
Effect of an Intensive Lifestyle Intervention on Circulating Biomarkers of Atrial Fibrillation-Related Pathways among Adults with Metabolic Syndrome: Results from a Randomized Trial
 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Methods
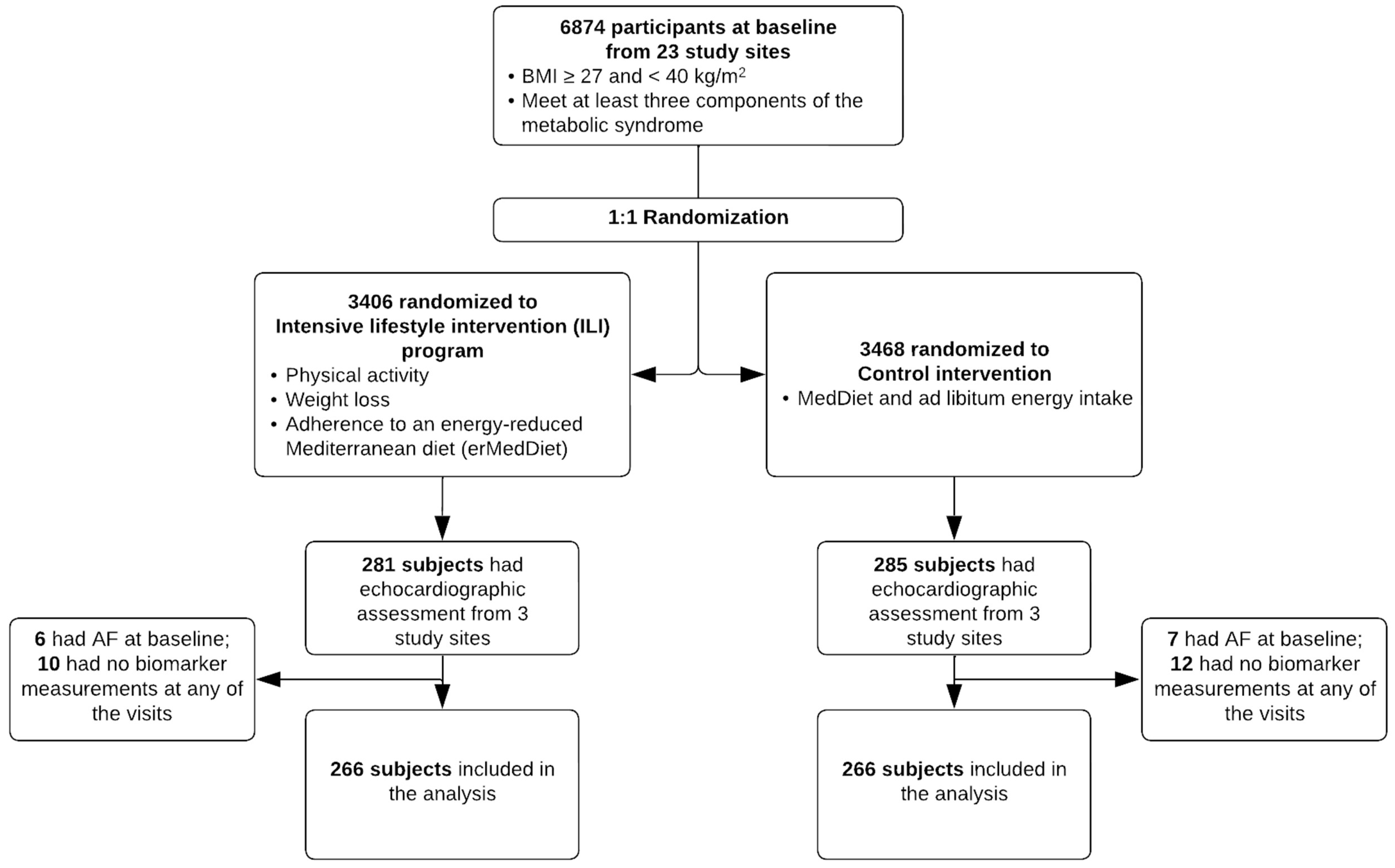
2.1. Study Design and Population
2.2. Intervention Components and Outcome Measures
2.3. Other Covariates
2.4. Sample Size Estimation
2.5. Statistical Analysis
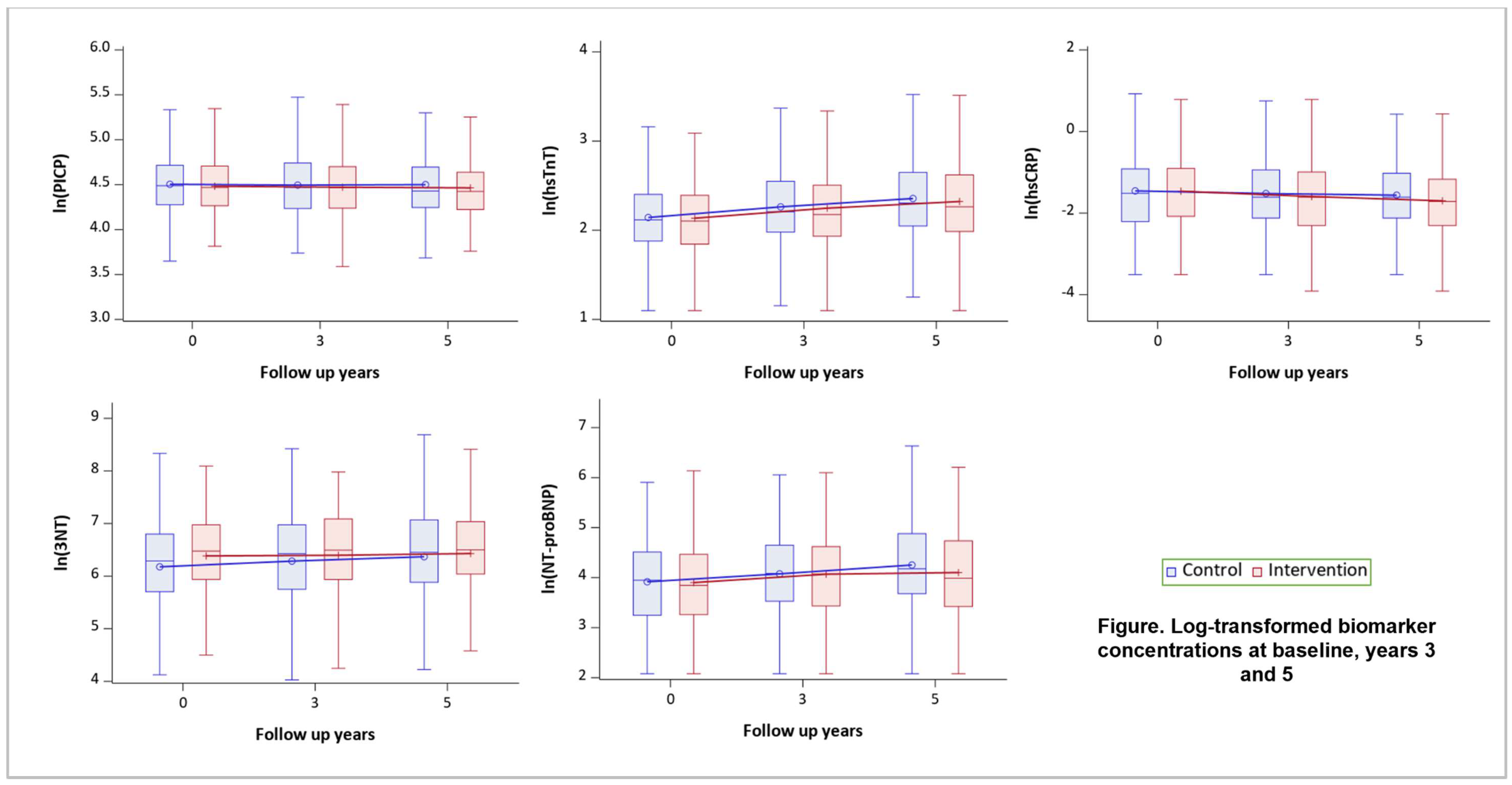
3. Results
3.1. Mediation Analysis
3.2. Stratified Analysis
3.3. Sensitivity Analysis
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alonso, A.; Agarwal, S.K.; Soliman, E.Z.; Ambrose, M.; Chamberlain, A.M.; Prineas, R.J.; Folsom, A.R. Incidence of atrial fibrillation in whites and African-Americans: The Atherosclerosis Risk in Communities (ARIC) study. Am. Heart J. 2009, 158, 111–117. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [PubMed]
- Global Burden of Disease Study. University of Washington. Available online: https://ghdx.healthdata.org/ (accessed on 1 December 2022).
