
The Expression and Amplification of HER2 Has a Significant Impact on the Prognosis of Endometrial Carcinoma in Korean Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Construction of a Tissue Microarray Using Representative Tissue Samples
2.3. Immunohistochemistry
2.4. Dual-Color SISH
2.5. Statistical Analysis
3. Results
3.1. Clinical Data
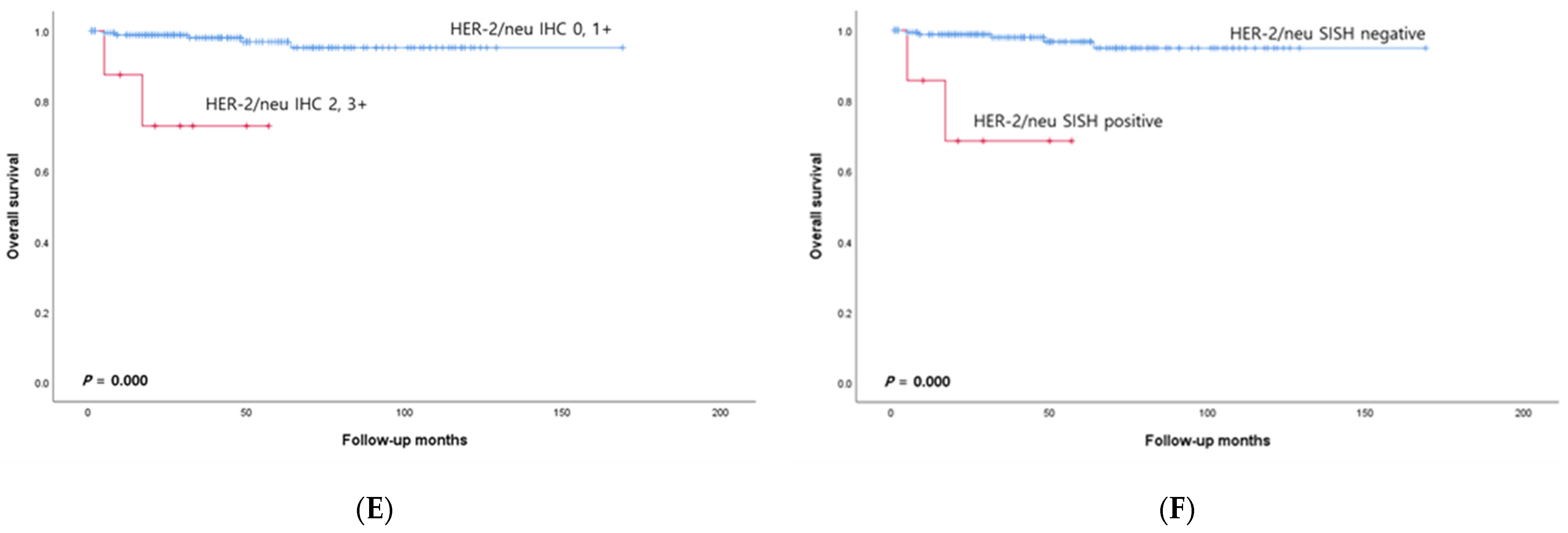
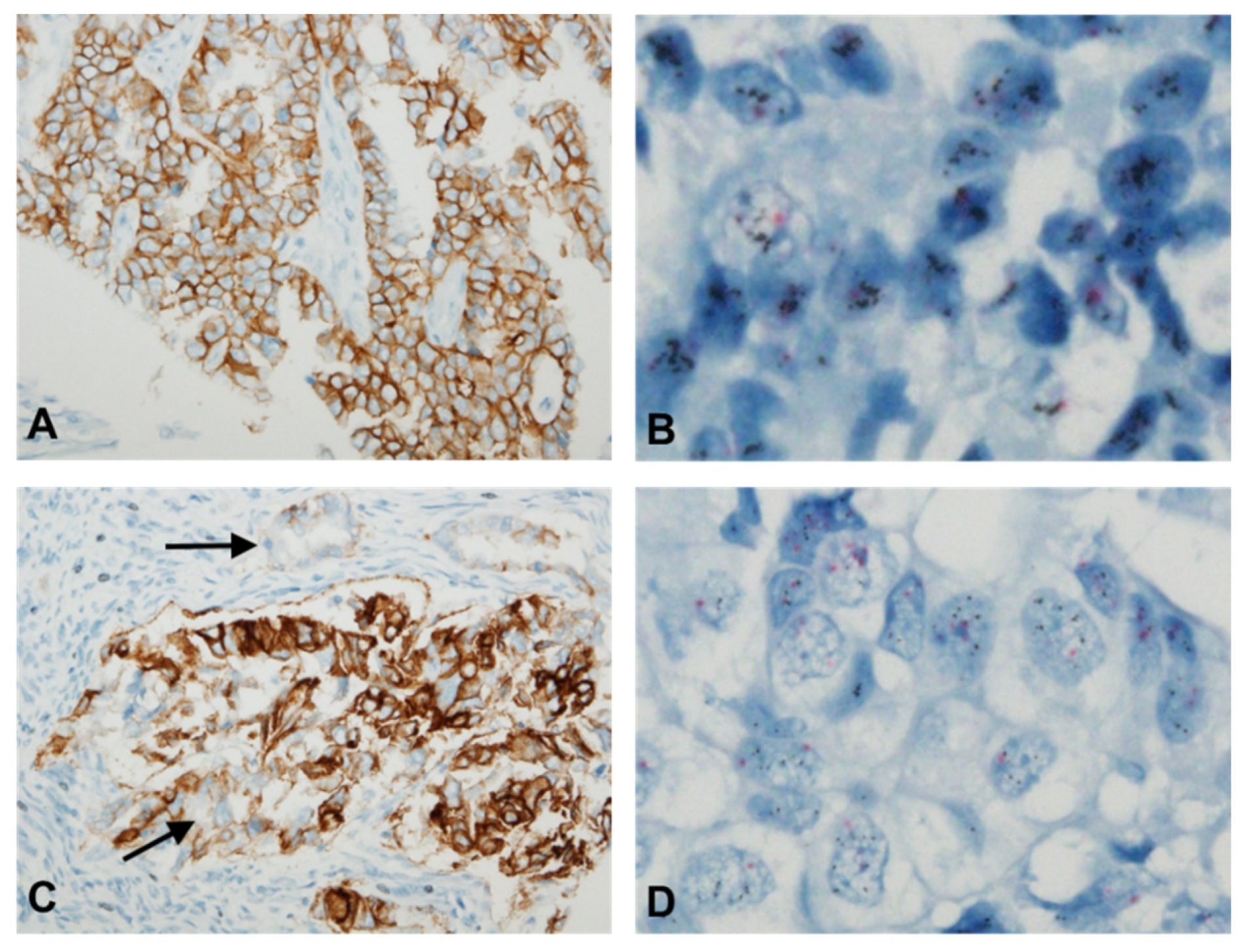
3.2. HER2 Protein Expression Analysis via IHC
3.3. HER2 Gene Amplification Analysis via SISH
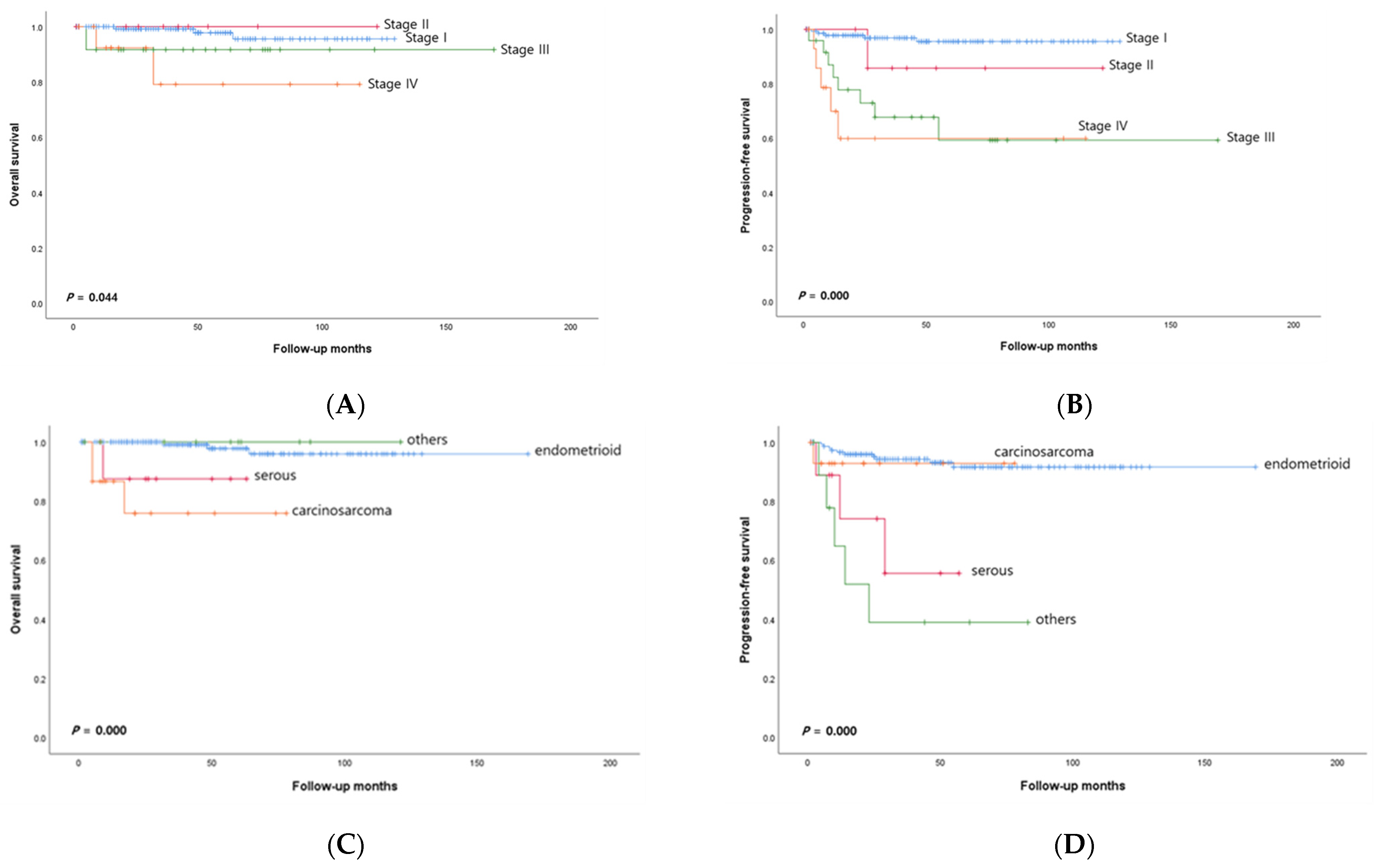
3.4. Relationships between Surgical-Pathologic Variables and Survival Outcome
3.5. Associations between HER2 Protein Expression and Gene Amplification
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jung, K.; Won, Y.; Kang, M.J.; Kong, H.; Im, J.; Seo, H.G. Prediction of cancer incidence and mortality in Korea, 2022. Cancer Res. Treat. 2022, 54, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.; Won, Y.; Hong, S.; Kong, H.; Lee, E.S. Prediction of cancer incidence and mortality in Korea, 2020. Cancer Res. Treat. 2020, 52, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Brüggmann, D.; Ouassou, K.; Klingelhöfer, D.; Bohlmann, M.K.; Jaque, J.; Groneberg, D.A. Endometrial cancer: Mapping the global landscape of research. J. Transl. Med. 2020, 18, 386. [Google Scholar] [CrossRef]
- Slomovitz, B.M.; Broaddus, R.R.; Burke, T.W.; Sneige, N.; Soliman, P.T.; Wu, W.; Sun, C.C.; Munsell, M.F.; Gershenson, D.M.; Lu, K.H. Her-2/neu overexpression and amplification in uterine papillary serous carcinoma. J. Clin. Oncol. 2004, 22, 3126–3132. [Google Scholar] [CrossRef]
- Rottmann, D.; Snir, O.L.; Wu, X.; Wong, S.; Hui, P.; Santin, A.D.; Buza, N. HER2 testing of gynecologic carcinosarcomas: Tumor stratification for potential targeted therapy. Mod. Pathol. 2020, 33, 118–127. [Google Scholar] [CrossRef]
