
Prediction of Intracranial Pressure in Patients with an Aneurysmal Subarachnoid Hemorrhage Using Optic Nerve Sheath Diameter via Explainable Predictive Modeling


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Measurement of Optic Nerve Sheath Diameter
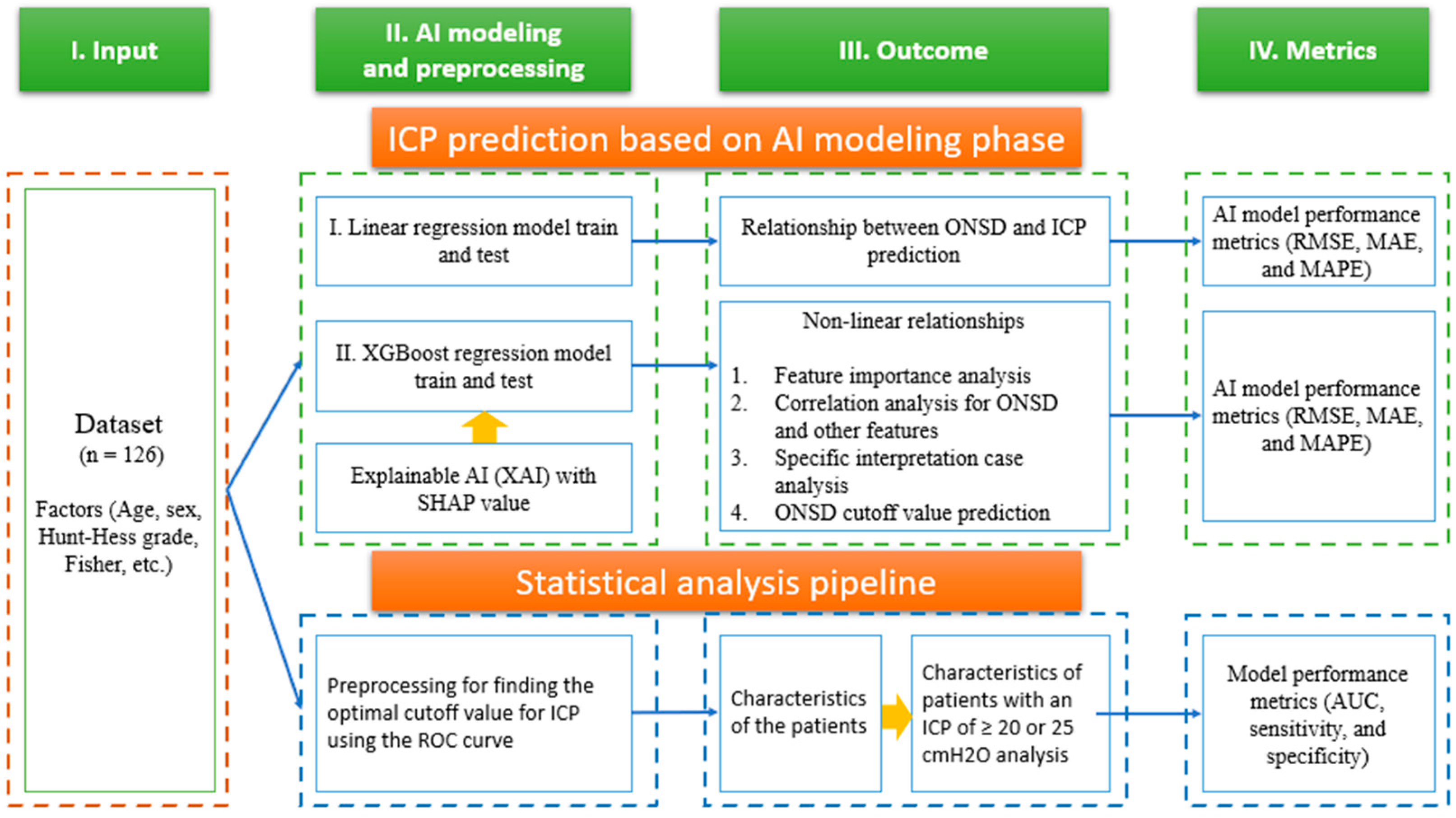
2.3. Research Diagram
2.4. Programming Environment and Analysis Software Used
3. Results
3.1. Clinical Characteristics of the Patients and the Criteria for ICP > 20 and 25 cmH2O
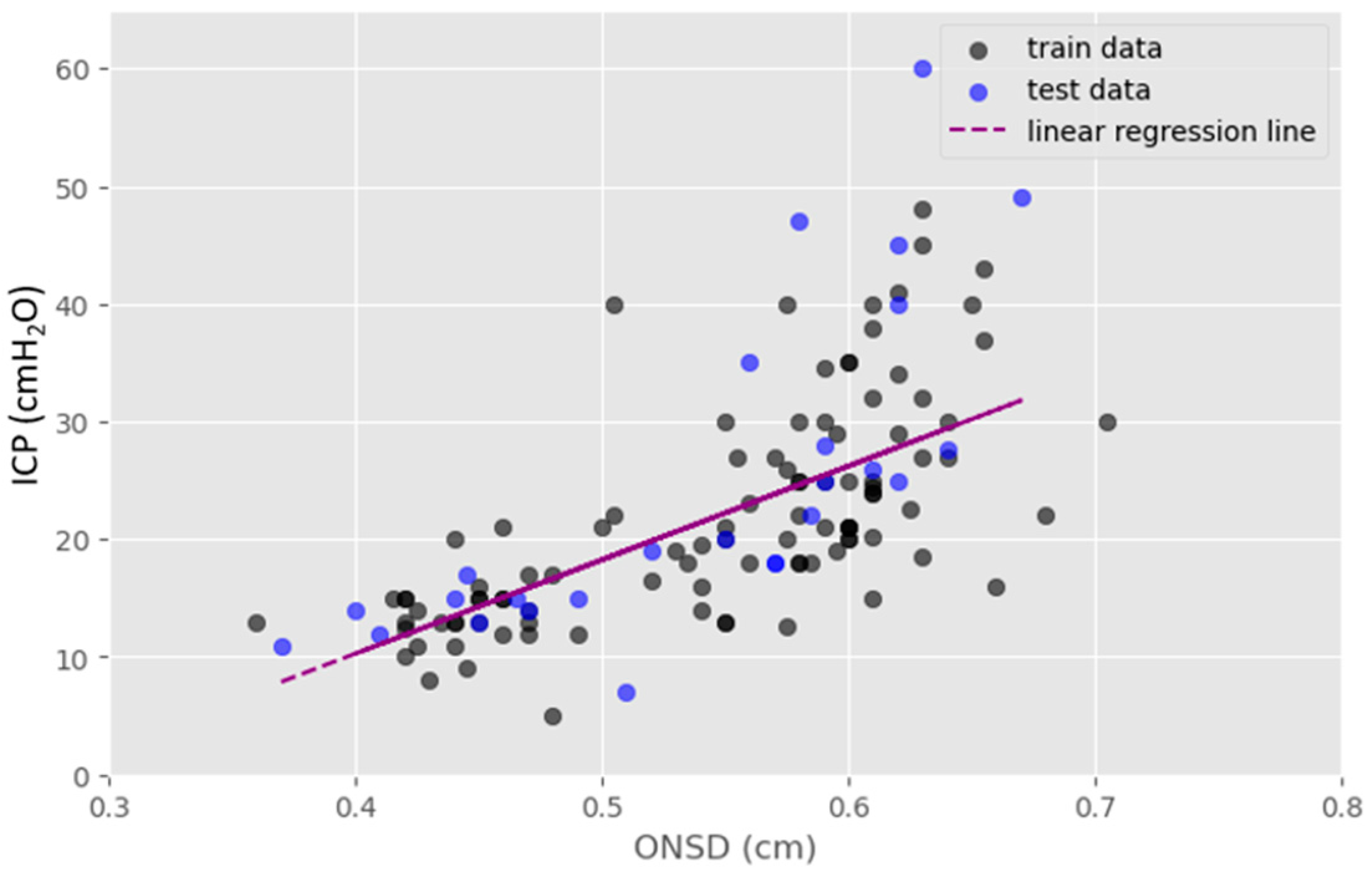
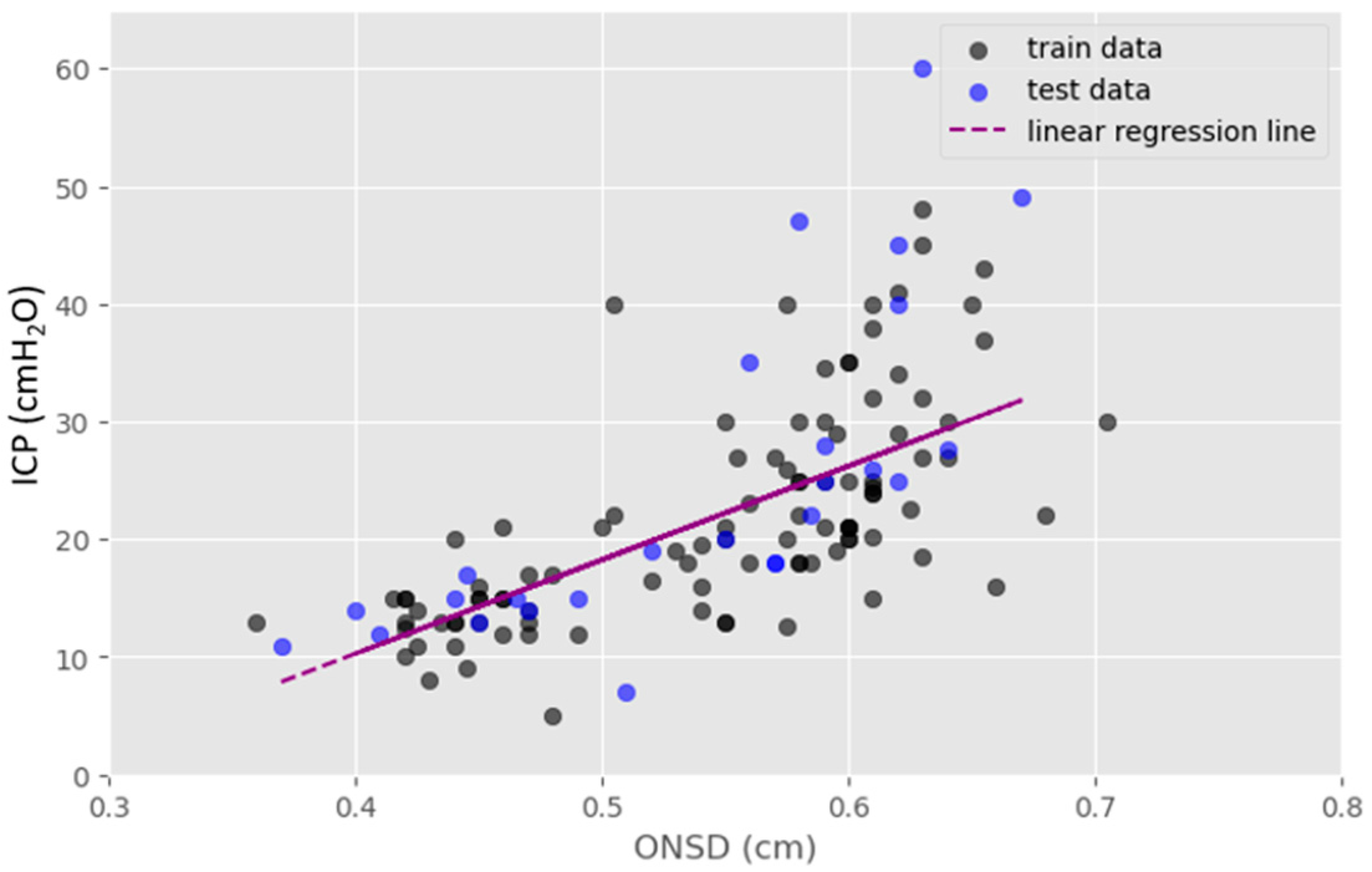
3.2. Association between ONSD and ICP
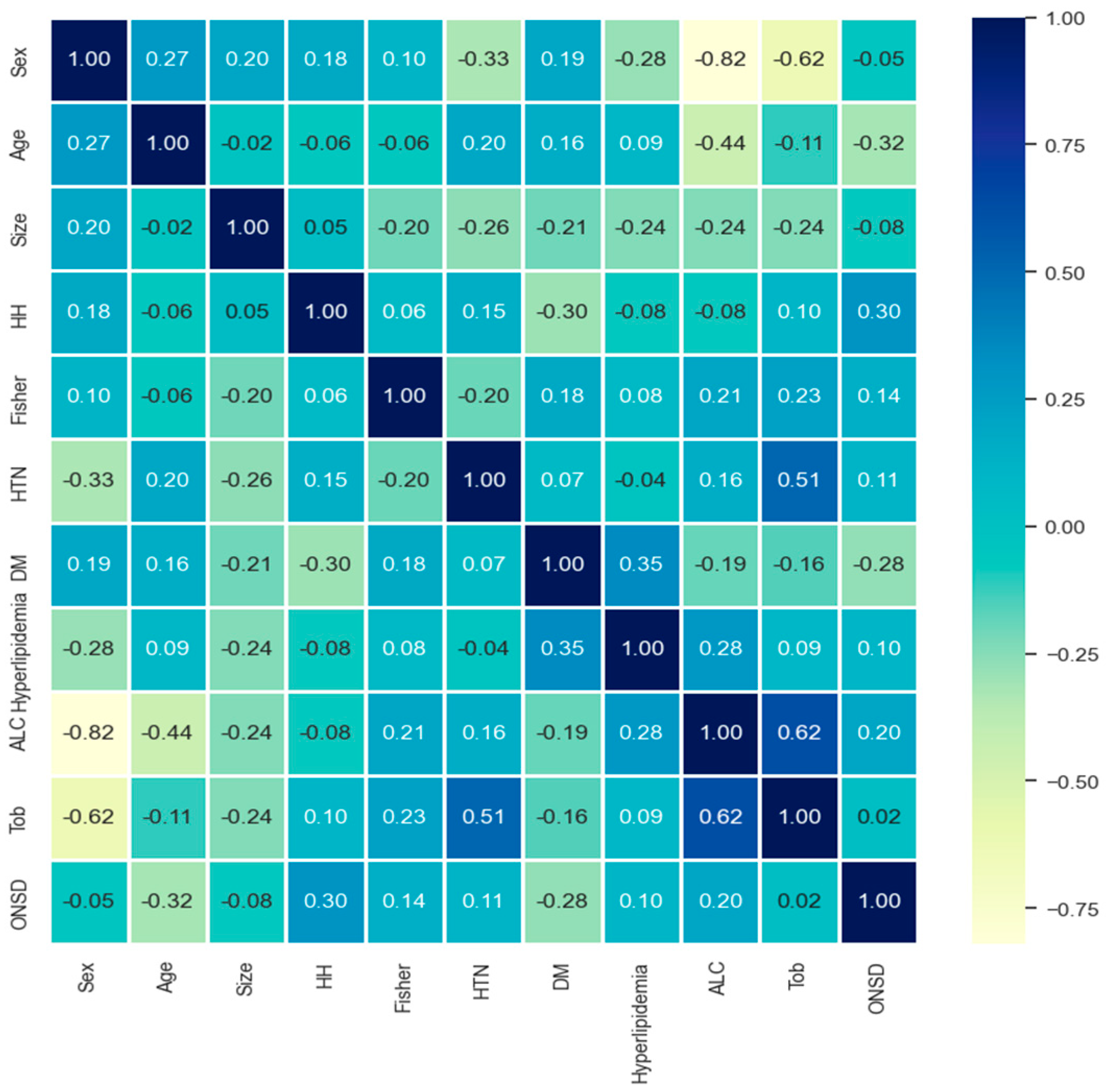
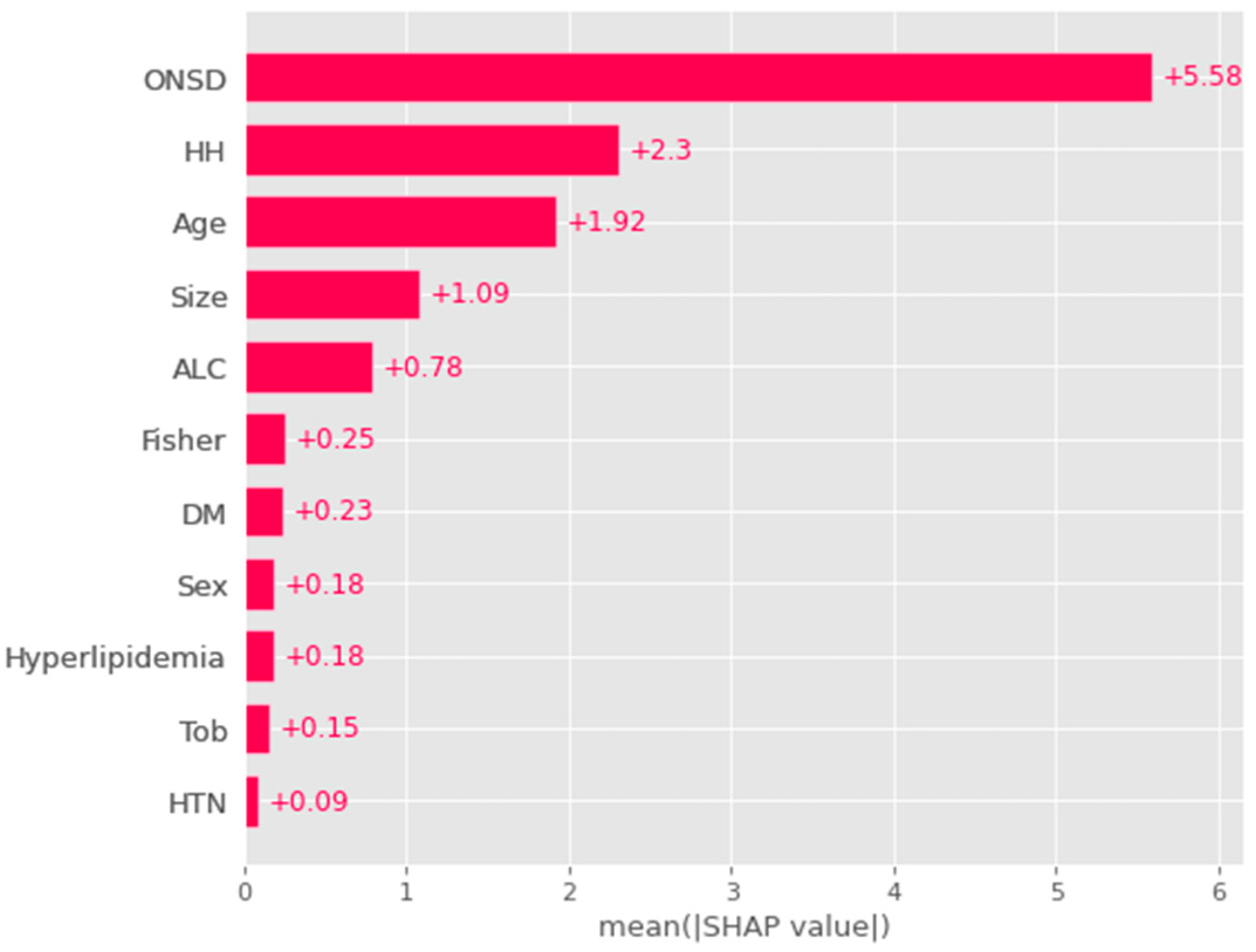
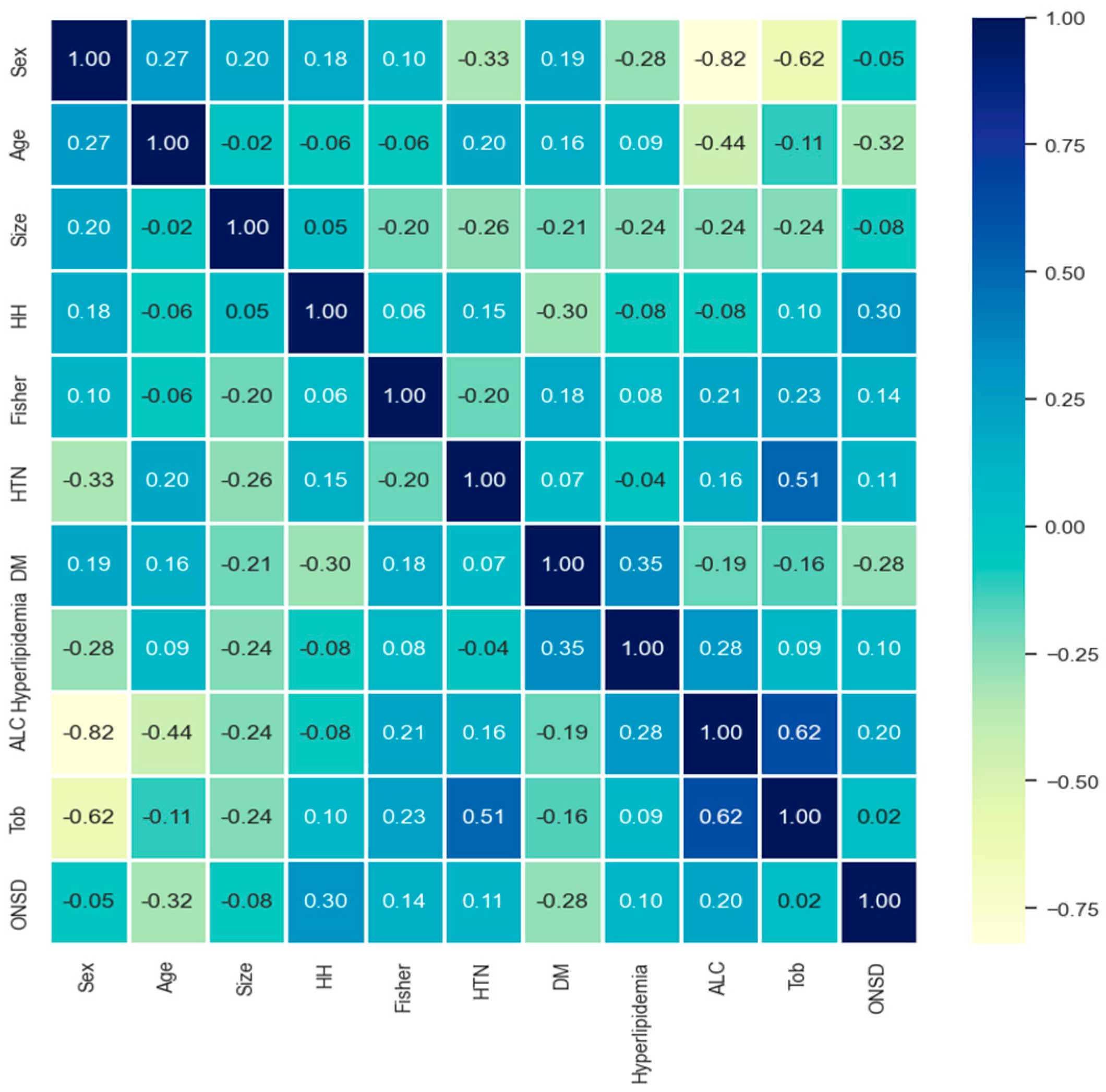
3.3. Global Feature and Correlation Analysis for the Risk Factors Related to ICP
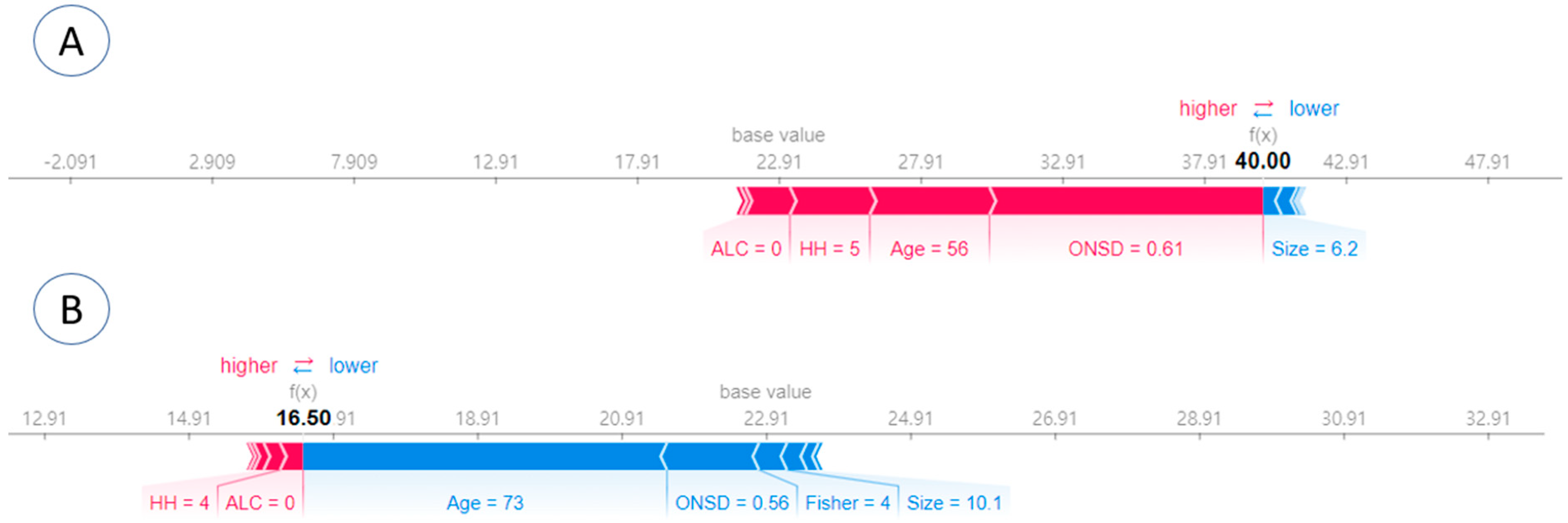
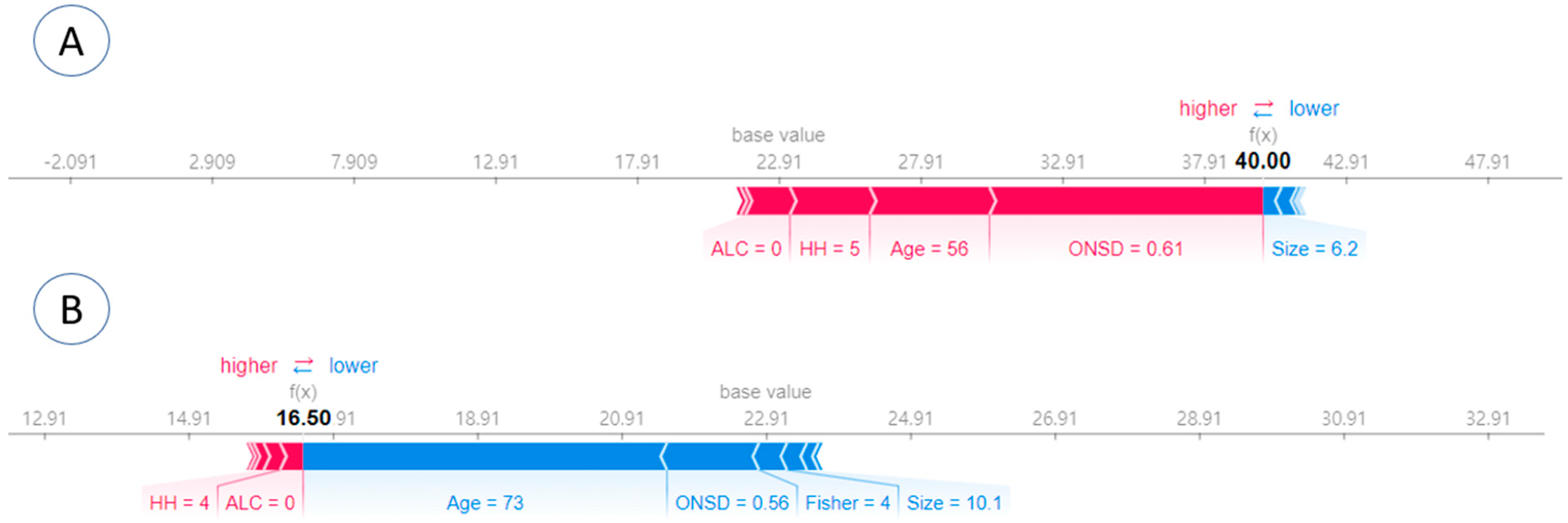
