
Pediatric Odontogenic Sinusitis: A Systematic Review

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Information Sources and Search Strategy
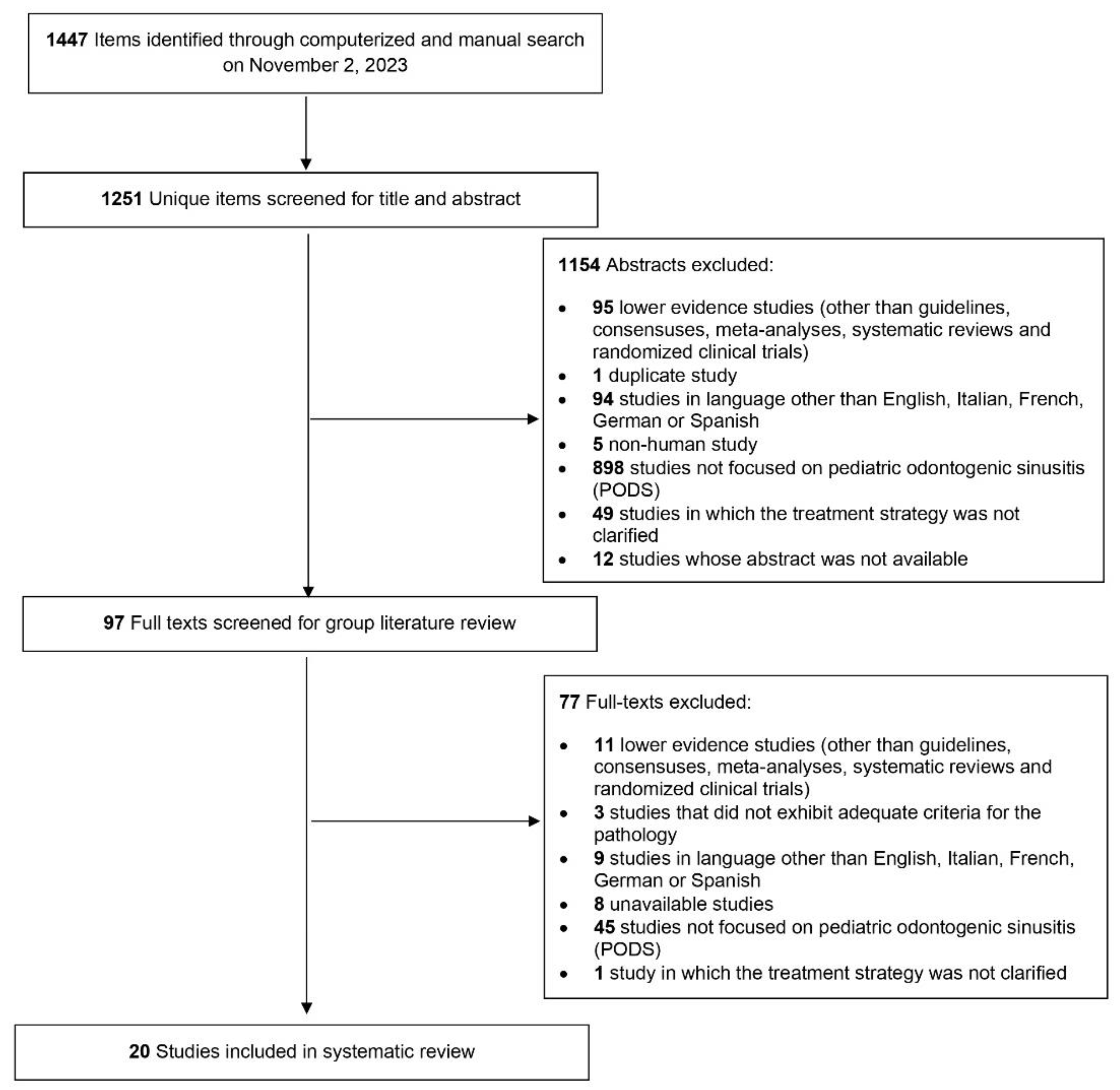
2.3. Selection Process
2.4. PICOS Criteria
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Presentation and Synthesis Method
3. Results
4. Discussion
4.1. Epidemiology
4.2. Etiology
4.3. Complications
4.4. Diagnostic Modalities
4.5. Treatments
4.6. Outcomes
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Craig, J.R.; Poetker, D.M.; Aksoy, U.; Allevi, F.; Biglioli, F.; Cha, B.Y.; Chiapasco, M.; Lechien, J.R.; Safadi, A.; Simuntis, R.; et al. Diagnosing Odontogenic Sinusitis: An International Multidisciplinary Consensus Statement. Int. Forum Allergy Rhinol. 2021, 11, 1235–1248. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.R.; Tataryn, R.W.; Cha, B.Y.; Bhargava, P.; Pokorny, A.; Gray, S.T.; Mattos, J.L.; Poetker, D.M. Diagnosing Odontogenic Sinusitis of Endodontic Origin: A Multidisciplinary Literature Review. Am. J. Otolaryngol. 2021, 42, 102925. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.M.; Pipolo, C.; Borloni, R.; Felisati, G. ENT and Dentist Cooperation in the Management of Odontogenic Sinusitis. A Review. Acta Otorhinolaryngol. Ital. 2021, 41, S116–S123. [Google Scholar] [CrossRef] [PubMed]
- Vitali, F.C.; Santos, P.S.; Massignan, C.; Maia, L.C.; Cardoso, M.; da Silveira Teixeira, C. Global Prevalence of Maxillary Sinusitis of Odontogenic Origin and Associated Factors: A Systematic Review and Meta-Analysis. J. Endod. 2023, 49, 369–381.e11. [Google Scholar] [CrossRef]
- Akhlaghi, F.; Esmaeelinejad, M.; Safai, P. Etiologies and Treatments of Odontogenic Maxillary Sinusitis: A Systematic Review. Iran. Red Crescent Med. J. 2015, 17, e25536. [Google Scholar] [CrossRef] [PubMed]
- Allevi, F.; Fadda, G.L.; Rosso, C.; Martino, F.; Pipolo, C.; Cavallo, G.; Felisati, G.; Saibene, A.M. Diagnostic Criteria for Odontogenic Sinusitis: A Systematic Review. Am. J. Rhinol. Allergy 2021, 35, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Molteni, M.; Bulfamante, A.M.; Pipolo, C.; Lozza, P.; Allevi, F.; Pisani, A.; Chiapasco, M.; Portaleone, S.M.; Scotti, A.; Maccari, A.; et al. Odontogenic Sinusitis and Sinonasal Complications of Dental Treatments: A Retrospective Case Series of 480 Patients with Critical Assessment of the Current Classification. Acta Otorhinolaryngol. Ital. 2020, 40, 282–289. [Google Scholar] [CrossRef]
- Saibene, A.M.; Collurà, F.; Pipolo, C.; Bulfamante, A.M.; Lozza, P.; Maccari, A.; Arnone, F.; Ghelma, F.; Allevi, F.; Biglioli, F.; et al. Odontogenic Rhinosinusitis and Sinonasal Complications of Dental Disease or Treatment: Prospective Validation of a Classification and Treatment Protocol. Eur. Arch. Otorhinolaryngol. 2019, 276, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowska, M.A.; Szczygielski, K.; Chloupek, A.; Szczupak, P.; Jurkiewicz, D. Clinical Characteristics of Odontogenic Sinusitis with Periapical Lesions. Am. J. Otolaryngol. 2022, 43, 103338. [Google Scholar] [CrossRef]
- Turfe, Z.; Ahmad, A.; Peterson, E.I.; Craig, J.R. Odontogenic Sinusitis Is a Common Cause of Unilateral Sinus Disease with Maxillary Sinus Opacification. Int. Forum Allergy Rhinol. 2019, 9, 1515–1520. [Google Scholar] [CrossRef]