- Johnson, A.L.; Medina, H.N.; Schlumbrecht, M.P.; Reis, I.; Kobetz, E.N.; Pinheiro, P.S. The role of histology on endometrial cancer survival disparities in diverse florida. PLoS ONE 2020, 15, e0236402. [Google Scholar] [CrossRef] [PubMed]
- Santin, A.D.; Bellone, S.; Van Stedum, S.; Bushen, W.; Palmieri, M.; Siegel, E.R.; De Las Casas Luis, E.; Roman, J.J.; Burnett, A.; Pecorelli, S. Amplification of c-erbB2 oncogene: A major prognostic indicator in uterine serous papillary carcinoma. Cancer 2005, 104, 1391–1397. [Google Scholar] [CrossRef]
- Akiyama, T.; Sudo, C.; Ogawara, H.; Toyoshima, K.; Yamamoto, T. The product of the human c-erbB-2 gene: A 185-kilodalton glycoprotein with tyrosine kinase activity. Science 1986, 232, 1644–1646. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, N.; Iqbal, N. Human epidermal growth factor receptor 2 (HER2) in cancers: Overexpression and therapeutic implications. Mol. Biol. Int. 2014, 2014, 852748. [Google Scholar] [CrossRef]
- Morrison, C.; Zanagnolo, V.; Ramirez, N.; Cohn, D.E.; Kelbick, N.; Copeland, L.; Maxwell, G.L.; Fowler, J.M. HER-2 is an independent prognostic factor in endometrial cancer: Association with outcome in a large cohort of surgically staged patients. J. Clin. Oncol. 2006, 24, 2376–2385. [Google Scholar] [CrossRef]
- Felix, A.S.; Scott McMeekin, D.; Mutch, D.; Walker, J.L.; Creasman, W.T.; Cohn, D.E.; Ali, S.; Moore, R.G.; Downs, L.S.; Ioffe, O.B.; et al. Associations between etiologic factors and mortality after endometrial cancer diagnosis: The NRG oncology/gynecologic oncology group 210 trial. Gynecol. Oncol. 2015, 139, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Kuwata, T.; Setsuda, A.; Tokunaga, M.; Kaito, A.; Sugita, S.; Tonouchi, A.; Kinoshita, T.; Nagino, M. Molecular and pathological analyses of gastric stump cancer by next-generation sequencing and immunohistochemistry. Sci. Rep. 2021, 11, 4165–4171. