
Cognitive Effects of Reducing First-Generation Antipsychotic Dose Compared to Switching to Ziprasidone in Long-Stay Patients with Schizophrenia

Abstract
1. Introduction
2. Materials and Methods
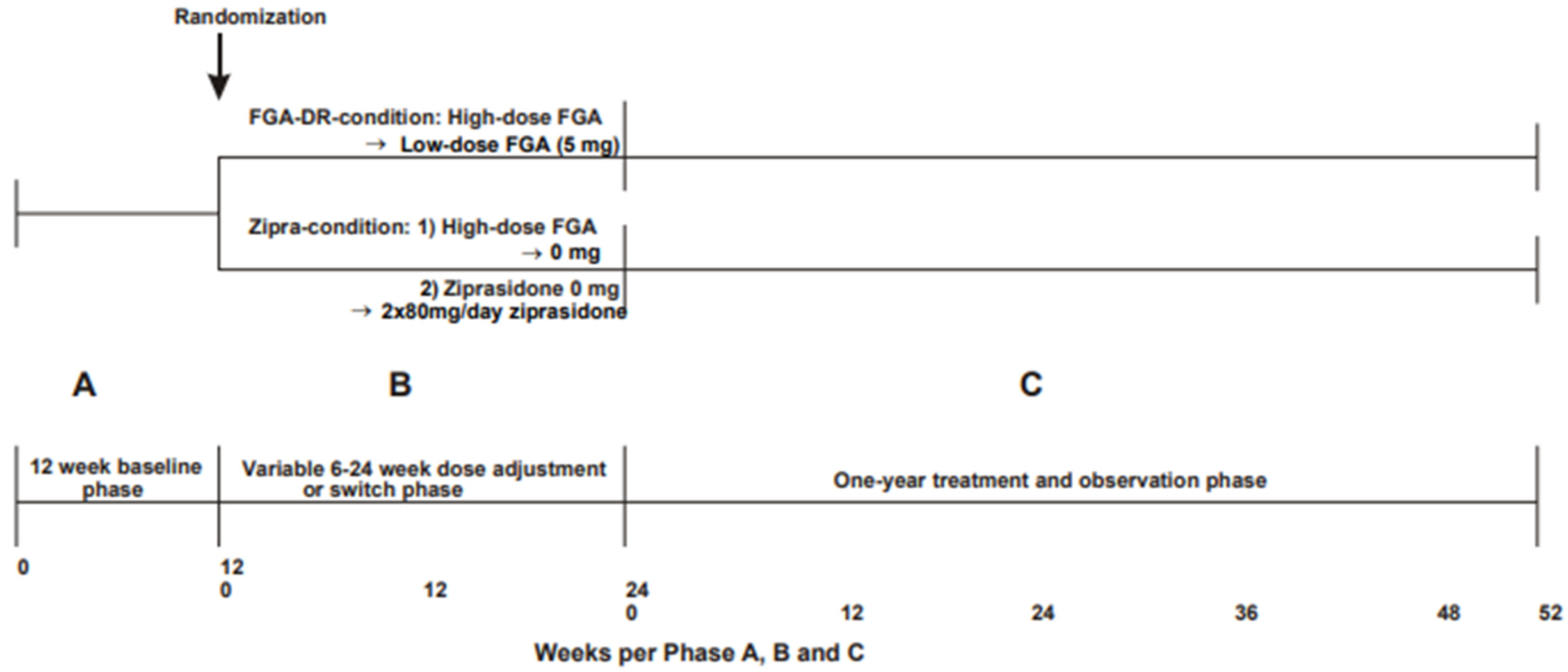
2.1. Study Design
2.2. Study Participants
2.3. Drug Regimen and Assessments
2.4. Clinical Assessments
2.5. Analysis
2.6. Ethical Standard
3. Results
3.1. Patients
3.2. Patient Characteristics
3.3. Does Reducing the Dose of FGAs Improve Cognitive Function?
3.4. Does Switching to Ziprasidone Have a Superior Effect on Cognitive Function Than FGA Dose Reduction?
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schaefer, J.; Giangrande, E.; Weinberger, D.R.; Dickinson, D. The global cognitive impairment in schizophrenia: Consistent over decades and around the world. Schizophr. Res. 2013, 150, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Fett, A.; Reichenberg, A.; Velthorst, E. Lifespan evolution of neurocognitive impairment in schizophrenia—A narrative review. Schizophr. Res. Cogn. 2013, 28, 100237. [Google Scholar] [CrossRef] [PubMed]
- Jonas, K.; Lian, W.; Callahan, J.; Ruggero, C.J.; Clouston, S.; Reichenberg, A.; Carlson, G.A.; Bromet, E.J.; Kotov, R. The course of general cognitive ability in individuals with psychotic disorders. JAMA Psychiatry 2022, 79, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Kern, R.S.; Heaton, R.K. Longitudinal studies of cognition and functional outcome in schizophrenia: Implications for MATRICS. Schizophr. Res. 2004, 72, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Fatouros-Bergman, H.; Cervenka, S.; Flyckt, L.; Edman, G.; Farde, L. Meta-analysis of cognitive performance in drug-naïve patients with schizophrenia. Schizophr. Res. 2014, 158, 156–162. [Google Scholar] [CrossRef]
- Freedman, D.; Brown, A.S. The developmental course of executive functioning in schizophrenia. Int. J. Dev. Neurosci. 2011, 29, 237–243. [Google Scholar] [PubMed]
- Orellana, G.; Slachevsky, A. Executive functioning in schizophrenia. Front. Psychiatry 2013, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Green, M.F.; Harvey, P.D. Cognition in schizophrenia: Past, present, and future. Schizophr. Res. Cogn. 2014, 1, e1–e9. [Google Scholar] [CrossRef]
- Sharma, T. Impact on cognition of the use of antipsychotics. Curr. Med. Res. Opin. 2002, 18 (Suppl. 3), s13–s17. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Cognition in schizophrenia: Impairments, determinants, and functional importance. Psychiatr. Clin. N. Am. 2005, 28, 613–633. [Google Scholar] [CrossRef]
- Blackman, R.K.; Dickingson, D.; Eisenberg, D.P.; Gregory, M.D.; Apud, J.A.; Berman, K.F. Antipsychotic medication-mediated cognitive change in schizophrenia and polygenic score for cognitive ability. Schizophr. Res. Cogn. 2022, 27, 100223. [Google Scholar] [CrossRef] [PubMed]
