbutt, J.; Ciążyńska, M. Impact of the COVID-19 Pandemic on Atopic Dermatitis Patients. Int. J. Environ. Res. Public Health 2022, 19, 1734. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M.; Galbussera, A.A.; D’Avanzo, B.; Tettamanti, M.; Remuzzi, G.; Fortino, I.; Leoni, O.; Harari, S.; Nobili, A. Two years of SARS-CoV-2 pandemic and COVID-19 in Lombardy, Italy. Intern. Emerg. Med. 2023, 18, 1445–1451. [Google Scholar] [CrossRef]
- Müller, N. Immunology of major depression. Neuroimmunomodulation 2014, 21, 123–130. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Total Sample (N = 331) |
|---|---|
| Age | 37.03 (±16.96) |
| Age at onset | 11.12 (±18.97) |
| Gender | |
| Male | 183 (55.3%) |
| Female | 148 (44.7%) |
| BMI | 24.46 (±10.50) |
| Duration of illness | 26.03 (±15.70) |
| Type of AD | |
| Extrinsic | 300 (90.6%) |
| Intrinsic | 31 (9.4%) |
| Baseline Systemic Treatment | |
| Cyclosporine | 58 (17.5%) |
| Corticosteroids | 26 (7.9%) |
| Methotrexate | 5 (1.5%) |
| Antihistamines | 7 (2.1%) |
| No systemic treatment | 235 (71.0%) |
| Previous treatment with cyclosporine | |
| Yes | 278 (84.0%) |
| No | 53 (16.0%) |
| Previous treatment with corticosteroids | |
| Yes | 258 (77.9%) |
| No | 73 (27.1%) |
| Previous treatment with methotrexate | |
| Yes | 30 (9.1%) |
| No | 301 (90.9%) |
| Previous treatment with azathioprine | |
| Yes | 7 (2.1%) |
| No | 324 (97.9%) |
| Previous treatment with alitretinoin | |
| Yes | 9 (2.7%) |
| No | 322 (97.3%) |
| Variables | Baseline (N = 331) Mean (±SD) | 24 Months (N = 331) Mean (±SD) | t | p |
|---|---|---|---|---|
| Total IgE (kU/L) | 3619.48 (±6348.51) | 655.95 (±1147.56) | 6.23 | <0.001 |
| HADS-anxiety | 8.46 (±4.23) | 3.41 (±3.57) | 18.14 | <0.001 |
| HADS-depression | 7.22 (±4.23) | 3.30 (±3.80) | 14.35 | <0.001 |
| POEM | 21.27 (±5.73) | 5.56 (±5.14) | 40.83 | <0.001 |
| DLQI | 15.70 (±6.63) | 2.61 (±2.98) | 34.27 | <0.001 |
| SQ-NRS | 6.81 (±3.07) | 0.65 (±1.65) | 33.64 | <0.001 |
| itch-NRS | 8.49 (±1.42) | 2.47 (±2.35) | 40.06 | <0.001 |
| PGA | 3.51 (±0.55) | 0.77 (±0.74) | 52.16 | <0.001 |
| EASI | 29.07 (±7.21) | 1.88 (±2.56) | 65.27 | <0.001 |
| ADCT | 19.98 (±3.81) | 3.86 (±3.68) | 54.82 | <0.001 |
| Baseline Variables | B | SE | Wald | p-Value | Exp(B) | 95% CI for Exp(B) |
|---|---|---|---|---|---|---|
| Age | −0.002 | 0.017 | 0.019 | 0.889 | 0.998 | 0.966–1.031 |
| Age at onset | −0.005 | 0.016 | 0.107 | 0.744 | 0.995 | 0.963–1.027 |
| BMI | 0.146 | 0.058 | 6.373 | 0.012 | 1.157 | 1.033–1.296 |
| IgE | 0.001 | 0.001 | 0.112 | 0.738 | 1.000 | 1.000–1.000 |
| Gender | 0.775 | 0.459 | 2.853 | 0.091 | 2.171 | 0.883–5.337 |
| EASI | −0.042 | 0.038 | 1.261 | 0.261 | 0.959 | 0.891–1.032 |
| PGA | −0.134 | 0.407 | 0.108 | 0.743 | 0.875 | 0.394–1.944 |
| Itch-NRS | −0.214 | 0.167 | 1.653 | 0.199 | 0.807 | 0.582–1.119 |
| SQ-NRS | 0.150 | 0.098 | 2.344 | 0.126 | 1.162 | 0.959–1.407 |
| DLQI | −0.108 | 0.044 | 5.933 | 0.015 | 0.898 | 0.823–0.979 |