3.4. Individual SHAP Analysis Result in Each Patient
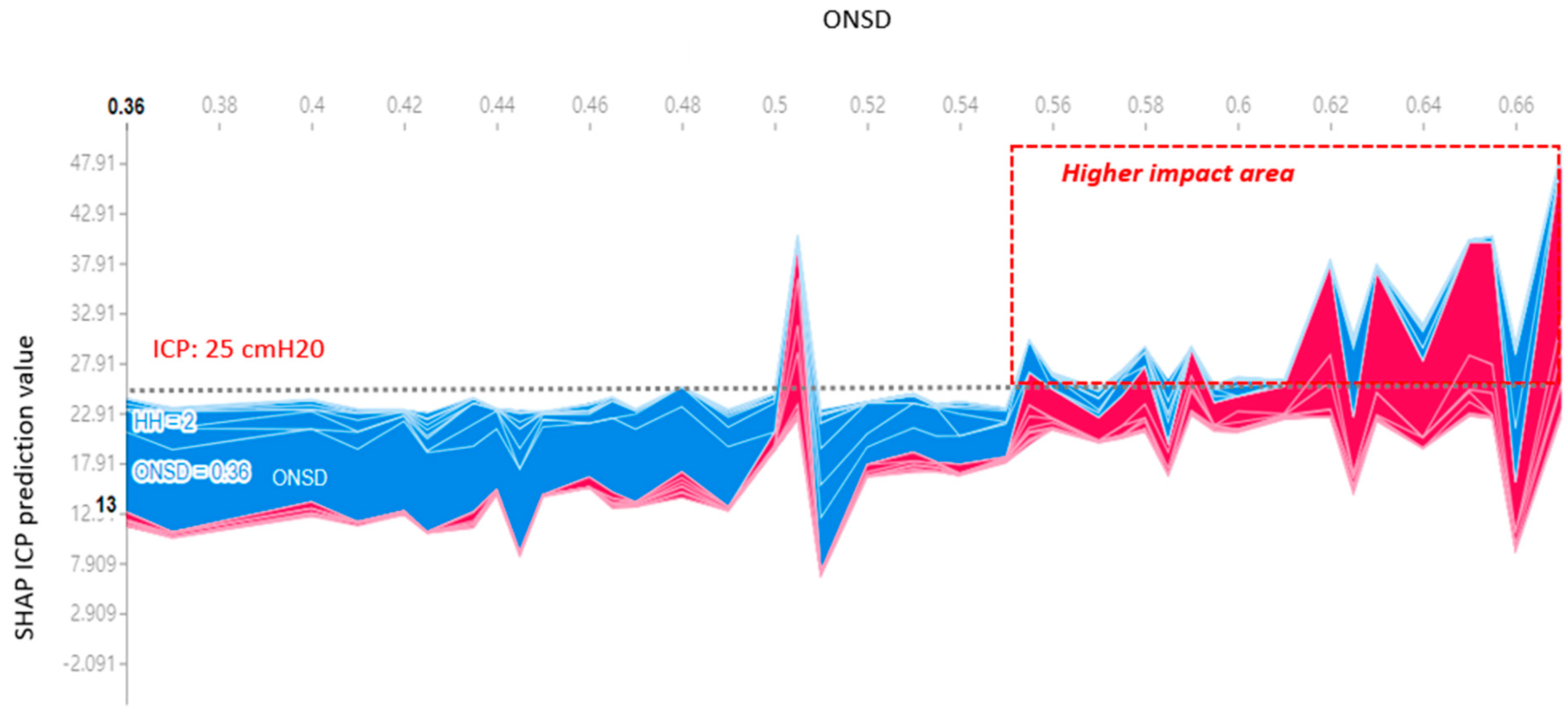
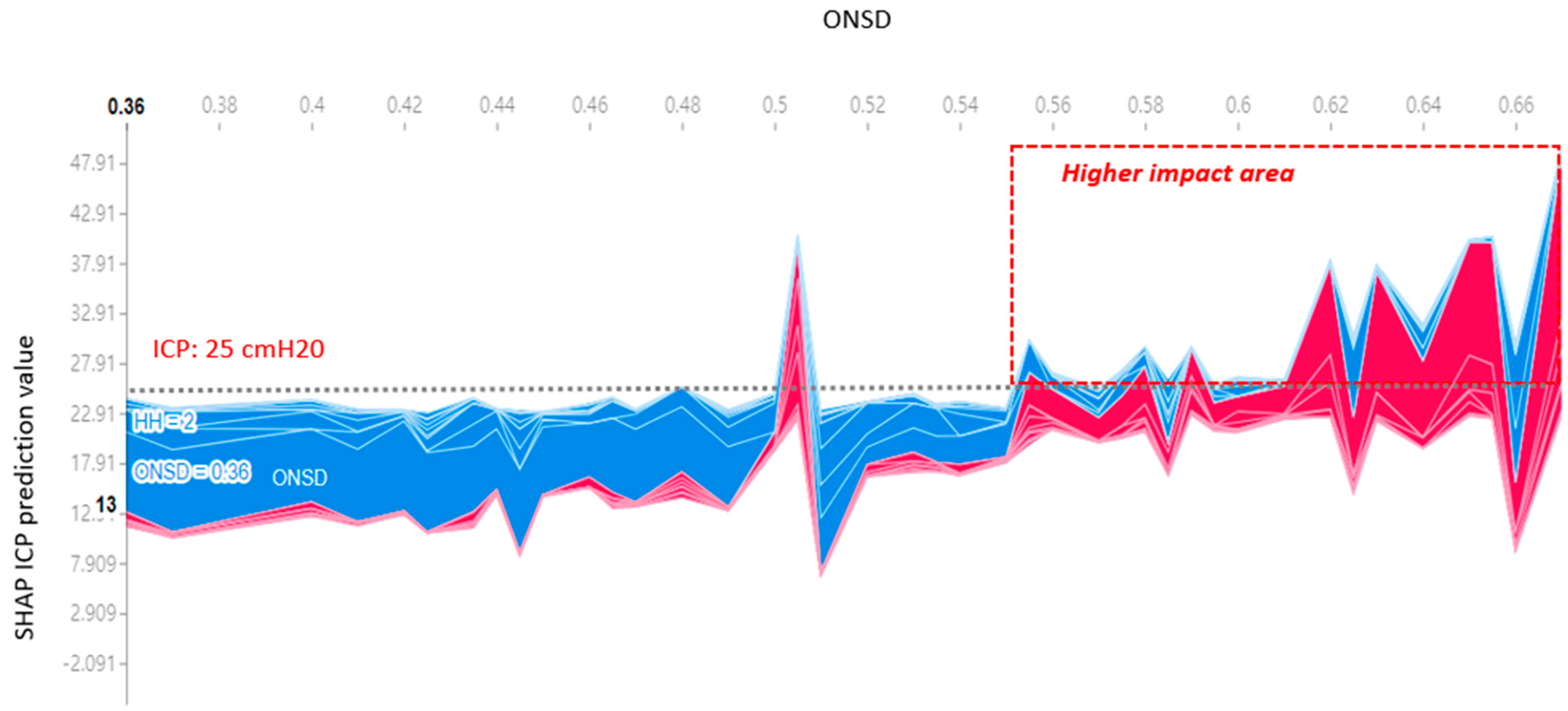
3.5. ICP Prediction Explainer for Criteria ≥ 25 cmH2O
3.6. ONSD Cutoff Values and Performance Metrics
4. Discussion
4.1. The Association between ONSD and IICP
4.2. Utilizing XAI for the Modeling of ICP
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cremer, O.L.; van Dijk, G.W.; van Wensen, E.; Brekelmans, G.J.; Moons, K.G.; Leenen, L.P.; Kalkman, C.J. Effect of intracranial pressure monitoring and targeted intensive care on functional outcome after severe head injury. Crit. Care Med. 2005, 33, 2207–2213. [Google Scholar] [CrossRef]
- Raboel, P.; Bartek, J.; Andresen, M.; Bellander, B.; Romner, B. Intracranial pressure monitoring: Invasive versus non-invasive methods—A review. Crit. Care Res. Pract. 2012, 2012, 950393. [Google Scholar] [CrossRef]