- Saibene, A.M.; Pipolo, G.C.; Lozza, P.; Maccari, A.; Portaleone, S.M.; Scotti, A.; Borloni, R.; Messina, F.; Di Pasquale, D.; Felisati, G. Redefining Boundaries in Odontogenic Sinusitis: A Retrospective Evaluation of Extramaxillary Involvement in 315 Patients. Int. Forum Allergy Rhinol. 2014, 4, 1020–1023. [Google Scholar] [CrossRef]
- Goyal, V.K.; Ahmad, A.; Turfe, Z.; Peterson, E.I.; Craig, J.R. Predicting Odontogenic Sinusitis in Unilateral Sinus Disease: A Prospective, Multivariate Analysis. Am. J. Rhinol. Allergy 2021, 35, 164–171. [Google Scholar] [CrossRef]
- Craig, J.R.; Tataryn, R.W.; Aghaloo, T.L.; Pokorny, A.T.; Gray, S.T.; Mattos, J.L.; Poetker, D.M. Management of Odontogenic Sinusitis: Multidisciplinary Consensus Statement. Int. Forum Allergy Rhinol. 2020, 10, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Felisati, G.; Chiapasco, M.; Lozza, P.; Saibene, A.M.; Pipolo, C.; Zaniboni, M.; Biglioli, F.; Borloni, R. Sinonasal Complications Resulting from Dental Treatment: Outcome-Oriented Proposal of Classification and Surgical Protocol. Am. J. Rhinol. Allergy 2013, 27, e101–e106. [Google Scholar] [CrossRef]
- Andric, M.; Saranovic, V.; Drazic, R.; Brkovic, B.; Todorovic, L. Functional Endoscopic Sinus Surgery as an Adjunctive Treatment for Closure of Oroantral Fistulae: A Retrospective Analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 510–516. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Huang, C.-C.; Chang, P.-H.; Chen, C.-W.; Wu, C.-C.; Fu, C.-H.; Lee, T.-J. The Characteristics and New Treatment Paradigm of Dental Implant-Related Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2013, 27, 237–244. [Google Scholar] [CrossRef]
- Craig, J.R. Odontogenic Sinusitis: A State-of-the-Art Review. World J. Otorhinolaryngol. Head Neck Surg. 2022, 8, 8–15. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Wald, E.R.; Applegate, K.E.; Bordley, C.; Darrow, D.H.; Glode, M.P.; Marcy, S.M.; Nelson, C.E.; Rosenfeld, R.M.; Shaikh, N.; Smith, M.J.; et al. Clinical Practice Guideline for the Diagnosis and Management of Acute Bacterial Sinusitis in Children Aged 1 to 18 Years. Pediatrics 2013, 132, e262–e280. [Google Scholar] [CrossRef] [PubMed]
- Mulvey, C.L.; Kiell, E.P.; Rizzi, M.D.; Buzi, A. The Microbiology of Complicated Acute Sinusitis among Pediatric Patients: A Case Series. Otolaryngol. Head Neck Surg. 2019, 160, 712–719. [Google Scholar] [CrossRef]
- Saibene, A.M.; Vassena, C.; Pipolo, C.; Trimboli, M.; De Vecchi, E.; Felisati, G.; Drago, L. Odontogenic and Rhinogenic Chronic Sinusitis: A Modern Microbiological Comparison. Int. Forum Allergy Rhinol. 2016, 6, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.; Hon, K.L.; Chu, W.C. Acute Bacterial Sinusitis in Children: An Updated Review. Drugs Context 2020, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Akhaddar, A.; Elasri, F.; Elouennass, M.; Mahi, M.; Elomari, N.; Elmostarchid, B.; Oubaaz, A.; Boucetta, M. Orbital Abscess Associated with Sinusitis from Odontogenic Origin. Intern. Med. 2010, 49, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 14 March 2024).
- Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 14 March 2024).