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Shim, S.; Jung, H.Y.; Dong, M.; Kim, S.; Lee, S.J. The gene copy number of c-MET has a significant impact on progression-free survival in korean patients with ovarian carcinoma. Hum. Pathol. 2017, 64, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Yutani, S.; Shirahama, T.; Muroya, D.; Matsueda, S.; Yamaguchi, R.; Morita, M.; Shichijo, S.; Yamada, A.; Sasada, T.; Itoh, K. Feasibility study of personalized peptide vaccination for hepatocellular carcinoma patients refractory to locoregional therapies. Cancer Sci. 2017, 108, 1732–1738. [Google Scholar] [CrossRef]
- Hammock, L.; Lewis, M.; Phillips, C.; Cohen, C. Strong HER-2/neu protein overexpression by immunohistochemistry often does not predict oncogene amplification by fluorescence in situ hybridization. Hum. Pathol. 2003, 34, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Jang, N.; Kwon, H.J.; Park, M.H.; Kang, S.H.; Bae, Y.K. Prognostic value of tumor-infiltrating lymphocyte density assessed using a standardized method based on molecular subtypes and adjuvant chemotherapy in invasive breast cancer. Ann. Surg. Oncol. 2018, 25, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Kong, T.W.; Chang, S.J.; Paek, J.; Lee, Y.; Chun, M.; Ryu, H.S. Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer: A validation study of the gynecologic oncology group criteria. J. Gynecol. Oncol. 2015, 26, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Vloeberghs, V.; Woestenborghs, H.; Debiec-Rychter, M.; Verbist, L.; Moerman, P.; Vergote, I. ERBB-2 gene overexpression and amplification in uterine sarcomas. Gynecol. Oncol. 2004, 95, 583–587. [Google Scholar] [CrossRef]