- Keefe, R.S.; Bilder, R.M.; Davis, S.M.; Harvey, P.D.; Palmer, B.W.; Gold, J.M.; Meltzer, H.Y.; Green, M.F.; Capuano, G.; Stroup, T.S.; et al. Neurocognitive effects of antipsychotic medications in patients with chronic schizophrenia in the CATIE trial. Arch. Gen. Psychiatry 2007, 64, 633–647. [Google Scholar] [CrossRef]
- Davidson, M.; Galderisi, S.; Weiser, M.; Werbeloff, N.; Fleischhacker, W.W.; Keefe, R.S.; Boter, H.; Keet, I.P.M.; Prelipceanu, D.; Rybakowski, J.K.; et al. Cognitive effects of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: A randomized open-label clinical trial (EUFEST). Am. J. Psychiatry 2009, 166, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Désaméricq, G.; Schurhoff, F.; Meary, A.; Szöke, A.; Macquin-Mavier, I.; Bachoud-Lévi, A.C.; Maison, P. Long-term neurocognitive effects of antipsychotics in schizophrenia: A network meta-analysis. Eur. J. Clin. Pharmacol. 2014, 70, 127–134. [Google Scholar] [CrossRef]
- Hsu, W.-Y.; Lane, H.-Y.; Lin, C.-H. Medications used for cognitive enhancement in patients with schizophrenia, bipolar disorder, Alzheimer’s disease, and Parkinson’s disease. Front. Psychiatry 2018, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Keefe, R.S.; Sweeney, J.A.; Gu, H.; Hamer, R.M.; Perkins, D.O.; McEvoy, J.P.; Lieberman, J.A. Effects of olanzapine, quetiapine, and risperidone on neurocognitive function in early psychosis: A randomized, double-blind 52-week comparison. Am. J. Psychiatry 2007, 164, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; Fagerlund, B.; Rasmussen, H.; Ebdrup, B.H.; Aggernaes, B.; Gade, A.; Oranje, B.; Glenthoj, B. Cognitive effects of six months of treatment with quetiapine, in antipsychotic-naïve first-episode schizophrenia. Psychiatry Res. 2011, 187, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D. Ziprasidone and cognition: The evolving story. J. Clin. Psychiatry 2003, 64 (Suppl. 19), 33–39. [Google Scholar]
- Baldez, D.P.; Biazus, T.B.; Rabelo-da-Ponte, D.R.; Nogaro, G.P.; Martins, D.S.; Kunz, M.; Czepielewski, L.S. The effect of antipsychotics on the cognitive performance of individuals with psychotic disorders: Network meta-analyses of randomized controlled trials. Neurosci. Biobehav. Rev. 2021, 126, 265–275. [Google Scholar] [CrossRef]
- van Veelen, N.M.J.; Grootens, K.P.; Peuskens, J.; Sabbe, B.G.C.; Salden, M.E.; Verkes, R.J.; Kahn, R.S.; Sitskoorn, M.M. Short term neurocognitive effects of treatment with ziprasidone and olanzapine in recent onset schizophrenia. Schizophr. Res. 2010, 120, 191–198. [Google Scholar] [CrossRef]