| POEM | 0.038 | 0.049 | 0.619 | 0.431 | 1.039 | 0.944–1.143 |
| ADCT | 0.036 | 0.075 | 0.232 | 0.630 | 1.037 | 0.895–1.201 |
| HADS-Depression | 0.226 | 0.073 | 9.571 | 0.002 | 1.253 | 1.086–1.446 |
| HADS-Anxiety | 0.019 | 0.074 | 0.064 | 0.800 | 1.019 | 0.882–1.177 |
| Extrinsic/intrinsic subtype | −0.347 | 0.734 | 0.223 | 0.637 | 0.707 | 0.168–2.981 |
| Baseline Variables | B | SE | Wald | p-Value | Exp(B) | 95% CI for Exp(B) |
|---|---|---|---|---|---|---|
| Age | 0.007 | 0.017 | 0.190 | 0.663 | 1.007 | 0.975–1.041 |
| Age at onset | 0.002 | 0.017 | 0.014 | 0.906 | 1.002 | 0.970–1.035 |
| BMI | 0.097 | 0.056 | 2.942 | 0.086 | 1.102 | 0.986–1.230 |
| IgE | 0.001 | 0.001 | 0.473 | 0.492 | 1.000 | 1.000–1.000 |
| Gender | 1.070 | 0.505 | 4.487 | 0.034 | 2.916 | 1.083–7.848 |
| EASI | −0.049 | 0.039 | 1.565 | 0.211 | 0.953 | 0.883–1.028 |
| PGA | 0.276 | 0.446 | 0.383 | 0.536 | 1.318 | 0.550–3.160 |
| Itch-NRS | −0.081 | 0.167 | 0.233 | 0.629 | 0.923 | 0.665–1.279 |
| SQ-NRS | 0.141 | 0.099 | 2.013 | 0.156 | 1.152 | 0.948–1.399 |
| DLQI | −0.010 | 0.043 | 0.054 | 0.816 | 0.990 | 0.910–1.077 |
| POEM | 0.002 | 0.046 | 0.002 | 0.969 | 1.002 | 0.915–1.097 |
| ADCT | −0.075 | 0.076 | 0.960 | 0.327 | 0.928 | 0.799–1.077 |
| HADS-Depression | 0.120 | 0.074 | 2.660 | 0.103 | 1.128 | 0.976–1.304 |
| HADS-Anxiety | −0.076 | 0.078 | 0.951 | 0.329 | 0.927 | 0.795–1.080 |
| Extrinsic/intrinsic subtype | −0.128 | 0.713 | 0.032 | 0.858 | 0.880 | 0.217–3.562 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrucci, S.M.; Tavecchio, S.; Ceresa, A.; Angileri, L.; Berti, E.; Marzano, A.V.; Buoli, M. Which Factors Are Associated with Persistence of Depressive and Anxiety Symptoms in Patients Affected by Atopic Dermatitis despite 2-Year Treatment with Dupilumab? J. Clin. Med. 2024, 13, 1980. https://doi.org/10.3390/jcm13071980
Ferrucci SM, Tavecchio S, Ceresa A, Angileri L, Berti E, Marzano AV, Buoli M. Which Factors Are Associated with Persistence of Depressive and Anxiety Symptoms in Patients Affected by Atopic Dermatitis despite 2-Year Treatment with Dupilumab? Journal of Clinical Medicine. 2024; 13(7):1980. https://doi.org/10.3390/jcm13071980
Chicago/Turabian StyleFerrucci, Silvia Mariel, Simona Tavecchio, Alessandro Ceresa, Luisa Angileri, Emilio Berti, Angelo Valerio Marzano, and Massimiliano Buoli. 2024. "Which Factors Are Associated with Persistence of Depressive and Anxiety Symptoms in Patients Affected by Atopic Dermatitis despite 2-Year Treatment with Dupilumab?" Journal of Clinical Medicine 13, no. 7: 1980. https://doi.org/10.3390/jcm13071980
APA StyleFerrucci, S. M., Tavecchio, S., Ceresa, A., Angileri, L., Berti, E., Marzano, A. V., & Buoli, M. (2024). Which Factors Are Associated with Persistence of Depressive and Anxiety Symptoms in Patients Affected by Atopic Dermatitis despite 2-Year Treatment with Dupilumab? Journal of Clinical Medicine, 13(7), 1980. https://doi.org/10.3390/jcm13071980