- Zeng, X.; Zhao, D.; Zhou, W.; Wu, S.; Liang, Z.; Liu, T. Evaluation of HER2 gene expression status in breast cancer by fluorescence in-situ hybridization. Zhonghua Bing Li Xue Za Zhi 2005, 34, 701–705. [Google Scholar]
- Grazziotin, L.R.; Dada, B.R.; de la Rosa Jaimes, C.; Cheung, W.Y.; Marshall, D.A. Chromogenic and silver in situ hybridization for identification of HER 2 overexpression in breast cancer patients: A systematic review and meta-analysis. Appl. Immunohistochem. Mol. Morphol. 2020, 28, 411–421. [Google Scholar] [CrossRef]
- Fader, A.N.; Roque, D.M.; Siegel, E.; Buza, N.; Hui, P.; Abdelghany, O.; Chambers, S.K.; Secord, A.A.; Havrilesky, L.; O’Malley, D.M.; et al. Randomized phase II trial of carboplatin-paclitaxel versus carboplatin-paclitaxel-trastuzumab in uterine serous carcinomas that overexpress human epidermal growth factor receptor 2/neu. J. Clin. Oncol. 2018, 36, 2044–2051. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, T.M.; Cantrell, L.A.; Stoler, M.H.; Mills, A.M. HER2 overespression and amplification in uterine carcinosarcomas with serous morphology. Am. J. Surg. Pathol. 2022, 46, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Vermij, L.; Horeweg, N.; Leon-Castillo, A.; Rutten, T.A.; Mileshkin, L.R.; Mackay, H.J.; Leary, A.; Powell, M.E.; Singh, N.; Crosbie, E.J.; et al. Her2 status in high-risk endometrial cancers (PORTEC-3): Relationship with histotype, molecular classification, and clinical outcomes. Cancers 2020, 13, 44. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, E.; Wu, R.C.; Guan, B.; Wu, G.; Zhang, J.; Wang, Y.; Song, L.; Yuan, X.; Wei, L.; Roden, R.B.; et al. Identification of molecular pathway aberrations in uterine serous carcinoma by genome-wide analyses. J. Natl. Cancer Inst. 2012, 104, 1503–1513. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [PubMed]