- Johnson, E.; Jørgensen, H.A.; Kroken, R.A.; Løberg, E.M. Neurocognitive effectiveness of quetiapine, olanzapine, risperidone, and ziprasidone: A pragmatic, randomized trial. Eur. Psychiatry 2013, 28, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhang, Z.H.; Song, Y.; Yuan, W.; Liu, Z.X.; Tang, M.Q. A paired case-control comparison of ziprasidone on visual sustained attention and visual selective attention in patients with paranoid schizophrenia. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2952–2956. [Google Scholar] [PubMed]
- Harvey, P.D.; Meltzer, H.; Simpson, G.M.; Potkin, S.G.; Loebel, A.; Siu, C.; Romano, S.J. Improvement in cognitive function following a switch to ziprasidone from conventional antipsychotics, olanzapine, or risperidone in outpatients with schizophrenia. Schizophr. Res. 2004, 66, 101–113. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D.; Siu, C.O.; Romano, S. Randomized, controlled, double-blind, multicenter comparison of the cognitive effects of ziprasidone versus olanzapine in acutely ill inpatients with schizophrenia or schizoaffective disorder. Psychopharmacology 2004, 172, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.K.; Burdick, K.E.; Razi, K.; Bates, J.A.; Sanders, M.; Kane, J.M. Ziprasidone-induced cognitive enhancement in schizophrenia: Specificity or pseudospecificity? Schizophr. Res. 2006, 87, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Harvey, P.D.; Sacchetti, E.; Galluzzo, A.; Romeo, F.; Gorini, B.; Bilder, R.M.; Loebel, A.D. A randomized double-blind comparison of ziprasidone vs. clozapine for cognition in patients with schizophrenia selected for resistance or intolerance to previous treatment. Schizophr. Res. 2008, 105, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Gibel, A.; Ritsner, M.S. Neurocognitive effects of ziprasidone and related factors in patients with chronic schizophrenia undergoing usual care: A 12-month, open-label, flexible-dose, naturalistic observational trial. Clin. Neuropharmacol. 2008, 31, 204–219. [Google Scholar] [CrossRef] [PubMed]
- Ballesteros, A.; Sánchez-Torres, A.M.; López-Ilundain, J.M.; Cabrera, B.; Lobo, A.; González-Pinto, A.M.; Díaz-Caneja, C.; Corripio, I.; Vieta, E.; de la Serna, E.; et al. Is cognitive impairment associated with antipsychotic dose and anticholinergic equivalent loads in first-episode psychosis? Psychol. Med. 2018, 48, 2247–2256. [Google Scholar] [CrossRef]
- Singh, A.; Kumar, V.; Pathak, H.; Jacob, A.A.; Venkatasubramanian, G.; Varambally, S.; Rao, N.P. Effect of antipsychotic dose reduction on cognitive function in schizophrenia. Psychiatry Res. 2022, 308, 114383. [Google Scholar] [CrossRef]