- Colilla, S.; Crow, A.; Petkun, W.; Singer, D.E.; Simon, T.; Liu, X. Estimates of Current and Future Incidence and Prevalence of Atrial Fibrillation in the U.S. Adult Population. Am. J. Cardiol. 2013, 112, 1142–1147. [Google Scholar] [CrossRef]
- Magnussen, C.; Niiranen, T.J.; Ojeda, F.M.; Gianfagna, F.; Blankenberg, S.; Njølstad, I.; Vartiainen, E.; Sans, S.; Pasterkamp, G.; Hughes, M.; et al. Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: Results from the BiomarCaRE Consortium (Biomarker for Cardiovascular Risk Assessment in Europe). Circulation 2017, 136, 1588–1597. [Google Scholar] [CrossRef] [PubMed]
- Mou, L.; Norby, F.L.; Chen, L.Y.; O’Neal, W.T.; Lewis, T.T.; Loehr, L.R.; Soliman, E.Z.; Alonso, A. Lifetime Risk of Atrial Fibrillation by Race and Socioeconomic Status: ARIC Study (Atherosclerosis Risk in Communities). Circ. Arrhythmia Electrophysiol. 2018, 11, e006350. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Magnani, J.W.; Norby, F.L.; Agarwal, S.K.; Soliman, E.Z.; Chen, L.Y.; Loehr, L.R.; Alonso, A. Racial Differences in Atrial Fibrillation-Related Cardiovascular Disease and Mortality. JAMA Cardiol. 2016, 1, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Haïssaguerre, M.; Jaïs, P.; Shah, D.C.; Takahashi, A.; Hocini, M.; Quiniou, G.; Garrigue, S.; Le Mouroux, A.; Le Métayer, P.; Clémenty, J. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N. Engl. J. Med. 1998, 339, 659–666. [Google Scholar] [CrossRef]
- Ardhianto, P.; Yuniadi, Y. Biomarkers of Atrial Fibrillation: Which One Is a True Marker? Cardiol. Res. Pract. 2019, 2019, 8302326. [Google Scholar] [CrossRef]
- Hussein, A.A.; Bartz, T.M.; Gottdiener, J.S.; Sotoodehnia, N.; Heckbert, S.R.; Lloyd-Jones, D.; Kizer, J.R.; Christenson, R.; Wazni, O.; Defilippi, C. Serial measures of cardiac troponin T levels by a highly sensitive assay and incident atrial fibrillation in a prospective cohort of ambulatory older adults. Heart Rhythm 2015, 12, 879–885. [Google Scholar] [CrossRef]
- Sinner, M.F.; Stepas, K.A.; Moser, C.B.; Krijthe, B.P.; Aspelund, T.; Sotoodehnia, N.; Fontes, J.D.; Janssens, A.C.J.; Kronmal, R.A.; Magnani, J.W.; et al. B-type natriuretic peptide and C-reactive protein in the prediction of atrial fibrillation risk: The CHARGE-AF Consortium of community-based cohort studies. Europace 2014, 16, 1426–1433. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.P.; Yousuf, O.; Alonso, A.; Selvin, E.; Calkins, H.; McEvoy, J.W. High-Sensitivity Troponin as a Biomarker in Heart Rhythm Disease. Am. J. Cardiol. 2017, 119, 1407–1413. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.B.; Larson, M.G.; Yamamoto, J.F.; Sullivan, L.M.; Pencina, M.J.; Meigs, J.B.; Tofler, G.H.; Selhub, J.; Jacques, P.F.; Wolf, P.A.; et al. Relations of biomarkers of distinct pathophysiological pathways and atrial fibrillation incidence in the community. Circulation 2010, 121, 200–207. [Google Scholar] [CrossRef]
- Jabati, S.; Fareed, J.; Liles, J.; Otto, A.; Hoppensteadt, D.; Bontekoe, J.; Phan, T.; Walborn, A.; Syed, M. Biomarkers of Inflammation, Thrombogenesis, and Collagen Turnover in Patients with Atrial Fibrillation. Clin. Appl. Thromb. Hemost. 2018, 24, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Parise, H.; Levy, D.; D’Agostino, R.B., Sr.; Wolf, P.A.; Vasan, R.S.; Benjamin, E.J. Obesity and the risk of new-onset atrial fibrillation. JAMA 2004, 292, 2471–2477. [Google Scholar] [CrossRef] [PubMed]