- Cozzi, A.T.; Ottavi, A.; Lozza, P.; Maccari, A.; Borloni, R.; Nitro, L.; Felisati, E.G.; Alliata, A.; Martino, B.; Cacioppo, G.; et al. Intraoperative Neuromonitoring Does Not Reduce the Risk of Temporary and Definitive Recurrent Laryngeal Nerve Damage during Thyroid Surgery: A Systematic Review and Meta-Analysis of Endoscopic Findings from 73,325 Nerves at Risk. J. Pers Med. 2023, 13, 1429. [Google Scholar] [CrossRef] [PubMed]
- Battulga, B.; Benjamin, M.R.; Chen, H.; Bat-Enkh, E. The Impact of Social Support and Pregnancy on Subjective Well-Being: A Systematic Review. Front. Psychol. 2021, 12, 710858. [Google Scholar] [CrossRef] [PubMed]
- OCEBM Levels of Evidence. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 14 March 2024).
- Arunkumar, K.V. Orbital Infection Threatening Blindness Due to Carious Primary Molars: An Interesting Case Report. J. Maxillofac. Oral Surg. 2016, 15, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Blagojević, M.; Stefanović, B.; Piščević, P.; Radosavljević, M. Phlegmon de L’orbite D’origine Dentaire. Ophthalmologica 2010, 157, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, D.S.; Powell, O. Orbital Cellulitis and Sinusitis Caused by Group B Beta Streptococcus in a 3-Year-Old Child. J. Natl. Med. Assoc. 1985, 77, 147–148. [Google Scholar]
- Brook, I. Microbiology of Acute Sinusitis of Odontogenic Origin Presenting with Periorbital Cellulitis in Children. Ann. Otol. Rhinol. Laryngol. 2007, 116, 386–388. [Google Scholar] [CrossRef]
- Brook, I. Microbiology of Intracranial Abscesses Associated with Sinusitis of Odontogenic Origin. Ann. Otol. Rhinol. Laryngol. 2006, 115, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Brook, I.; Friedman, E.M. Intracranial Complications of Sinusitis in Children. A Sequela of Periapical Abscess. Ann. Otol. Rhinol. Laryngol. 1982, 91, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Bullock, J.D.; Fleishman, J.A. Orbital Cellulitis Following Dental Extraction. Trans. Am. Ophthalmol. Soc. 1984, 82, 111–133. [Google Scholar] [PubMed]
- Derin, S.; Sahan, M.; Hazer, D.B.; Sahan, L. Subdural Empyema and Unilateral Pansinusitis due to a Tooth Infection. BMJ Case Rep. 2015, 2015, bcr2014207666. [Google Scholar] [CrossRef]
- de Assis-Costa, M.D.M.; Santos, G.S.; Maciel, J.; Sonoda, C.K.; de Melo, W.M. Odontogenic Infection Causing Orbital Cellulitis in a Pediatric Patient. J. Craniofac. Surg. 2013, 24, e526–e529. [Google Scholar] [CrossRef]
- Dhingra, S.; Gulati, A. Teeth in Rare Locations with Rare Complications: An Overview. Indian J. Otolaryngol. Head Neck Surg. 2015, 67, 438–443. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Goh, Y.H. Ectopic Eruption of Maxillary Molar Tooth—An Unusual Cause of Recurrent Sinusitis. Singap. Med. J. 2001, 42, 80–81. [Google Scholar]
- Janakarajah, N.; Sukumaran, K. Orbital Cellulitis of Dental Origin: Case Report and Review of the Literature. Br. J. Oral Maxillofac. Surg. 1985, 23, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Kallel, S.; Ghorbel, A.M. Facial abscess revealing maxillary sinusitis of dental origin. Pan Afr. Med. J. 2019, 32, 115. [Google Scholar] [CrossRef]
- de Araujo, C.M. Odontogenic Maxillary Sinusitis In Children. Rev. Bras. Otorrinolaringol. 1945, 13, 197–208. [Google Scholar]