- Seeman, P. Dopamine D2 receptors as treatment targets in schizophrenia. Clin. Schizophr. Relat. Psychoses 2010, 3, 56–73. [Google Scholar] [CrossRef]
- Buckley, P.F.; Correll, C.U. Strategies for dosing and switching antipsychotics for optimal clinical management. J. Clin. Psychiatry 2008, 69 (Suppl. 1), 4–17. [Google Scholar]
- Andreasen, N.C.; Pressler, M.; Nopoulos, P.; Miller, D.; Ho, B.-C. Antipsychotic dose equivalents and dose-years: A standardized method for comparing exposure to different drugs. Biol. Psychiatry 2010, 67, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Gardner, D.M.; Murphy, A.L.; O’Donnell, H.; Centorrino, F.; Baldessarini, R.J. International consensus study of antipsychotic dosing. Am. J. Psychiatry 2010, 167, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Bogers, J.P.A.M.; Schulte, P.F.J.; Broekman, T.G.; Moleman, P.; de Haan, L. Dose-reduction of high-dose first-generation antipsychotics or switch to ziprasidone in long-stay patients with schizophrenia: A 1 year double-blind randomized clinical trial. Eur. Neuropsychopharmacol. 2018, 28, 1024–1034. [Google Scholar] [CrossRef] [PubMed]
- McLeod, S.A. What Does Effect Size Tell You? Simply Psychology, 31 July 2023. Available online: https://www.simplypsychology.org/effect-size.html (accessed on 19 August 2023).
- van Aken, B.C.; Wierdsma, A.I.; Voskes, Y.; Pijnenborg, G.H.M.; van Weeghel, J.; Mulder, C.L. The association between executive functioning and personal recovery in people with psychotic disorders. Schizophr. Bull Open 2022, 3, sgac023. [Google Scholar] [CrossRef]
- Horowitz, M.A.; Moncrieff, J.; de Haan, L.; Bogers, J.P.A.M.; Gangarin, S.S.; Kikkert, M.; Veling, W.; Sommer, I.E.C. Tapering antipsychotic medication: Practical considerations. Psychol. Med. 2022, 52, 32–35. [Google Scholar] [CrossRef]
- Woodward, N.D.; Purdon, S.E.; Meltzer, H.Y.; Zald, D.H. A meta-analysis of cognitive change with haloperidol in clinical trials of atypical antipsychotics: Dose effects and comparison to practice effects. Schizophr. Res. 2007, 89, 211–224. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Cognitive Domain: | Test: | Number of Participants | ||
|---|---|---|---|---|
| Total Group | FGA-DR Condition | ZIPRA Condition | ||
| 1. Speed of processing information | Symbol digit modalities test Stroop color word test, card 1 Trail making test part A | 18 19 20 | 7 9 9 | 11 10 11 |
| 2. Attention and vigilance | Continuous performance test | 11 | 5 | 6 |
| 3. Working memory | Digits forward Digits backward | 23 | 10 | 13 |
| 4. Verbal learning | 15 words test (Rey auditory verbal learning test) | 21 | 9 | 12 |
| 5. Executive functions | Verbal fluency tests Stroop interference (cards 2 and 3) Trail making test part B | 21 19 20 | 9 9 9 | 12 10 11 |