- Ross, D.S.; Devereaux, K.A.; Jin, C.; Lin, D.Y.; Zhang, Y.; Marra, A.; Makker, V.; Weigelt, B.; Elleson, L.H.; Chui, M.H. Histopathologic features and molecular genetic landscape of HER2-amplified endometrial carcinomas. Mod. Pathol. 2022, 35, 962–971. [Google Scholar] [CrossRef]
- Iwai, K.; Fukuda, K.; Hachisuga, T.; Mori, M.; Uchiyama, M.; Iwasaka, T.; Sugimori, H. Prognostic significance of progesterone receptor immunohistochemistry for lymph node metastases in endometrial carcinoma. Gynecol. Oncol. 1999, 72, 351–359. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Number of Patients (%) (n = 191) |
|---|---|
| Age, n (%) | |
| <50 | 67 (35.1) |
| ≥50 | 124 (64.9) |
| Histologic subtype, n (%) | |
| Endometrioid | 157 (82.2) |
| Serous | 9 (4.7) |
| Clear cell | 1 (0.5) |
| Squamous | 1 (0.5) |
| Mixed | 8 (4.2) |
| Carcinosarcoma | 15 (7.9) |
| Stage of disease, n (%) | |
| I | 142 (74.3) |
| II | 10 (5.2) |
| III | 24 (12.6) |
| IV | 15 (7.9) |
| Histological grade, n (%) | |
| 1 | 84 (44.0) |
| 2 | 66 (34.6) |
| 3 | 26 (13.6) |
| unknown | 15 (7.8) |
| Myometrial invasion, n (%) | |
| <1/2 | 133 (69.6) |
| ≥1/2 | 58 (30.4) |
| Adnexal involvement, n (%) | |
| No | 171 (89.5) |
| Yes | 20 (10.5) |
| Lymph-vascular space invasion, n (%) | |
| No | 145 (75.9) |
| Yes | 46 (24.1) |
| Lymph node involvement | |
| No | 166 (86.9) |
| Yes | 25 (13.1) |
| Recurrence of disease, n (%) | 19 (9.9) |
| Died of disease, n (%) | 7 (3.7) |
| Histotype | HER2 IHC | p | HER2 SISH | p | |||
|---|---|---|---|---|---|---|---|
| Negative 0 or 1+ | Positive | Negative | Positive | ||||
| 2+ | 3+ | ||||||
| Endometrioid | 156 (99.4) | 1 (0.6) | 0 | <0.0001 | 151 (100.0) | 0 | <0.0001 |
| Serous | 6 (66.6) | 2 (22.2) | 1 (11.1) | 6 (66.7) | 3 (33.3) | ||
| Clear cell | 1 (100.0) | 0 | 0 | 1 (100.0) | 0 | ||
| Squamous | 1 (100.0) | 0 | 0 | 1 (100.0) | 0 | ||
| Mixed | 8 (100.0) | 0 | 0 | 8 (100.0) | 0 | ||
| Carcinosarcoma | 11 (73.3) | 2 (13.3) | 2 (13.3) | 10 (71.4) | 4 (28.6) | ||