- Nisa, L.; Giger, R. Images in Clinical Medicine. Ectopic Tooth in the Maxillary Sinus. N. Engl. J. Med. 2011, 365, 1232. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, S.P.; Padwa, B.L.; Robson, C.D.; Rahbar, R. Dentigerous Cyst Associated with a Displaced Tooth in the Maxillary Sinus: An Unusual Cause of Recurrent Sinusitis in an Adolescent. Pediatr. Radiol. 2009, 39, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Ruth, M.; Widiastuti, M.G.; Dwiraharjo, B. Removal of an Ectopic Canine Tooth in the Maxillary Sinus Using Bone Lid Technique. J. Dentomaxillofacial Sci. 2022, 7, 128–131. [Google Scholar] [CrossRef]
- Wysluch, A.; Maurer, P.; Ast, J.; Kunkel, M. Orbital Complications due to an Acute Odontogenic Focus in a Child. A Case Report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, e39–e42. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.-W.; Kwon, H.-J.; Woo, I.-H.; Yang, B.-E.; Lee, S.-Y.; Lee, H.-R.; Kim, K.-N. An Unusual Cause of Acute Maxillary Sinusitis in a 9-Year-Old Child: Odontogenic Origin of Infected Dentigerous Cyst with Supernumerary Teeth. Pediatr. Infect. Vaccine 2015, 22, 201. [Google Scholar] [CrossRef]
- Ramadan, H.H.; Chaiban, R.; Makary, C. Pediatric Rhinosinusitis. Pediatr. Clin. N. Am. 2022, 69, 275–286. [Google Scholar] [CrossRef]
- Ramadan, H.H. Pediatric Chronic Rhinosinusitis. Eur. Arch. Otorhinolaryngol. 2024, 281, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Magit, A. Pediatric Rhinosinusitis. Otolaryngol. Clin. N. Am. 2014, 47, 733–746. [Google Scholar] [CrossRef]
- Snidvongs, K.; Sangubol, M.; Poachanukoon, O. Pediatric Versus Adult Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2020, 20, 29. [Google Scholar] [CrossRef]
- Morcom, S.; Phillips, N.; Pastuszek, A.; Timperley, D. Sinusitis. Aust. Fam. Physician 2016, 45, 374–377. [Google Scholar]
- Khanna, G.; Sato, Y.; Smith, R.J.H.; Bauman, N.M.; Nerad, J. Causes of Facial Swelling in Pediatric Patients: Correlation of Clinical and Radiologic Findings. Radiographics 2006, 26, 157–171. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.C.; Lee, S.J. Clinical Features and Treatments of Odontogenic Sinusitis. Yonsei Med. J. 2010, 51, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.R.; Cheema, A.J.; Dunn, R.T.; Vemuri, S.; Peterson, E.L. Extrasinus Complications from Odontogenic Sinusitis: A Systematic Review. Otolaryngol. Head Neck Surg. 2022, 166, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R. Pediatric Odontogenic and Paranasal Sinus Infections. Neuroimaging Clin. N. Am. 2023, 33, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Thawley, S.E.; Gado, M.; Fuller, T.R. Computerized Tomography in the Evaluation of Head and Neck Lesions. Laryngoscope 1978, 88, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Chandy, Z.; Ference, E.; Lee, J.T. Clinical Guidelines on Chronic Rhinosinusitis in Children. Curr. Allergy Asthma Rep. 2019, 19, 14. [Google Scholar] [CrossRef] [PubMed]
- Goodman, T.R.; Mustafa, A.; Rowe, E. Pediatric CT Radiation Exposure: Where We Were, and Where We Are Now. Pediatr. Radiol. 2019, 49, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Saibene, A.M.; Allevi, F.; Calvo-Henriquez, C.; Maniaci, A.; Mayo-Yáñez, M.; Paderno, A.; Vaira, L.A.; Felisati, G.; Craig, J.R. Reliability of Large Language Models in Managing Odontogenic Sinusitis Clinical Scenarios: A Preliminary Multidisciplinary Evaluation. Eur. Arch. Otorhinolaryngol. 2024, 281, 1835–1841. [Google Scholar] [CrossRef] [PubMed]