- Bratton, S.L.; Chestnut, R.M.; Ghajar, J.; Hammond, F.F.M.; Harris, O.A.; Hartl, R.; Manley, G.T.; Nemecek, A.; Newell, D.W.; Rosenthal, G.; et al. Guidelines for the management of severe traumatic brain injury. V. Deep vein thrombosis prophylaxis. J. Neurotrauma 2007, 24, S32–S36. [Google Scholar] [CrossRef]
- Harary, M.; Dolmans, R.G.; Gormley, W.B. Intracranial pressure monitoring—Review and avenues for development. Sensors 2018, 18, 465. [Google Scholar] [CrossRef]
- Kim, Y.H.; Lee, J.H.; Hong, C.K.; Cho, K.W.; Yeo, J.H.; Kang, M.J.; Kim, Y.W.; Lee, K.Y.; Kim, J.J.; Hwang, S.Y. Feasibility of optic nerve sheath diameter measured on initial brain computed tomography as an early neurologic outcome predictor after cardiac arrest. Acad. Emerg. Med. 2014, 21, 1121–1128. [Google Scholar]
- Yesilaras, M.; Kilic, T.Y.; Yesilaras, S.; Atilla, O.D.; Öncel, D.; Çamlar, M. The diagnostic and prognostic value of the optic nerve sheath diameter on CT for diagnosis spontaneous subarachnoid hemorrhage. Am. J. Emerg. Med. 2017, 35, 1408–1413. [Google Scholar] [CrossRef] [PubMed]
- Yanamandra, U.; Gupta, A.; Yanamandra, S.; Das, S.K.; Patyal, S.; Nair, V. Bedside ultrasonography as an alternative to computed tomography scan for the measurement of optic nerve sheath diameter. J. Neurosci. Rural Pract. 2018, 9, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-M.; Wang, L.-J.; Hu, Y.; Jiang, X.-H.; Wang, Y.-Z.; Xing, Y.-Q. Ultrasonic measurement of optic nerve sheath diameter: A non-invasive surrogate approach for dynamic, real-time evaluation of intracranial pressure. Br. J. Ophthalmol. 2018, 103, 437–441. [Google Scholar] [CrossRef]
- Helmke, K.; Hansen, H. Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension: II. Patient study. Pediatr. Radiol. 1996, 26, 706–710. [Google Scholar] [CrossRef]
