
Psychodiabetology: The Challenge of the Future?


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
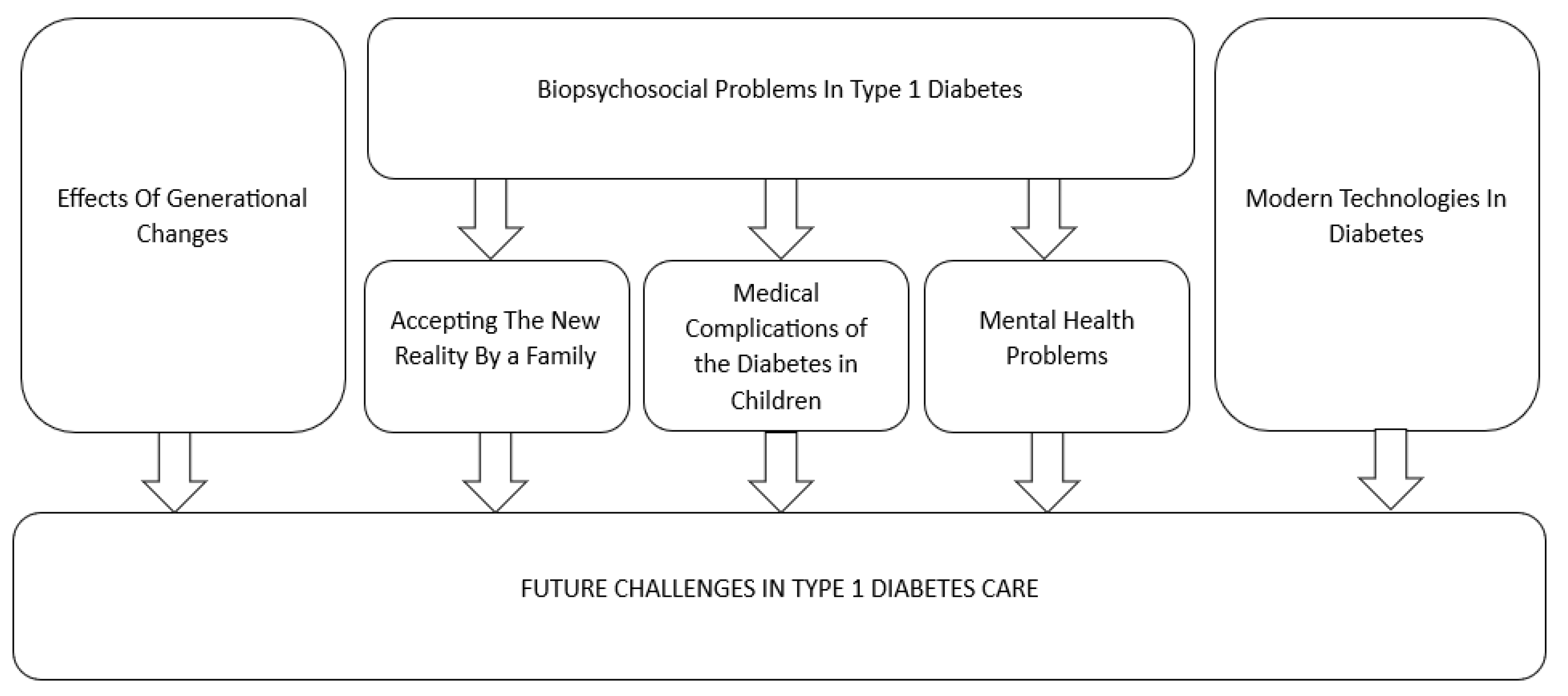
2. Biopsychosocial Problems in Diabetes
2.1. Accepting the New Reality by a Family
2.2. Medical Complications of Diabetes in Children
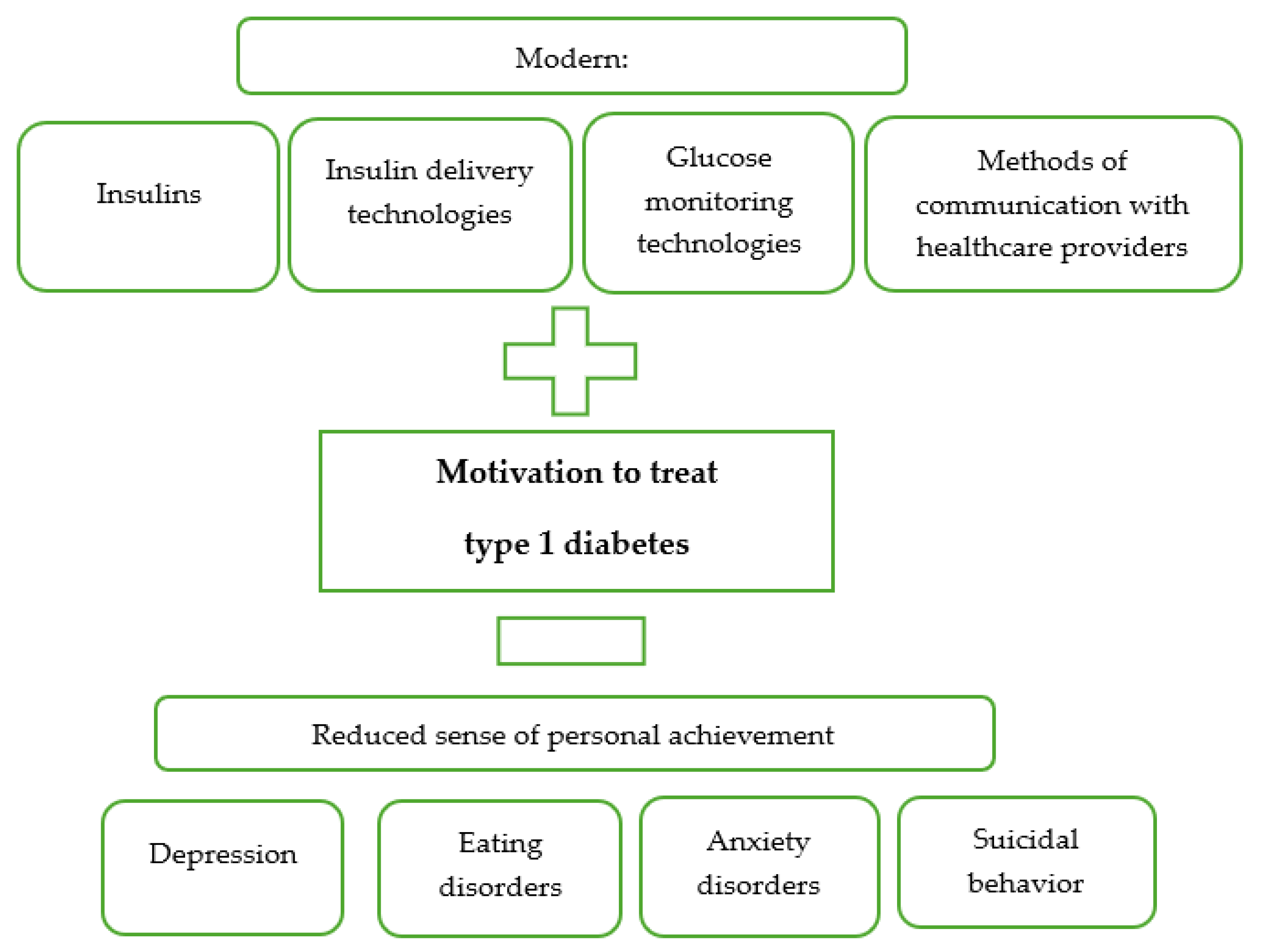
2.3. Mental Health Problems
3. Effects of Generational Changes
4. Modern Technologies in Diabetes
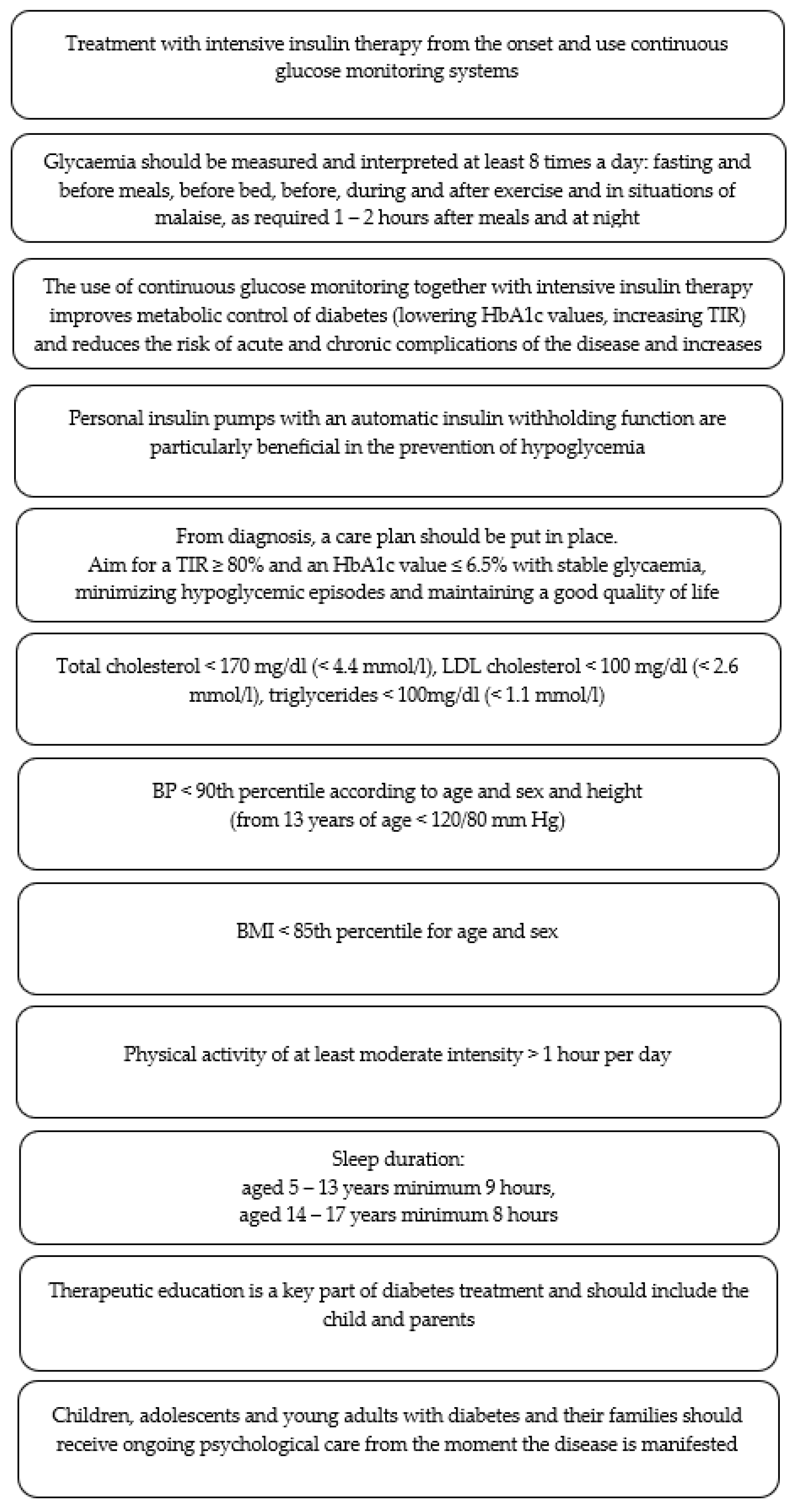
5. Future Challenges
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Foundation. IDF Diabetes Atlas, 10th ed.; International Diabetes Foundation: Brussels, Belgium, 2021. [Google Scholar]
- Jarosz-Chobot, P.; Otto-Buczkowska, E. Epidemiologia cukrzycy typu 1. Stand. Med. Pediatr. 2010, 7, 392–398. [Google Scholar]
- Instytutu Ochrony Zdrowia. Cukrzyca. In Gdzie Jesteśmy? Dokąd Zmierzamy? Raport Instytutu Ochrony Zdrowia; Instytutu Ochrony Zdrowia: Warsaw, Poland, 2018. [Google Scholar]
- EURODIAB ACE Study Group. Variation and trends in incidence of childhood diabetes in Europe. Lancet 2000, 335, 873–876. [Google Scholar]
- Jarosz-Chobot, P.; Polanska, J.; Szadkowska, A.; Kretowski, A.; Bandurska-Stankiewicz, E.; Ciechanowska, M.; Deja, G.; Mysliwiec, M.; Peczynska, J.; Rutkowska, J.; et al. Rapid increase in the incidence of type 1 diabetes in Polish children from 1989 to 2004, and predictions for 2010 to 2025. Diabetologia 2011, 54, 508–515. [Google Scholar] [CrossRef]