- Simuntis, R.; Kubilius, R.; Tušas, P.; Leketas, M.; Vaitkus, J.; Vaitkus, S. Chronic Odontogenic Rhinosinusitis: Optimization of Surgical Treatment Indications. Am. J. Rhinol. Allergy 2020, 34, 767–774. [Google Scholar] [CrossRef]
- Craig, J.R.; Saibene, A.M.; Felisati, G. Chronic Odontogenic Rhinosinusitis: Optimization of Surgical Treatment Indications. Am. J. Rhinol. Allergy 2021, 35, 142–143. [Google Scholar] [CrossRef]
- Albu, S.; Baciut, M. Failures in Endoscopic Surgery of the Maxillary Sinus. Otolaryngol. Head Neck Surg. 2010, 142, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Aukštakalnis, R.; Simonavičiūtė, R.; Simuntis, R. Treatment Options for Odontogenic Maxillary Sinusitis: A Review. Stomatologija 2018, 20, 22–26. [Google Scholar] [PubMed]
- Preda, M.A.; Muşat, O.; Sarafoleanu, C.C.; Popescu, I.S.; Muşat, A.; Pîrvulescu, R.; Barac, R.; Tătaru, C.P.; Muşat, G.C. Oculo-Orbital Complications of Odontogenic Sinusitis. Rom. J. Ophthalmol. 2023, 67, 175–179. [Google Scholar] [PubMed]


{kind=link}
| Database | Search Date | Query | Items Retrieved (n) |
|---|---|---|---|
| Medline | 2 November 2023 | (child*[Title/Abstract] OR pediatr*[Title/Abstract] OR infan*[Title/Abstract] OR newborn*[Title/Abstract] OR new-born*[Title/Abstract] OR perinat*[Title/Abstract] OR neonat*[Title/Abstract] OR baby[Title/Abstract] OR babies[Title/Abstract] OR toddler*[Title/Abstract] OR minors*[Title/Abstract] OR boy[Title/Abstract] OR boys[Title/Abstract] OR girl[Title/Abstract] OR girls[Title/Abstract] OR kid[Title/Abstract] OR kids[Title/Abstract] OR preschool*[Title/Abstract] OR schoolchild*[Title/Abstract] OR “school child*”[Title/Abstract] OR adolescen*[Title/Abstract] OR juvenil*[Title/Abstract] OR youth*[Title/Abstract] OR teen*[Title/Abstract] OR underage*[Title/Abstract] OR “under age”[Title/Abstract] OR pubescen*[Title/Abstract] OR puberty[Title/Abstract] OR paediatric*[Title/Abstract] OR peadiatric*[Title/Abstract]) AND (sinusitis[Title/Abstract] OR rhinosinusitis[Title/Abstract]) AND (odontogenic[Title/Abstract] OR implant[Title/Abstract] OR “dental implant”[Title/Abstract] OR tooth[Title/Abstract] OR “sinus elevation”[Title/Abstract] OR “sinus augmentation”[Title/Abstract] OR “sinus lift”[Title/Abstract] OR “dental implantation”[Title/Abstract] OR fistula[Title/Abstract] OR extraction[Title/Abstract] OR endodontic[Title/Abstract]) | 67 |
| Embase | 2 November 2023 | (child*:ti,ab,kw OR pediatr*:ti,ab,kw OR infan*:ti,ab,kw OR newborn*:ti,ab,kw OR ‘new born*’:ti,ab,kw OR perinat*:ti,ab,kw OR neonat*:ti,ab,kw OR baby:ti,ab,kw OR babies:ti,ab,kw OR toddler*:ti,ab,kw OR minors*:ti,ab,kw OR boy:ti,ab,kw OR boys:ti,ab,kw OR girl:ti,ab,kw OR girls:ti,ab,kw OR kid:ti,ab,kw OR kids:ti,ab,kw OR preschool*:ti,ab,kw OR schoolchild*:ti,ab,kw OR ‘school child*’:ti,ab,kw OR adolescen*:ti,ab,kw OR juvenil*:ti,ab,kw OR youth*:ti,ab,kw OR teen*:ti,ab,kw OR underage*:ti,ab,kw OR ‘under age’:ti,ab,kw OR pubescen*:ti,ab,kw OR puberty:ti,ab,kw OR paediatric*:ti,ab,kw OR peadiatric*:ti,ab,kw) AND (sinusitis:ti,ab,kw OR rhinosinusitis:ti,ab,kw) AND (odontogenic:ti,ab,kw OR implant:ti,ab,kw OR ‘dental implant’:ti,ab,kw OR tooth:ti,ab,kw OR ‘sinus elevation’:ti,ab,kw OR ‘sinus augmentation’:ti,ab,kw OR ‘sinus lift’:ti,ab,kw OR ‘dental implantation’:ti,ab,kw OR fistula:ti,ab,kw OR extraction:ti,ab,kw OR endodontic:ti,ab,kw) | 92 |