- Koo, H.-W. Real-time change of optic nerve sheath diameter after rebleeding of ruptured intracranial dissecting aneurysm. J. Cerebrovasc. Endovasc. Neurosurg. 2020, 22, 287. [Google Scholar] [CrossRef]
- Ye, G.; Balasubramanian, V.; Li, J.K.; Kaya, M. Machine learning-based continuous intracranial pressure prediction for traumatic injury patients. IEEE J. Transl. Eng. Health Med. 2022, 10, 4901008. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, T.; Sasaki, M.; Yamaura, A. Intracranial pressure based decision making: Prediction of suspected increased intracranial pressure with machine learning. PLoS ONE 2020, 15, e0240845. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Hu, B.; Schoepf, U.; Savage, R.; Dargis, D.; Pan, C.; Li, X.; Ni, Q.; Lu, G.; Zhang, L. Artificial intelligence in the management of intracranial aneurysms: Current status and future perspectives. Am. J. Neuroradiol. 2020, 41, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Yeo, M.; Kok, H.K.; Kutaiba, N.; Maingard, J.; Thijs, V.; Tahayori, B.; Russell, J.; Jhamb, A.; Chandra, R.V.; Brooks, M. Artificial intelligence in clinical decision support and outcome prediction–applications in stroke. J. Med. Imaging Radiat. Oncol. 2021, 65, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Hilton, C.B.; Milinovich, A.; Felix, C.; Vakharia, N.; Crone, T.; Donovan, C.; Proctor, A.; Nazha, A. Personalized predictions of patient outcomes during and after hospitalization using artificial intelligence. NPJ Digit. Med. 2020, 3, 51. [Google Scholar] [CrossRef] [PubMed]
- Gunning, D. Explainable Artificial Intelligence (XAI); Defense Advanced Research Projects Agency (DARPA): Arlington, MA, USA, 2017; Volume 2, Article Number 1.