- Huxley, R.R.; Misialek, J.R.; Agarwal, S.K.; Loehr, L.R.; Soliman, E.Z.; Chen, L.Y.; Alonso, A. Physical activity, obesity, weight change, and risk of atrial fibrillation: The Atherosclerosis Risk in Communities study. Circ. Arrhythmia Electrophysiol. 2014, 7, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Magnani, J.W.; Hylek, E.M.; Apovian, C.M. Obesity begets atrial fibrillation: A contemporary summary. Circulation 2013, 128, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.Á.; Toledo, E.; Arós, F.; Fiol, M.; Corella, D.; Salas-Salvadó, J.; Ros, E.; Covas, M.I.; Fernández-Crehuet, J.; Lapetra, J.; et al. Extravirgin olive oil consumption reduces risk of atrial fibrillation: The PREDIMED (Prevención con Dieta Mediterránea) trial. Circulation 2014, 130, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Urpi-Sarda, M.; Casas, R.; Chiva-Blanch, G.; Romero-Mamani, E.S.; Valderas-Martínez, P.; Arranz, S.; Andres-Lacueva, C.; Llorach, R.; Medina-Remón, A.; Lamuela-Raventos, R.M.; et al. Virgin olive oil and nuts as key foods of the Mediterranean diet effects on inflammatory biomarkers related to atherosclerosis. Pharmacol. Res. 2012, 65, 577–583. [Google Scholar] [CrossRef]
- Mitjavila, M.T.; Fandos, M.; Salas-Salvadó, J.; Covas, M.-I.; Borrego, S.; Estruch, R.; Lamuela-Raventós, R.; Corella, D.; Martínez-Gonzalez, M.; Sánchez, J.M.; et al. The Mediterranean diet improves the systemic lipid and DNA oxidative damage in metabolic syndrome individuals. A randomized, controlled, trial. Clin. Nutr. 2013, 32, 172–178. [Google Scholar] [CrossRef]
- Fitó, M.; Estruch, R.; Salas-Salvadó, J.; Martínez-Gonzalez, M.A.; Arós, F.; Vila, J.; Corella, D.; Díaz, O.; Sáez, G.; de la Torre, R.; et al. Effect of the Mediterranean diet on heart failure biomarkers: A randomized sample from the PREDIMED trial. Eur. J. Heart Fail. 2014, 16, 543–550. [Google Scholar] [CrossRef]
- Aizer, A.; Gaziano, J.M.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Albert, C.M. Relation of vigorous exercise to risk of atrial fibrillation. Am. J. Cardiol. 2009, 103, 1572–1577. [Google Scholar] [CrossRef] [PubMed]
- Mont, L.; Elosua, R.; Brugada, J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace 2009, 11, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.; Alam, A.B.; Li, L.; Norby, F.L.; Chen, L.Y.; Soliman, E.Z.; Alonso, A. Association of physical activity with the incidence of atrial fibrillation in persons > 65 years old: The Atherosclerosis Risk in Communities (ARIC) study. BMC Cardiovasc. Disord. 2022, 22, 196. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The Clinical Profile and Pathophysiology of Atrial Fibrillation. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Buil-Cosiales, P.; Corella, D.; Bulló, M.; Fitó, M.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; López-Miranda, J.; et al. Cohort Profile: Design and methods of the PREDIMED-Plus randomized trial. Int. J. Epidemiol. 2019, 48, 387–388o. [Google Scholar] [CrossRef]
- López, L.; Rossello, X.; Romaguera, D.; Alonso-Gómez, M.; Toledo, E.; Fortuny, E.; Noris, M.; Mas-Lladó, C.; Fiol, M.; Ramallal, R.; et al. The Palma Echo Platform: Rationale and Design of an Echocardiography Core Lab. Front. Cardiovasc. Med. 2022, 9, 909347. [Google Scholar] [CrossRef] [PubMed]
- Rossello, X.; Ramallal, R.; Romaguera, D.; Alonso-Gómez, M.; Alonso, A.; Tojal-Sierra, L.; Fernández-Palomeque, C.; Martínez-González, M.; Garrido-Uriarte, M.; López, L.; et al. Effect of an intensive lifestyle intervention on the structural and functional substrate for atrial fibrillation in people with metabolic syndrome. Eur. J. Prev. Cardiol. 2023, 31, 629–639. [Google Scholar] [CrossRef]