- Peczyńska, J.; Peczyńska, J.; Jemiołkowska, M. Epidemiologia cukrzycy typu 1 w makroregionie podlaskim w latach 2005–2012. Pediatr. Endocrinol. Diabetes Metab. 2016, 24, 14–19. [Google Scholar]
- Szybiński, Z. Wieloośrodkowe badania nad zapadalnością na cukrzycę typu 1 w grupie wiekowej 0–14 lat w Polsce w latach 1998–1999. Pol. Arch. Intern. Med. 2001, 106, 759. [Google Scholar]
- Brzuszek, M. Trend Sekularny Występowania Cukrzycy Typu 1 w Województwie Podkarpackim w Latach 2009–2019. Ph.D. Thesis, Uniwersytet Rzeszowski, Rzeszów, Poland, 2023. [Google Scholar]
- Otto-Buczkowska, E. Metabolic memory—The role in diabetes. Forum Med. Rodz. 2014, 8, 51–55. [Google Scholar]
- Deja, G.; Chobot, A.; Polańska, J.; Jarosz-Chobot, P. Epidemiologia cukrzycy typu 1. In Diabetologia Wieku Rozwojowego; Myśliwiec, M., Jarosz-Chobot, P., Eds.; PZWL: Warsaw, Poland, 2018; pp. 50–55. [Google Scholar]
- Whittemore, R.; Jaser, S.; Guo, J.; Grey, M. A Conceptual Model of Childhood Adaptation to Type 1 Diabetes. Nurs. Outlook 2010, 58, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Gruchoła, M. Pokolenie Alpha—Nowy wymiar tożsamości. Rozpr. Społeczne 2016, 10, 5–13. [Google Scholar]