| Cochrane library | 2 November 2023 | ((child* OR pediatr* OR infan* OR newborn* OR new-born* OR perinat* OR neonat* OR baby OR babies OR toddler* OR minors* OR boy OR boys OR girl OR girls OR kid OR kids OR preschool* OR schoolchild* OR “school child*” OR adolescen* OR juvenil* OR youth* OR teen* OR underage* OR “under age” OR pubescen* OR puberty OR paediatric* OR peadiatric*) AND (sinusitis OR rhinosinusitis) AND (odontogenic OR implant OR “dental implant” OR tooth OR “sinus elevation” OR “sinus augmentation” OR “sinus lift” OR “dental implantation” OR fistula OR extraction OR endodontic)):ti,ab,kw | 256 |
| Web Of Science | 2 November 2023 | TS = ((child* OR pediatr* OR infan* OR newborn* OR new-born* OR perinat* OR neonat* OR baby OR babies OR toddler* OR minors* OR boy OR boys OR girl OR girls OR kid OR kids OR preschool* OR schoolchild* OR “school child*” OR adolescen* OR juvenil* OR youth* OR teen* OR underage* OR “under age” OR pubescen* OR puberty OR paediatric* OR peadiatric*) AND (sinusitis OR rhinosinusitis) AND (odontogenic OR implant OR “dental implant” OR tooth OR “sinus elevation” OR “sinus augmentation” OR “sinus lift” OR “dental implantation” OR fistula OR extraction OR endodontic)) | 94 |
| Clinicaltrials.gov | 2 November 2023 | (child* OR pediatr* OR infan* OR newborn* OR new-born* OR perinat* OR neonat* OR baby OR babies OR toddler* OR minors* OR boy OR boys OR girl OR girls OR kid OR kids OR preschool* OR schoolchild* OR “school child*” OR adolescen* OR juvenil* OR youth* OR teen* OR underage* OR “under age” OR pubescen* OR puberty OR paediatric* OR peadiatric*) AND (sinusitis OR rhinosinusitis) AND (odontogenic OR implant OR “dental implant” OR tooth OR “sinus elevation” OR “sinus augmentation” OR “sinus lift” OR “dental implantation” OR fistula OR extraction OR endodontic) | 41 |
| Scopus | 2 November 2023 | TITLE-ABS-KEY ((child* OR pediatr* OR infan* OR newborn* OR new-born* OR perinat* OR neonat* OR baby OR babies OR toddler* OR minors* OR boy OR boys OR girl OR girls OR kid OR kids OR preschool* OR schoolchild* OR “school child*” OR adolescen* OR juvenil* OR youth* OR teen* OR underage* OR “under age” OR pubescen* OR puberty OR paediatric* OR peadiatric*) AND (sinusitis OR rhinosinusitis) AND (odontogenic OR implant OR “dental implant” OR tooth OR “sinus elevation” OR “sinus augmentation” OR “sinus lift” OR “dental implantation” OR fistula OR extraction OR endodontic)) | 897 |
| Total non-unique hits | 1447 | ||
| Reference | Study Type | OCEBM Rating | Quality Rating |
|---|---|---|---|
| Akhaddar et al., 2010 [23] | CR | 4 | F |
| Arunkmar, 2015 [30] | CR | 4 | G |
| Blagojeviḉ et al., 1969 [31] | CS | 4 | G |
| Blumenthal et al., 1985 [32] | CR | 4 | G |
| Brook et al., 1982 [33] | CS | 4 | G |
| Brook, 2006 [34] | CS | 4 | P |
| Brook, 2007 [35] | CS | 4 | P |
| Bullock et al., 1984 [36] | CR | 4 | G |
| Derin et al., 2015 [37] | CR | 4 | G |
| de Assis Costa et al., 2013 [38] | CR | 4 | G |
| Dhingra et al., 2015 [39] | CS | 4 | G |
| Goh, 2001 [40] | CR | 4 | G |
| Janakarajah et al., 1985 [41] | CR | 4 | G |
| Kallel et al., 2019 [42] | CR | 4 | F |
| Machado de Araujo, 1945 [43] | CR | 4 | G |
| Nisa et al., 2011 [44] | CR | 4 | G |
| Prabhu et al., 2009 [45] | CR | 4 | G |
| Ruth et al., 2022 [46] | CR | 4 | G |