- Inker, L.A.; Eneanya, N.D.; Coresh, J.; Tighiouart, H.; Wang, D.; Sang, Y.; Crews, D.C.; Doria, A.; Estrella, M.M.; Froissart, M.; et al. New Creatinine- and Cystatin C–Based Equations to Estimate GFR without Race. N. Engl. J. Med. 2021, 385, 1737–1749. [Google Scholar] [CrossRef]
- Valeri, L.; VanderWeele, T.J. Mediation analysis allowing for exposure–mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef]
- Sayón-Orea, C.; Razquin, C.; Bulló, M.; Corella, D.; Fitó, M.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; Wärnberg, J.; Martínez, J.A.; et al. Effect of a Nutritional and Behavioral Intervention on Energy-Reduced Mediterranean Diet Adherence Among Patients with Metabolic Syndrome: Interim Analysis of the PREDIMED-Plus Randomized Clinical Trial. JAMA 2019, 322, 1486–1499. [Google Scholar] [CrossRef] [PubMed]
- Nicklas, J.M.; Sacks, F.M.; Smith, S.R.; LeBoff, M.S.; Rood, J.C.; Bray, G.A.; Ridker, P.M. Effect of dietary composition of weight loss diets on high-sensitivity c-reactive protein: The Randomized POUNDS LOST trial. Obesity 2013, 21, 681–689. [Google Scholar] [CrossRef] [PubMed]
- López-Domènech, S.; Martínez-Herrera, M.; Abad-Jiménez, Z.; Morillas, C.; Escribano-López, I.; Díaz-Morales, N.; Bañuls, C.; Víctor, V.M.; Rocha, M. Dietary weight loss intervention improves subclinical atherosclerosis and oxidative stress markers in leukocytes of obese humans. Int. J. Obes. 2019, 43, 2200–2209. [Google Scholar] [CrossRef] [PubMed]
- van Gemert, W.A.; May, A.M.; Schuit, A.J.; Oosterhof, B.Y.; Peeters, P.H.; Monninkhof, E.M. Effect of Weight Loss with or without Exercise on Inflammatory Markers and Adipokines in Postmenopausal Women: The SHAPE-2 Trial, A Randomized Controlled Trial. Cancer Epidemiol. Biomark. Prev. 2016, 25, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, M.; Heitkamp, M.; Braun, I.; Vogg, N.; Haller, B.; Langhof, H.; Koenig, W.; Halle, M. Changes of omentin-1 and chemerin during 4 weeks of lifestyle intervention and 1 year follow-up in children with obesity. Clin. Nutr. 2021, 40, 5648–5654. [Google Scholar] [CrossRef] [PubMed]
- Chainani-Wu, N.; Weidner, G.; Purnell, D.M.; Frenda, S.; Merritt-Worden, T.; Kemp, C.; Kersh, E.; Ornish, D. Relation of B-Type Natriuretic Peptide Levels to Body Mass Index After Comprehensive Lifestyle Changes. Am. J. Cardiol. 2010, 105, 1570–1576. [Google Scholar] [CrossRef]
- Fedele, D.; Bicchiega, V.; Collo, A.; Barutta, F.; Pistone, E.; Gruden, G.; Bruno, G. Short term variation in NTproBNP after lifestyle intervention in severe obesity. PLoS ONE 2017, 12, e0181212. [Google Scholar] [CrossRef] [PubMed]
- Chen-Tournoux, A.; Khan, A.M.; Baggish, A.L.; Castro, V.M.; Semigran, M.J.; McCabe, E.L.; Moukarbel, G.; Reingold, J.; Durrani, S.; Lewis, G.D.; et al. Effect of Weight Loss After Weight Loss Surgery on Plasma N-Terminal Pro-B-Type Natriuretic Peptide Levels. Am. J. Cardiol. 2010, 106, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Kistorp, C.; Bliddal, H.; Goetze, J.P.; Christensen, R.; Faber, J. Cardiac natriuretic peptides in plasma increase after dietary induced weight loss in obesity. BMC Obes. 2014, 1, 24. [Google Scholar] [CrossRef]
- Pennathur, S.; Jaiswal, M.; Vivekanandan-Giri, A.; White, E.A.; Ang, L.; Raffel, D.M.; Rubenfire, M.; Pop-Busui, R. Structured lifestyle intervention in patients with the metabolic syndrome mitigates oxidative stress but fails to improve measures of cardiovascular autonomic neuropathy. J. Diabetes Its Complicat. 2017, 31, 1437–1443. [Google Scholar] [CrossRef]