| Total | 183 (95.9%) | 5 (2.6%) | 3 (1.6%) | 177 (96.2%) | 7 (3.8%) | ||
| Histologic Type | Age | Stage | Carcinoma Type | Sarcoma Type | HER2 IHC | HER2 SISH |
|---|---|---|---|---|---|---|
| Carcinosarcoma | 64 | IVB | Serous | Rhabdomyosarcoma | 3+ | Positive |
| Carcinosarcoma | 57 | IVA | Serous | Homologous | 3+ | Positive |
| Carcinosarcoma | 83 | IA | Serous | Homologous | 2+ | Positive |
| Carcinosarcoma | 65 | IB | Serous | Homologous | 2+ | Positive |
| Serous | 59 | IA | - | - | 3+ | Positive |
| Serous | 62 | IA | - | - | 2+ | Positive |
| Serous | 63 | IIIC2 | - | - | 2+ | Positive |
| Endometrioid | 69 | IB | - | - | 2+ | Negative |
| Factors | N | Overall Survival | Progression-Free Survival | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| Age | |||||||
| <50 | 67 | 1.00 | 1.00 | ||||
| ≥50 | 124 | 2.27 | 0.20–25.41 | 0.505 | 2.10 | 0.66–6.72 | 0.210 |
| Histology | |||||||
| Endometrioid | 157 | 1.00 | 1.00 | ||||
| Nonendometrioid | 34 | 0.98 | 0.07–13.06 | 0.988 | 1.64 | 0.46–5.84 | 0.440 |
| Grade | |||||||
| Endometrioid G1, G2 | 145 | 1.00 | 1.00 | ||||
| Endometrioid G3, serous, clear cell, carcinosarcoma | 46 | 3.44 | 0.24–48.39 | 0.359 | 3.02 | 0.78–11.69 | 0.110 |
| Stage of disease | |||||||
| I or II | 152 | 1.00 | 1.00 | ||||
| III or IV | 39 | 1.00 | 0.09–10.82 | 1.000 | 3.34 | 0.89–12.47 | 0.043 |
| Myometrial invasion, | |||||||
| <1/2 | 133 | 1.00 | 1.00 | ||||
| ≥1/2 | 58 | 3.23 | 0.39–26.86 | 0.278 | 0.57 | 0.19–1.73 | 0.323 |
| Adnexal involvement | |||||||
| No | 171 | 1.00 | 1.00 | ||||
| Yes | 20 | 4.49 | 0.46–43.64 | 0.195 | 1.28 | 0.43–3.83 | 0.663 |
| Lymph-vascular space invasion | |||||||
| No | 145 | 1.00 | 1.00 | ||||
| Yes | 46 | 0.89 | 0.09–8.25 | 0.921 | 4.41 | 1.34–14.55 | 0.015 |
| HER2 IHC/HER2 SISH | |||||||
| Negative/negative | 183 | 1.00 | |||||