- Kim, K.H.; Koo, H.-W.; Lee, B.-J.; Sohn, M.-J. Analysis of risk factors correlated with angiographic vasospasm in patients with aneurysmal subarachnoid hemorrhage using explainable predictive modeling. J. Clin. Neurosci. 2021, 91, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Koo, H.-W.; Lee, B.-J.; Yoon, S.-W.; Sohn, M.-J. Cerebral hemorrhage detection and localization with medical imaging for cerebrovascular disease diagnosis and treatment using explainable deep learning. J. Korean Phys. Soc. 2021, 79, 321–327. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, B.-J.; Koo, H.-W. Effect of Cilostazol on Delayed Cerebral Infarction in Aneurysmal Subarachnoid Hemorrhage Using Explainable Predictive Modeling. Bioengineering 2023, 10, 797. [Google Scholar] [CrossRef] [PubMed]
- Bumberger, A.; Braunsteiner, T.; Leitgeb, J.; Haider, T. Intracranial pressure monitoring following traumatic brain injury: Evaluation of indications, complications, and significance of follow-up imaging—An exploratory, retrospective study of consecutive patients at a level I trauma center. Eur. J. Trauma Emerg. Surg. 2020, 48, 863–870. [Google Scholar] [CrossRef]
- Bäuerle, J.; Niesen, W.D.; Egger, K.; Buttler, K.J.; Reinhard, M. Enlarged optic nerve sheath in aneurysmal subarachnoid hemorrhage despite normal intracranial pressure. J. Neuroimaging 2016, 26, 194–196. [Google Scholar] [CrossRef]
- Ay, T.; Akdag, U.B.; Kilincli, M.F.; Ogut, E.; Barut, C. Anatomical variations of foramen of the diaphragma sellae and neighboring structures: A cadaveric study. Anat. Sci. Int. 2024, 99, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.P.; Lee, S.U.; Kim, S.-E.; Kang, S.H.; Yang, J.S.; Choi, H.J.; Cho, Y.J.; Ban, S.P.; Byoun, H.S.; Kim, Y.S. Correlation of optic nerve sheath diameter with directly measured intracranial pressure in Korean adults using bedside ultrasonography. PLoS ONE 2017, 12, e0183170. [Google Scholar] [CrossRef] [PubMed]
- Maissan, I.M.; Dirven, P.J.; Haitsma, I.K.; Hoeks, S.E.; Gommers, D.; Stolker, R.J. Ultrasonographic measured optic nerve sheath diameter as an accurate and quick monitor for changes in intracranial pressure. J. Neurosurg. 2015, 123, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Tayal, V.S.; Neulander, M.; Norton, H.J.; Foster, T.; Saunders, T.; Blaivas, M. Emergency department sonographic measurement of optic nerve sheath diameter to detect findings of increased intracranial pressure in adult head injury patients. Ann. Emerg. Med. 2007, 49, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Morgan, W.H.; Balaratnasingam, C.; Lind, C.R.; Colley, S.; Kang, M.H.; House, P.H.; Yu, D.-Y. Cerebrospinal fluid pressure and the eye. Br. J. Ophthalmol. 2015, 100, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Bäuerle, J.; Lochner, P.; Kaps, M.; Nedelmann, M. Intra-and interobsever reliability of sonographic assessment of the optic nerve sheath diameter in healthy adults. J. Neuroimaging 2012, 22, 42–45. [Google Scholar] [CrossRef]
- Bäuerle, J.; Schuchardt, F.; Schroeder, L.; Egger, K.; Weigel, M.; Harloff, A. Reproducibility and accuracy of optic nerve sheath diameter assessment using ultrasound compared to magnetic resonance imaging. BMC Neurol. 2013, 13, 187. [Google Scholar] [CrossRef] [PubMed]
- Lochner, P.; Coppo, L.; Cantello, R.; Nardone, R.; Naldi, A.; Leone, M.A.; Brigo, F. Intra-and interobserver reliability of transorbital sonographic assessment of the optic nerve sheath diameter and optic nerve diameter in healthy adults. J. Ultrasound 2016, 19, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Maude, R.R.; Amir Hossain, M.; Hassan, M.U.; Osbourne, S.; Sayeed, K.L.A.; Karim, M.R.; Samad, R.; Borooah, S.; Dhillon, B.; Day, N.P. Transorbital sonographic evaluation of normal optic nerve sheath diameter in healthy volunteers in Bangladesh. PLoS ONE 2013, 8, e81013. [Google Scholar] [CrossRef]
- Wang, L.; Feng, L.; Yao, Y.; Deng, F.; Wang, Y.; Feng, J.; Xing, Y. Ultrasonographic evaluation of optic nerve sheath diameter among healthy Chinese adults. Ultrasound Med. Biol. 2016, 42, 683–688. [Google Scholar] [CrossRef]
- Karami, M.; Shirazinejad, S.; Shaygannejad, V.; Shirazinejad, Z. Transocular Doppler and optic nerve sheath diameter monitoring to detect intracranial hypertension. Adv. Biomed. Res. 2015, 4, 231. [Google Scholar]
- Kim, D.H.; Jun, J.-S.; Kim, R. Ultrasonographic measurement of the optic nerve sheath diameter and its association with eyeball transverse diameter in 585 healthy volunteers. Sci. Rep. 2017, 7, 15906. [Google Scholar] [CrossRef] [PubMed]
- Ballantyne, S.; O’neill, G.; Hamilton, R.; Hollman, A. Observer variation in the sonographic measurement of optic nerve sheath diameter in normal adults. Eur. J. Ultrasound 2002, 15, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Blaivas, M.; Theodoro, D.; Sierzenski, P.R. Elevated intracranial pressure detected by bedside emergency ultrasonography of the optic nerve sheath. Acad. Emerg. Med. 2003, 10, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Geeraerts, T.; Merceron, S.; Benhamou, D.; Vigué, B.; Duranteau, J. Noninvasive assessment of intracranial pressure using ocular sonography in neurocritical care patients. Crit. Care 2008, 12, P117. [Google Scholar] [CrossRef]
- Soldatos, T.; Karakitsos, D.; Chatzimichail, K.; Papathanasiou, M.; Gouliamos, A.; Karabinis, A. Optic nerve sonography in the diagnostic evaluation of adult brain injury. Crit. Care 2008, 12, R67. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Kariman, H.; Dolatabadi, A.A.; Hatamabadi, H.R.; Derakhshanfar, H.; Mansouri, B.; Safari, S.; Eqtesadi, R. Use of the sonographic diameter of optic nerve sheath to estimate intracranial pressure. Am. J. Emerg. Med. 2013, 31, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Moretti, R.; Pizzi, B. Optic nerve ultrasound for detection of intracranial hypertension in intracranial hemorrhage patients: Confirmation of previous findings in a different patient population. J. Neurosurg. Anesthesiol. 2009, 21, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Singleton, J.; Dagan, A.; Edlow, J.A.; Hoffmann, B. Real-time optic nerve sheath diameter reduction measured with bedside ultrasound after therapeutic lumbar puncture in a patient with idiopathic intracranial hypertension. Am. J. Emerg. Med. 2014, 33, 860.e5–860.e7. [Google Scholar] [CrossRef]