- Rector, R.S.; Turk, J.R.; Sun, G.Y.; Guilford, B.L.; Toedebusch, B.W.; McClanahan, M.W.; Thomas, T.R. Short-term lifestyle modification alters circulating biomarkers of endothelial health in sedentary, overweight adults. Appl. Physiol. Nutr. Metab. 2006, 31, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Van Der Linden, N.; Tieland, M.; Klinkenberg, L.; Verdijk, L.; de Groot, L.; van Loon, L.; van Dieijen-Visser, M.; Meex, S. The effect of a six-month resistance-type exercise training program on the course of high sensitive cardiac troponin T levels in (pre)frail elderly. Int. J. Cardiol. 2014, 175, 374–375. [Google Scholar] [CrossRef] [PubMed]
- van der Linden, N.; Klinkenberg, L.J.J.; Leenders, M.; Tieland, M.; Verdijk, L.B.; Niens, M.; van Suijlen, J.D.E.; de Groot, L.C.P.G.M.; Bekers, O.; van Loon, L.J.C.; et al. The effect of exercise training on the course of cardiac troponin T and I levels: Three independent training studies. Sci. Rep. 2015, 5, 18320. [Google Scholar] [CrossRef] [PubMed]
- Lyngbakken, M.N.; Omland, T.; Nordstrand, N.; Norseth, J.; Hjelmesæth, J.; Hofsø, D. Effect of weight loss on subclinical myocardial injury: A clinical trial comparing gastric bypass surgery and intensive lifestyle intervention. Eur. J. Prev. Cardiol. 2016, 23, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Löfsjögård, J.; Persson, H.; Díez, J.; López, B.; González, A.; Edner, M.; Mejhert, M.; Kahan, T. Atrial fibrillation and biomarkers of myocardial fibrosis in heart failure. Scand. Cardiovasc. J. 2014, 48, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Selvin, E.; Lutsey, P.L.; Hoogeveen, R.C.; O’Neal, W.T.; Soliman, E.Z.; Chen, L.Y.; Alonso, A. Association of N-terminal pro B-type natriuretic peptide (NT-proBNP) change with the risk of atrial fibrillation in the ARIC cohort. Am. Heart J. 2018, 204, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Selvin, E.; Hoogeveen, R.C.; Soliman, E.Z.; Chen, L.Y.; Norby, F.L.; Alonso, A. 6-year change in high sensitivity cardiac troponin T and the risk of atrial fibrillation in the Atherosclerosis Risk in Communities cohort. Clin. Cardiol. 2021, 44, 1594–1601. [Google Scholar] [CrossRef]
- Alonso, A.; Krijthe, B.P.; Aspelund, T.; Stepas, K.A.; Pencina, M.J.; Moser, C.B.; Sinner, M.F.; Sotoodehnia, N.; Fontes, J.D.; Janssens, A.C.J.W.; et al. Simple risk model predicts incidence of atrial fibrillation in a racially and geographically diverse population: The CHARGE-AF consortium. J. Am. Heart Assoc. 2013, 2, e000102. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 532) | ILI Arm (n = 266) | Control Arm (n = 266) | |
|---|---|---|---|
| Age, yr | 65.1 (4.9) | 64.7 (5.0) | 65.5 (4.8) |
| Female, % | 214 (40.2) | 99 (37.2) | 115 (43.2) |
| Origin, % | |||
| European | 518 (97.4) | 259 (97.4) | 259 (97.4) |
| Latin American | 14 (2.6) | 7 (2.6) | 7 (2.6) |
| Marital status, % | |||
| Single | 30 (5.7) | 13 (4.9) | 17 (6.4) |
| Married/cohabiting | 416 (78.3) | 203 (76.3) | 213 (80.4) |
| Divorced | 53 (10.0) | 34 (12.8) | 19 (7.2) |
| Widower | 32 (6.0) | 16 (6.0) | 16 (6.0) |
| Education, % | |||
| Less than high school | 259 (48.7) | 122 (45.9) | 137 (51.5) |
| High school | 167 (31.4) | 94 (35.3) | 73 (27.4) |
| At least some college | 106 (19.9) | 50 (18.8) | 56 (21.1) |
| BMI, kg/m2 | 32.2 (3.3) | 32.6 (3.4) | 31.9 (3.2) |
| SBP, mmHg | 141.1 (16.8) | 141.6 (17.8) | 140.7 (15.8) |
| DBP, mmHg | 79.3 (10.1) | 79.3 (10.3) | 79.3 (9.9) |
| Smoking, % | |||