- Topór-Mądry, R. Choroby przewlekłe. Obciążenie, jakość życia i konsekwencje ekonomiczne. Zdr. Publiczne Zarz. 2011, 25–49. [Google Scholar]
- Twarduś, K. Choroba przewlekła i niepełnosprawność jako sytuacje trudne w życiu dziecka i rodziny. In Modele Pielęgnowania Dziecka Przewlekle Chorego; Cepuch, G., Krzeczkowska, B., Perek, M., Twarduś, K., Eds.; PZWL: Warsaw, Poland, 2011; pp. 25–34. [Google Scholar]
- Nitka-Siemińska, A. Zespół Wypalenia u Rodziców Osób Chorujących na Schizofrenię Przewlekłą. Ph.D. Thesis, Akademia Medyczna w Gdańsku, Gdańsk, Poland, 2007. [Google Scholar]
- Heinrich, M.; Boß, K.; Wendenburg, J.; Hilgard, D.; Von Sengbusch, S.; Kapellen, T.M. Unzureichende Versorgung gefährdet Inklusion von Kindern mit Diabetes mellitus Typ 1. Diabetol. Stoffwechs. 2019, 14, 380–387. [Google Scholar]
- Ly, T.T.; Maahs, D.M.; Rewers, A.; Dunger, D.; Oduwole, A.; Jones, T.W. Assesment and management of hypoglycemia in children and adolescents with diabetes. Pediatr. Diabetes 2014, 15 (Suppl. S20), 180–192. [Google Scholar] [CrossRef] [PubMed]
- Kania, L. Hipoglikemia typu 1. Postępy Nauk Med. 2017, 30, 95–98. [Google Scholar]