| Wysluch et al., 2008 [47] | CR | 4 | G |
| Yun et al., 2015 [48] | CR | 4 | G |
| Reference | Treated Patients (n) | Female:Male Ratio (n:n) | Patients’ Mean Age at Diagnosis (Years) | Diagnosis | Aetiology |
|---|---|---|---|---|---|
| Akhaddar et al., 2010 [23] | 1 | 1:0 | 11 | Ophthalmologic visit, CT, MR | Endodontic treatment |
| Arunkmar, 2015 [30] | 1 | 0:1 | 10 | Ophthalmologic visit, nasal endoscopy, CT | Carious tooth |
| Blagojeviḉ et al., 1969 [31] | 2 | 1:1 | 11.5 | Ophthalmologic visit (2) | Tooth extraction (2) |
| Blumenthal et al., 1985 [32] | 1 | 1:0 | 3 | XR, CT, blood sample | Carious tooth |
| Brook et al., 1982 [33] | 2 | 2:0 | 6.5 | XR (2) | Tooth rupture; endodontic treatment |
| Brook, 2006 [34] | 2 | 2:0 | 6.5 | N/R | Periodontal abscess (2) |
| Brook, 2007 [35] | 18 | 12:6 | 14 | XR(18); CT (18) | Pulpitis (9); periodonotal abscess (7); endodontic treatment (2) |
| Bullock et al., 1984 [36] | 1 | 1:0 | 12 | CT, ophthalmologic visit | Tooth extraction |
| Derin et al., 2015 [37] | 1 | 1:0 | 16 | CT | Ectopic tooth |
| de Assis Costa et al., 2013 [38] | 1 | 1:0 | 6 | CT | Carious tooth |
| Dhingra et al., 2015 [39] | 2 | 1:1 | 12 | CT (2); TB test (1) | Ectopic tooth (2) |
| Goh, 2001 [40] | 1 | 1:0 | 17 | Nasal endoscopy, XR | Ectopic tooth |
| Janakarajah et al., 1985 [41] | 1 | 1:0 | 14 | OPT, XR, ophthalmologic visit, blood sample | N/R |
| Kallel et al., 2019 [42] | 1 | 1:0 | 17 | CT | Ectopic tooth |
| Machado de Araujo, 1945 [43] | 1 | 1:0 | 5 | Blood sample, XR | Tooth extraction |
| Nisa et al., 2011 [44] | 1 | 1:0 | 15 | CT | Ectopic tooth |
| Prabhu et al., 2009 [45] | 1 | 1:0 | 14 | OPT, CT | Ectopic tooth |
| Ruth et al., 2022 [46] | 1 | 0:1 | 9 | OPT, CT | Ectopic tooth |
| Wysluch et al., 2008 [47] | 1 | 0:1 | 12 | Ophthalmologic visit, blood sample, CT | Endodontic treatment |
| Yun et al., 2015 [48] | 1 | 1:0 | 9 | OPT, CT | Supernumerary teeth |
| Reference | Treated Patients (n) | Prior Therapy | Primary Treatment | Other Concurrent Treatment | Outcome | Complications | Other Further Treatments | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|
| Akhaddar et al., 2010 [23] | 1 | Antibiotics (Amoxicillin) | Surgery: N/R | Antibiotics (Amoxicilli, Metronidazole, Gentamicin) | S | Orbital abscess | OCS, HOT | N/R |
| Arunkmar, 2015 [30] | 1 | Antibiotics (Vancomycin, Meropenem, Metronidazole) | Combined Surgery: Caldwell-Luc, tooth extraction, inferomedial-orbital incision | Antibiotics—same scheme as prior therapy | S | Orbital cellulitis | None | 3 |
| Blagojeviḉ et al., 1969 [31] | 2 | None | Surgery: Caldwell-Luc (1); anterior orbitotomy through Lynch incision (1); OAC closure (2) | Antibiotics | S | Orbital cellulitis (1); orbital phlegmon (1) | None | N/R |
| Blumenthal et al., 1985 [32] | 1 | Antibiotics (Ampicillin, Cloramphenicol, Penicillin G) | Surgery: intranasal endoscopic | None | F | Orbital cellulitis, seizure | Tooth extraction | 12 |
| Brook et al., 1982 [33] | 2 | Antibiotics (2) (Ampicillin, Erythromicin, Chloramphenicol; Methicillin) | Surgery: combined surgery with Caldwell-Luc and craniotomy (1); craniotomy (1) | None | S | Cerebritis and periorbital cellulitis (1); subdural empyema (1) | Antibiotics (2) (Ampicillin + Oxacillin) | 12 |
| Brook, 2006 [34] | 2 | None | Surgery (2): N/R | Antibiotics | N/R | Subdural empyema (2) | N/R | N/R |