| Never | 209 (39.3) | 105 (39.5) | 104 (39.1) |
| Former | 268 (50.4) | 132 (49.6) | 136 (51.1) |
| Current | 53 (10.0) | 29 (10.9) | 24 (9.0) |
| Alcohol consumption, g/day | 16.0 (20.3) | 16.1 (20.6) | 15.9 (20.1) |
| MedDiet adherence score | 7.7 (2.9) | 7.7 (2.9) | 7.6 (3.0) |
| MVPA, METs-min/week | 1887.5 (2219.4) | 1655.1 (2159.1) | 2119.9 (2258.3) |
| TPA, METs-min/week | 2540.7 (2258.5) | 2271.5 (2221.6) | 2809.8 (2267.0) |
| Diabetes, % | 149 (28.0) | 72 (27.1) | 77 (29.0) |
| Anti-hypertension medication, % | 408 (76.7) | 204 (76.7) | 204 (76.7) |
| Lipid-lowering medication, % | 270 (50.8) | 132 (49.6) | 138 (51.9) |
| Oral antidiabetic drugs, % | 116 (21.8) | 58 (21.8) | 58 (21.8) |
| Total cholesterol, mg/dL | 199.7 (36.0) | 199.8 (34.2) | 199.5 (37.8) |
| Triglycerides, mg/dL | 153.4 (70.9) | 153.7 (69.7) | 153.2 (72.1) |
| HDLc, mg/dL | 45.4 (10.7) | 45.6 (10.8) | 45.2 (10.6) |
| LDLc, mg/dL | 124.0 (31.3) | 123.8 (29.6) | 124.2 (32.9) |
| eGFR, mL/min/1.73 m2 | 90.6 (12.0) | 91.9 (10.9) | 89.3 (12.9) |
| PICP, mg/mL | 97.0 (42.0) | 95.5 (37.7) | 98.6 (46.0) |
| hsTnT, ng/L | 9.4 (4.8) | 9.4 (5.3) | 9.3 (4.2) |
| hsCRP, mg/dL | 0.4 (0.7) | 0.4 (0.5) | 0.4 (0.8) |
| 3-NT, nM | 762.0 (693.5) | 802.2 (683.0) | 721.4 (702.8) |
| NT-proBNP, pg/mL | 76.9 (127.5) | 72.3 (84.3) | 81.5 (159.7) |
| Control Arm | ILI Arm | Difference ILI—Control | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Y3 vs. Baseline | p-Value | Y5 vs. Baseline | p-Value | Y3 vs. Baseline | p-Value | Y5 vs. Baseline | p-Value | Y3 vs. Baseline | p-Value | Y5 vs. Baseline | p-Value | |
| PICP | −1% (−7%, 6%) | 0.83 | −1% (−7%, 5%) | 0.73 | −2% (−7%, 2%) | 0.29 | −3% (−8%, 1%) | 0.14 | −2% (−9%, 6%) | 0.69 | −2% (−9%, 6%) | 0.62 |
| hsTnT | 13% (9%, 16%) | <0.001 | 23% (19%, 27%) | <0.001 | 11% (7%, 15%) | <0.001 | 20% (16%, 24%) | <0.001 | −2% (−6%, 3%) | 0.47 | −3% (−7%, 2%) | 0.24 |
| hsCRP | −5% (−15%, 7%) | 0.38 | −9% (−18%, 3%) | 0.13 | −14% (−22%, −5%) | 0.004 | −21% (−29%, −13%) | <0.001 | −9% (−22%, 5%) | 0.20 | −14% (−26%, 0%) | 0.06 |
| 3−NT | 12% (3%, 23%) | 0.01 | 22% (11%, 33%) | <0.001 | 1% (−6%, 9%) | 0.72 | 3% (−5%, 11%) | 0.525 | −10% (−20%, 1%) | 0.08 | −16% (−25%, −5%) | 0.005 |
| NT-proBNP | 19% (9%, 30%) | <0.001 | 41% (29%, 55%) | <0.001 | 18% (7%, 30%) | <0.001 | 25% (13%, 38%) | <0.001 | −1% (−13%, 13%) | 0.87 | −12% (−23%, 1%) | 0.07 |
| Year 3 | Year 5 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Natural Direct Effect | Natural Indirect Effect | Total Effect | Proportion Mediated | p-Value for Indirect Effect | Natural Direct Effect | Natural Indirect Effect | Total Effect | Proportion Mediated | p-Value for Indirect Effect | |
| PICP | ||||||||||
| Physical activity | ||||||||||
| TPA | −3% (−10%, 4%) | 0% (−3%, 3%) | −3% (−10%, 4%) | 4% | 0.94 | −2% (−11%, 8%) | −1% (−5%, 3%) | −2% (−11%, 7%) | 36% | 0.66 |
| MVPA | −3% (−10%, 4%) | 0% (−3%, 3%) | −3% (−10%, 4%) | 3% | 0.96 | −2% (−11%, 8%) | −1% (−5%, 3%) | −2% (−11%, 7%) | 30% | 0.71 |
| MedDiet | −1% (−8%, 6%) | −2% (−4%, 1%) | −3% (−9%, 4%) | 58% | 0.19 | −2% (−11%, 7%) | 0% (−2%, 2%) | −2% (−11%, 7%) | −1% | 0.98 |
| Weight loss | 1% (−7%, 9%) | −4% (−7%, 0%) | −3% (−9%, 4%) | 122% | 0.08 | −1% (−11%, 9%) | −1% (−6%, 3%) | −2% (−11%, 7%) | 52% | 0.58 |
| hsTnT | ||||||||||
| Physical activity | ||||||||||
| TPA | −1% (−5%, 3%) | 0% (−2%, 1%) | −2% (−6%, 2%) | 30% | 0.54 | −2% (−8%, 3%) | 0% (−2%, 2%) | −2% (−7%, 3%) | −4% | 0.93 |
| MVPA | −1% (−5%, 4%) | −1% (−3%, 0%) | −2% (−6%, 2%) | 68% | 0.15 | −2% (−7%, 4%) | 0% (−3%, 2%) | −2% (−7%, 3%) | 20% | 0.67 |