| FGA-DR Condition (n = 10) | ZIPRA Condition (n = 13) | |
|---|---|---|
| Male in numbers (%) | 7 (70) | 6 (46) |
| Mean age in years (SD) | 50.00 (17.51) | 52.62 (14.09) |
| Mean time (years) in the hospital (SD) | 17.38 (10.62) | 18.67 (12.94) |
| Mean time (years) of antipsychotic use | 17.38 (10.62) | 19.33 (12.63) |
| Dose equivalents in mg/day of haloperidol before dose reduction/switch (SD) | 16.95 (15.98) | 13.37 (9.56) |
| Mean PANSS total score (SD) | 103.6 (10.68) | 96.54 (7.21) |
| Total Group of Patients | FGA-DR Condition | Ziprasidone Condition | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median | ∆T0-T1 | Median | ∆T0-T1 | Median | ∆T0-T1 | ||||||||||
| Domains | T0 | T1 | Z | r | p | T0 | T1 | Z | r | p | T0 | T1 | Z | r | p |
| 1. Speed of processing information | |||||||||||||||
| Symbol Digits MT | 18.0 | 12.0 | −2.25 | −0.53 | 0.24 | 18.0 | 12.0 | −1.36 | −0.51 | 0.17 | 18.0 | 12.0 | −1.78 | −0.53 | 0.08 |
| Stroop Chart 1 | 80.0 | 80.0 | −0.47 | −0.11 | 0.64 | 80.0 | 80.0 | −0.71 | −0.24 | 0.48 | 88.5 | 76.0 | −0.28 | −0.08 | 0.78 |
| Trail Making Test A | 94.0 | 96.5 | −0.73 | −0.16 | 0.47 | 94.0 | 114.0 | −0.53 | −0.18 | 0.59 | 94.0 | 88.0 | −0.71 | −0.21 | 0.48 |
| 2. Attention and vigilance | |||||||||||||||
| Continuous Performance | 698.0 | 647.0 | −0.80 | −0.24 | 0.42 | 605.0 | 727.0 | −0.67 | −0.29 | 0.50 | 826.5 | 622.5 | −0.94 | −0.38 | 0.35 |
| 3. Working memory | |||||||||||||||
| Digits Forward | 5.0 | 5.0 | −1.03 | −0.21 | 0.30 | 5.0 | 4.5 | −0.36 | −0.11 | 0.72 | 5.0 | 5.0 | −1.29 | −0.36 | 0.20 |
| Digits Backward | 3.0 | 3.0 | −1.44 | −0.30 | 0.15 | 3.0 | 3.0 | −1.61 | −0.50 | 0.11 | 4.0 | 3.0 | −0.52 | −0.14 | 0.61 |
| 4. Verbal learning | |||||||||||||||
| 15 Words Test Total | 20.0 | 21.0 | −1.15 | −0.24 | 0.25 | 19.0 | 16.0 | −0.36 | −0.12 | 0.72 | 21.0 | 22.0 | −1.10 | −0.31 | 0.27 |
| 15 Words Test Recall | 3.0 | 4.0 | −1.21 | −0.26 | 0.23 | 3.0 | 3.0 | −0.11 | −0.03 | 0.92 | 2.5 | 4.0 | −1.50 | −0.43 | 0.14 |
| 15 Words Test Recognition | 13.0 | 12.0 | −1.62 | −0.35 | 0.11 | 13.0 | 11.0 | −2.13 | −0.71 | 0.33 | 12.5 | 12.5 | −0.36 | −0.11 | 0.72 |
| 5. Executive function | |||||||||||||||
| Verbal fluency Letter N | 5.0 | 4.0 | −0.65 | −0.14 | 0.52 | 3.0 | 3.0 | −0.21 | −0.07 | 0.83 | 5.0 | 5.0 | −1.12 | −0.32 | 0.27 |
| Verbal fluency Letter A | 3.0 | 3.0 | −0.69 | −0.15 | 0.49 | 3.0 | 2.0 | −2.16 | −0.72 | 0.31 | 4.0 | 5.5 | −1.29 | −0.37 | 0.20 |
| Verbal fluency Animals | 10.0 | 9.0 | −1.14 | −0.25 | 0.26 | 10.0 | 8.0 | −1.56 | −0.52 | 0.12 | 8.5 | 12.5 | −2.50 | −0.72 | 0.01 * |
| Verbal fluency Occupations | 5.0 | 5.0 | −0.88 | −0.19 | 0.38 | 4.0 | 5.0 | −0.68 | −0.23 | 0.50 | 5.5 | 6.0 | −1.58 | −0.46 | 0.12 |