| Positive/negative | 1 | 0.00 | 0.00 | 0.994 | 0.00 | 0.00 | 0.996 |
| Positive/positive | 7 | 7.86 | 1.85–72.28 | 0.049 | 0.00 | 0.00 | 0.985 |
| Factors | N | Overall Survival | Progression-Free Survival | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | ||
| Age | |||||||
| <50 | 67 | 1.00 | 1.00 | ||||
| ≥50 | 124 | 2.42 | 0.27–22.00 | 0.434 | 2.08 | 0.688–6.290 | 0.194 |
| Stage of disease | |||||||
| I or II | 152 | 1.00 | 1.00 | ||||
| III or IV | 39 | 3.44 | 0.05–23.36 | 0.206 | 5.00 | 1.58–15.79 | 0.006 |
| Lymph-vascular space invasion | |||||||
| No | 145 | 1.00 | 1.00 | ||||
| Yes | 46 | 2.24 | 0.32–15.84 | 0.419 | 3.94 | 1.24–12.55 | 0.020 |
| HER2 IHC/HER2 SISH | |||||||
| Negative/negative | 183 | 1.00 | |||||
| Positive/negative | 1 | 0.00 | 0.00 | 0.993 | 0.00 | 0.00 | 0.997 |
| Positive/positive | 7 | 12.99 | 2.08–81.03 | 0.006 | 0.01 | 0.00 | 0.982 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.Y.; Yang, E.J.; Jang, E.B.; Lee, A.J.; So, K.A.; Shim, S.-H.; Kim, T.J.; Lee, S.J. The Expression and Amplification of HER2 Has a Significant Impact on the Prognosis of Endometrial Carcinoma in Korean Patients. J. Clin. Med. 2024, 13, 2158. https://doi.org/10.3390/jcm13082158
Kim WY, Yang EJ, Jang EB, Lee AJ, So KA, Shim S-H, Kim TJ, Lee SJ. The Expression and Amplification of HER2 Has a Significant Impact on the Prognosis of Endometrial Carcinoma in Korean Patients. Journal of Clinical Medicine. 2024; 13(8):2158. https://doi.org/10.3390/jcm13082158
Chicago/Turabian StyleKim, Wook Youn, Eun Jung Yang, Eun Bi Jang, A Jin Lee, Kyeong A So, Seung-Hyuk Shim, Tae Jin Kim, and Sun Joo Lee. 2024. "The Expression and Amplification of HER2 Has a Significant Impact on the Prognosis of Endometrial Carcinoma in Korean Patients" Journal of Clinical Medicine 13, no. 8: 2158. https://doi.org/10.3390/jcm13082158