| MedDiet | −1% (−5%, 4%) | −1% (−2%, 1%) | −2% (−6%, 3%) | 44% | 0.36 | −2% (−7%, 4%) | 0% (−2%, 1%) | −2% (−7%, 3%) | 20% | 0.51 |
| Weight loss | −1% (−6%, 3%) | 0% (−3%, 2%) | −2% (−6%, 2%) | 11% | 0.88 | −4% (−10%, 2%) | 2% (−1%, 5%) | −3% (−7%, 3%) | −67% | 0.22 |
| hsCRP | ||||||||||
| Physical activity | ||||||||||
| TPA | −11% (−25%, 5%) | 0% (−6%, 6%) | −11% (−24%, 3%) | 2% | 0.92 | −12% (−26%, 5%) | −2% (−9%, 5%) | −14% (−27%, 1%) | 13% | 0.59 |
| MVPA | −8% (−22%, 8%) | −4% (−9%, 2%) | −11% (−24%, 3%) | 30% | 0.22 | −14% (−28%, 2%) | 0% (−7%, 7%) | −14% (−27%, 1%) | −1% | 0.98 |
| MedDiet | −8% (−22%, 8%) | −4% (−9%, 1%) | −12% (−24%, 3%) | 32% | 0.15 | −14% (−27%, 1%) | 0% (−4%, 4%) | −14% (−27%, 1%) | −1% | 0.92 |
| Weight loss | 1% (−16%, 20%) | −12% (−19%, −3%) | −11% (−24%, 4%) | 105% | 0.006 | −2% (−18%, 18%) | −12% (−19%, −5%) | −14% (−26%, 2%) | 89% | 0.002 |
| 3−NT | ||||||||||
| Physical activity | ||||||||||
| TPA | −9% (−20%, 2%) | −1% (−6%, 4%) | −10% (−20%, 0%) | 9% | 0.68 | −15% (−27%, −2%) | −1% (−6%, 5%) | −16% (−26%, −4%) | 4% | 0.81 |
| MVPA | −11% (−21%, 1%) | 0% (−4%, 5%) | −10% (−20%, 0%) | −4% | 0.86 | −14% (−26%, −1%) | −2% (−7%, 4%) | −16% (−26%, −4%) | 10% | 0.54 |
| MedDiet | −10% (−20%, 2%) | −1% (−5%, 4%) | −10% (−20%, 0%) | 6% | 0.76 | −15% (−26%, −3%) | 0% (−4%, 3%) | −16% (−26%, −4%) | 3% | 0.78 |
| Weight loss | −11% (−22%, 1%) | 1% (−5%, 8%) | −10% (−20%, 0%) | −10% | 0.75 | −17% (−29%, −4%) | 2% (−5%, 9%) | −16% (−26%, −4%) | −10% | 0.61 |
| NT-proBNP | ||||||||||
| Physical activity | ||||||||||
| TPA | −4% (−16%, 11%) | 1% (−4%, 7%) | −3% (−15%, 11%) | −44% | 0.67 | −10% (−23%, 6%) | 0% (−7%, 7%) | −10% (−22%, 4%) | 4% | 0.90 |
| MVPA | −4% (−16%, 11%) | 1% (−4%, 6%) | −3% (−15%, 11%) | −44% | 0.67 | −10% (−23%, 6%) | 0% (−7%, 7%) | −10% (−22%, 4%) | 2% | 0.94 |
| MedDiet | −3% (−16%, 11%) | 1% (−4%, 6%) | −2% (−15%, 12%) | −43% | 0.68 | −11% (−23%, 4%) | 1% (−3%, 5%) | −10% (−23%, 4%) | −5% | 0.79 |
| Weight loss | −9% (−22%, 6%) | 7% (−1%, 16%) | −3% (−15%, 11%) | −246% | 0.08 | −11% (−25%, 5%) | 1% (−6%, 9%) | −10% (−22%, 4%) | −12% | 0.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, L.; Alonso, A.; Romaguera, D.; Alonso-Gómez, A.M.; Razquin, C.; Tojal-Sierra, L.; Fiol, M.; Martínez-González, M.A.; Subramanya, V.; Salas-Salvadó, J.; et al. Effect of an Intensive Lifestyle Intervention on Circulating Biomarkers of Atrial Fibrillation-Related Pathways among Adults with Metabolic Syndrome: Results from a Randomized Trial. J. Clin. Med. 2024, 13, 2132. https://doi.org/10.3390/jcm13072132
Li L, Alonso A, Romaguera D, Alonso-Gómez AM, Razquin C, Tojal-Sierra L, Fiol M, Martínez-González MA, Subramanya V, Salas-Salvadó J, et al. Effect of an Intensive Lifestyle Intervention on Circulating Biomarkers of Atrial Fibrillation-Related Pathways among Adults with Metabolic Syndrome: Results from a Randomized Trial. Journal of Clinical Medicine. 2024; 13(7):2132. https://doi.org/10.3390/jcm13072132
Chicago/Turabian StyleLi, Linzi, Alvaro Alonso, Dora Romaguera, Angel M. Alonso-Gómez, Cristina Razquin, Lucas Tojal-Sierra, Miquel Fiol, Miguel Angel Martínez-González, Vinita Subramanya, Jordi Salas-Salvadó, and et al. 2024. "Effect of an Intensive Lifestyle Intervention on Circulating Biomarkers of Atrial Fibrillation-Related Pathways among Adults with Metabolic Syndrome: Results from a Randomized Trial" Journal of Clinical Medicine 13, no. 7: 2132. https://doi.org/10.3390/jcm13072132