| Brook, 2007 [35] | 18 | None | Surgery: intranasal endoscopic (16); Caldwell-Luc (2) | N/R | N/R | Orbital cellulitis (14) | N/R | N/R |
| Bullock et al., 1984 [36] | 1 | Antibiotics (Cephalotin) | Surgery: anterior orbitotomy through Lynch incision | Antibiotics (Gentamicin, Clindamycin, Methicillin, Chloramphenicol) | F | Periorbital cellulitis, cerebral abscess, death | None | N/R |
| Derin et al., 2015 [37] | 1 | Antibiotics | Combined surgery: external inferior lid approach and tooth extraction | Antibiotics (Ampicillin, Metronidazole) | S | Orbital cellulitis | None | N/R |
| de Assis Costa et al., 2013 [38] | 1 | None | Surgery: Caldwell-Luc | Antibiotics (Clindamycin, Ceftriaxone) | F | Pre-maxillary abscess, subdural empyema | Empyema’s drainage through craniotomy, antibiotics (Metronidazole) | 2 |
| Dhingra et al., 2015 [39] | 2 | None | Surgery: combined surgery with intranasal endoscopic surgery and tooth extraction (1); Caldwell-Luc (1) | None | S | None; fistulous tract | None | N/R; 24 |
| Goh, 2001 [40] | 1 | Antibiotics | Surgery: Caldwell-Luc | None | S | None | None | N/R |
| Janakarajah et al., 1985 [41] | 1 | None | Surgery: tooth extraction | None | S | Orbital cellulitis | None | 2 |
| Kallel et al., 2019 [42] | 1 | None | Combined surgery: external approach to the NV and intranasal endoscopic | None | S | Fistulous tract | None | N/R |
| Machado de Araujo, 1945 [43] | 1 | None | Surgery: tooth extraction | Nasal lavage, intranasal ephedrine | F | N/R | Adenoidectomy | N/R |
| Nisa et al., 2011 [44] | 1 | None | Surgery: intranasal endoscopic | None | S | None | None | 8 |
| Prabhu et al., 2009 [45] | 1 | Antibiotics, systemic antihistamines, INCS | Surgery: N/R | None | S | N/R | None | 0,5 |
| Ruth et al., 2022 [46] | 1 | None | Surgery: Caldwell-Luc | None | S | None | None | 1 |
| Wysluch et al., 2008 [47] | 1 | Endodontic treatment | Combined surgery: latero-orbital and Lynch incision, tooth extraction, and insertion of drainage tube from the nostril | Antibiotics (Amoxicillin, Metronidazole) | S | Orbital cellulitis | None | N/R |
| Yun et al., 2015 [48] | 1 | Antibiotics, systemic antihistamines, INCS | Surgery: Caldwell-Luc | None | S | none | None | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosso, C.; Urbanelli, A.; Spoldi, C.; Felisati, G.; Pecorari, G.; Pipolo, C.; Nava, N.; Saibene, A.M. Pediatric Odontogenic Sinusitis: A Systematic Review. J. Clin. Med. 2024, 13, 2215. https://doi.org/10.3390/jcm13082215
Rosso C, Urbanelli A, Spoldi C, Felisati G, Pecorari G, Pipolo C, Nava N, Saibene AM. Pediatric Odontogenic Sinusitis: A Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2215. https://doi.org/10.3390/jcm13082215
Chicago/Turabian StyleRosso, Cecilia, Anastasia Urbanelli, Chiara Spoldi, Giovanni Felisati, Giancarlo Pecorari, Carlotta Pipolo, Nicolò Nava, and Alberto Maria Saibene. 2024. "Pediatric Odontogenic Sinusitis: A Systematic Review" Journal of Clinical Medicine 13, no. 8: 2215. https://doi.org/10.3390/jcm13082215
APA StyleRosso, C., Urbanelli, A., Spoldi, C., Felisati, G., Pecorari, G., Pipolo, C., Nava, N., & Saibene, A. M. (2024). Pediatric Odontogenic Sinusitis: A Systematic Review. Journal of Clinical Medicine, 13(8), 2215. https://doi.org/10.3390/jcm13082215