- Robba, C.; Cardim, D.; Tajsic, T.; Pietersen, J.; Bulman, M.; Rasulo, F.; Bertuetti, R.; Donnelly, J.; Xiuyun, L.; Czosnyka, Z. Non-invasive intracranial pressure assessment in brain injured patients using ultrasound-based methods. In Intracranial Pressure & Neuromonitoring XVI; Springer: Cham, Switzerland, 2018; pp. 69–73. [Google Scholar]
- Lee, S.; Kim, Y.O.; Baek, J.S.; Ryu, J.-A. The prognostic value of optic nerve sheath diameter in patients with subarachnoid hemorrhage. Crit. Care 2019, 23, 65. [Google Scholar] [CrossRef]
- Zoerle, T.; Caccioppola, A.; D’Angelo, E.; Carbonara, M.; Conte, G.; Avignone, S.; Zanier, E.R.; Birg, T.; Ortolano, F.; Triulzi, F. Optic nerve sheath diameter is not related to intracranial pressure in subarachnoid hemorrhage patients. Neurocritical Care 2020, 33, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Stroh, N.; Stefanits, H.; Maletzky, A.; Kaltenleithner, S.; Thumfart, S.; Giretzlehner, M.; Drexler, R.; Ricklefs, F.L.; Dührsen, L.; Aspalter, S. Machine learning based outcome prediction of microsurgically treated unruptured intracranial aneurysms. Sci. Rep. 2023, 13, 22641. [Google Scholar] [CrossRef] [PubMed]
- Giordano, M.; D’Alessandris, Q.G.; Chiloiro, S.; Tariciotti, L.; Olivi, A.; Lauretti, L. Interpretable Machine Learning–Based Prediction of Intraoperative Cerebrospinal Fluid Leakage in Endoscopic Transsphenoidal Pituitary Surgery: A Pilot Study. J. Neurol. Surg. Part B Skull Base 2022, 83, 485–495. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | All Participants (n = 126) |
|---|---|
| Age (years) | 58.82 ± 14.86 |
| Sex [Female, n (%)] | 85 (67.46) |
| Aneurysm size (mm) | 6.93 ± 4.12 |
| Aneurysm location (n, %) | |
| ACA | 44 (34.92) |
| MCA | 18 (14.29) |
| ICA | 41 (32.54) |
| Posterior circulation | 23 (18.25) |
| Hunt–Hess grade (n, %) | |
| 1 | 0 (0.00) |
| 2 | 55 (43.65) |
| 3 | 38 (30.16) |
| 4 | 28 (22.22) |
| 5 | 5 (3.97) |
| Fisher grade (n, %) | |
| 1 | 3 (2.38) |
| 2 | 21 (16.67) |
| 3 | 24 (19.05) |
| 4 | 78 (61.90) |
| Hypertension (n, %) | 59 (46.83) |
| Diabetes (n, %) | 17 (13.49) |
| Hyperlipidemia (n, %) | 24 (19.05) |
| Smoking (n, %) | 33 (26.19) |
| Alcohol (n, %) | 39 (30.95) |
| Optic nerve sheath diameter (cm) | 0.545 ± 0.08 |
| Intracranial pressure (cmH2O) | 22.45 ± 10.28 |
| Characteristics | Patients with an ICP ≥ 20 cmH2O (n = 67) | Patients with an ICP < 20 cmH2O (n = 59) | p-Value |
|---|---|---|---|
| Age (years) | 55.33 ± 13.73 | 62.78 ± 15.20 | 0.005 |
| Sex [Female, n (%)] | 41 (61.19) | 44 (74.58) | 0.110 |
| Aneurysm size (mm) | 6.74 ± 3.76 | 7.15 ± 4.53 | 0.579 |
| Aneurysm location (n, %) | 0.09 | ||
| ACA | 28 (41.79) | 16 (27.12) | |
| MCA | 12 (17.91) | 6 (10.17) | |
| ICA | 18 (26.87) | 23 (38.98) | |
| Posterior circulation | 9 (13.43) | 14 (23.73) | |
| Hunt–Hess grade | 0.000 | ||
| 1 | 0 (0.00) | 0 (0.00) | |
| 2 | 19 (28.36) | 36 (61.02) | |
| 3 | 21 (31.34) | 17 (28.81) | |
| 4 | 23 (34.33) | 5 (8.47) | |
| 5 | 4 (5.97) | 1 (1.69) | |
| Fisher grade | 0.045 | ||
| 1 | 0 (0.00) | 3 (5.08) | |
| 2 | 8 (11.94) | 13 (22.03) | |
| 3 | 11 (16.42) | 13(22.03) | |
| 4 | 48 (71.64) | 30 (50.85) | |
| Hypertension (n) | 30 (44.78) | 29 (49.15) | 0.623 |
| Diabetes (n) | 7 (10.45) | 10 (16.95) | 0.286 |
| Hyperlipidemia (n) | 12 (17.91) | 12 (20.34) | 0.729 |
| Smoking (n) | 17 (25.37) | 16 (27.12) | 0.824 |
| Alcohol (n) | 22 (32.84) | 17 (28.81) | 0.626 |
| Optic nerve sheath diameter (cm) | 0.596 ± 0.046 | 0.486 ± 0.067 | 0.000 |
| Intracranial pressure (cmH2O) | 29.59 ± 8.97 | 14.35 ± 3.08 | 0.000 |
| Characteristics | Patients with an ICP ≥ 25 cmH2O (n = 44) | Patients with an ICP < 25 cmH2O (n = 82) | p-Value |
|---|---|---|---|
| Age (years) | 54.20 ± 14.11 | 61.29 ± 14.72 | 0.010 |
| Sex [Female, n (%)] | 24 (54.55) | 61 (74.39) | 0.023 |
| Aneurysm size (mm) | 6.63 ± 3.44 | 7.10 ± 4.46 | 0.546 |
| Aneurysm location (n, %) | 0.021 | ||
| ACA | 21 (47.73) | 23 (28.05) | |
| MCA | 9 (20.45) | 9 (10.98) | |
| ICA | 9 (20.45) | 32 (39.02) | |
| Posterior circulation | 5 (11.36) | 18 (21.95) | |
| Hunt–Hess grade | 0.000 | ||
| 1 | 0 (0.00) | 0 (0.00) | |
| 2 | 7 (15.91) | 48 (58.54) | |
| 3 | 16 (36.36) | 22 (26.83) | |
| 4 | 17 (38.64) | 11 (13.41) | |
| 5 | 4 (9.09) | 1 (1.22) | |
| Fisher grade | 0.024 | ||
| 1 | 0 (0.00) | 3 (3.66) | |
| 2 | 4 (9.09) | 17 (20.73) | |
| 3 | 5 (11.36) | 19 (23.17) | |
| 4 | 35 (79.55) | 43 (52.44) | |
| Hypertension (n) | 21 (47.73) | 38 (46.34) | 0.882 |
| Diabetes (n) | 4 (9.09) | 13 (15.85) | 0.289 |
| Hyperlipidemia (n) | 10 (22.73) | 14 (17.07) | 0.441 |
| Smoking (n) | 11 (25.00) | 22 (26.83) | 0.824 |
| Alcohol (n) | 17 (38.64) | 22 (26.83) | 0.172 |
| Optic nerve sheath diameter (cm) | 0.61 ± 0.035 | 0.51 ± 0.075 | 0.000 |
| Intracranial pressure (cmH2O) | 33.84 ± 8.28 | 16.34 ± 4.20 | 0.000 |
| ICP (cmH2O) | AUC | 95% CI | ONSD Cutoff Value (cm) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|---|
| ≥20 | 0.90 | 0.85–0.96 | 0.545 | 92.50 | 78.00 | 82.70 | 90.20 |
| ≥25 | 0.87 | 0.81–0.93 | 0.553 | 95.50 | 67.10 | 60.90 | 96.50 |
| Model | RMSE | MAE | MAPE |
|---|---|---|---|
| Linear regression | 2.64 | 5.77 | 0.36 |
| XGBoost regression | 2.74 | 6.26 | 0.42 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.H.; Kang, H.K.; Koo, H.-W. Prediction of Intracranial Pressure in Patients with an Aneurysmal Subarachnoid Hemorrhage Using Optic Nerve Sheath Diameter via Explainable Predictive Modeling. J. Clin. Med. 2024, 13, 2107. https://doi.org/10.3390/jcm13072107
Kim KH, Kang HK, Koo H-W. Prediction of Intracranial Pressure in Patients with an Aneurysmal Subarachnoid Hemorrhage Using Optic Nerve Sheath Diameter via Explainable Predictive Modeling. Journal of Clinical Medicine. 2024; 13(7):2107. https://doi.org/10.3390/jcm13072107
Chicago/Turabian StyleKim, Kwang Hyeon, Hyung Koo Kang, and Hae-Won Koo. 2024. "Prediction of Intracranial Pressure in Patients with an Aneurysmal Subarachnoid Hemorrhage Using Optic Nerve Sheath Diameter via Explainable Predictive Modeling" Journal of Clinical Medicine 13, no. 7: 2107. https://doi.org/10.3390/jcm13072107
APA StyleKim, K. H., Kang, H. K., & Koo, H.-W. (2024). Prediction of Intracranial Pressure in Patients with an Aneurysmal Subarachnoid Hemorrhage Using Optic Nerve Sheath Diameter via Explainable Predictive Modeling. Journal of Clinical Medicine, 13(7), 2107. https://doi.org/10.3390/jcm13072107