| Stroop Interference Score | 80.0 | 83.0 | −0.21 | −0.05 | 0.83 | 96.0 | 71.0 | −0.42 | −0.14 | 0.68 | 75.0 | 80.0 | −0.14 | −0.04 | 0.89 |
| Trail Making Test B | 346.0 | 287.0 | −1.23 | −0.28 | 0.22 | 342.0 | 269.0 | −0.42 | −0.14 | 0.68 | 351.0 | 305.0 | −1.42 | −0.43 | 0.16 |
| ∆T0-T1 | |||||
|---|---|---|---|---|---|
| Median Difference | |||||
| FGA | Ziprasidone | Z | r | p | |
| 1. Speed of information processing | |||||
| Symbol Digits MT | −2.00 | −5.00 | −0.18 | −0.04 | 0.86 |
| Stroop Chart 1 | −6.00 | −5.00 | −0.96 | −0.22 | 0.92 |
| Trail Making Test A | −12.00 | −13.00 | −0.49 | −0.11 | 0.62 |
| 2. Attention and vigilance | |||||
| Continuous Performance | 17.00 | −207.00 | −1.46 | −0.44 | 0.14 |
| 3. Working memory | |||||
| Digits Forward | −5.00 | 0.00 | −0.60 | −0.12 | 0.55 |
| Digits Backward | −2.00 | −1.00 | −1.01 | −0.21 | 0.31 |
| 4. Verbal learning | |||||
| 15 Words Test Total | 3.00 | 7.50 | −0.82 | −0.18 | 0.41 |
| 15 Words Test Recall | 0.00 | 0.50 | −0.83 | −0.18 | 0.41 |
| 15 Words Test Recognition | −2.00 | 0.00 | −1.22 | −0.26 | 0.22 |
| 5. Executive function | |||||
| Verbal Fluency Letter N | 0.00 | 1.00 | −0.54 | −0.12 | 0.59 |
| Verbal Fluency Letter A | −2.00 | 0.00 | −2.50 | −0.54 | 0.01 * |
| Verbal Fluency Animals | −1.00 | 2.50 | −1.55 | −0.33 | 0.12 |
| Verbal Fluency Occupations | 0.00 | 1.00 | −2.72 | −0.59 | 0.07 |
| Stroop Interference Score | 1.00 | 5.00 | −0.48 | −0.11 | 0.63 |
| Trail Making Test B | −28.00 | −71.00 | −0.61 | −0.14 | 0.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogers, J.P.A.M.; Blömer, J.A.; de Haan, L. Cognitive Effects of Reducing First-Generation Antipsychotic Dose Compared to Switching to Ziprasidone in Long-Stay Patients with Schizophrenia. J. Clin. Med. 2024, 13, 2112. https://doi.org/10.3390/jcm13072112
Bogers JPAM, Blömer JA, de Haan L. Cognitive Effects of Reducing First-Generation Antipsychotic Dose Compared to Switching to Ziprasidone in Long-Stay Patients with Schizophrenia. Journal of Clinical Medicine. 2024; 13(7):2112. https://doi.org/10.3390/jcm13072112
Chicago/Turabian StyleBogers, Jan P. A. M., Jasper A. Blömer, and Lieuwe de Haan. 2024. "Cognitive Effects of Reducing First-Generation Antipsychotic Dose Compared to Switching to Ziprasidone in Long-Stay Patients with Schizophrenia" Journal of Clinical Medicine 13, no. 7: 2112. https://doi.org/10.3390/jcm13072112
APA StyleBogers, J. P. A. M., Blömer, J. A., & de Haan, L. (2024). Cognitive Effects of Reducing First-Generation Antipsychotic Dose Compared to Switching to Ziprasidone in Long-Stay Patients with Schizophrenia. Journal of Clinical Medicine, 13(7), 2112. https://doi.org/10.3390/jcm13072112