- Rewers, M.J.; Pillay, K.; De Beaufort, C.; Craig, M.E.; Hanas, R.; Acerini, C.L.; Maahs, D.M. Assesment and monitoring control in children and adolescentes with diabetes. Pediatr. Diabetes 2014, 15 (Suppl. 20), 102–114. [Google Scholar] [CrossRef]
- Mianowska, B. Hipoglikemia w przebiegu cukrzycy typu 1. In Cukrzyca Typu 1; Otto-Buczkowska, E., Ed.; Cornetis: Wrocław, Poland, 2000; pp. 209–220. [Google Scholar]
- Ho, M.S.; Weller, N.J.; Ives, F.J.; Carne, C.L.; Murray, K.; vanden Driesen, R.I.; Nguyen, T.P.; Robins, P.D.; Bulsara, M.; Davis, E.A.; et al. Prevalence of structural central nervous system abnormalities in early-onset type 1 diabetes mellitus. J. Pediatr. 2008, 153, 385–390. [Google Scholar] [CrossRef]
- Stanisławska-Kubiak, M. Studia nad Wpływem Cukrzycy Typu 1 na Wybrane Parametry Zdrowia, w Tym Funkcjonowanie Psychiczne Dzieci i Młodzieży. Ph.D. Thesis, Uniwersytet Medyczny im. Karola Marcinkowskiego w Poznaniu, Poznań, Poland, 2013. [Google Scholar]
- Gonder-Frederick, L.A.; Fisher, C.D.; Ritterband, L.M.; Cox, D.J.; Hou, L.; DasGupta, A.A.; Clarke, W.L. Predictors of fear of hypoglycemia in adolescents with type 1 diabetes and their parents. Pediatr. Diabetes 2006, 7, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Majidi, S.; Driscoll, K.A.; Raymond, J.K. Anxiety in Children and Adolescents with Type 1 Diabetes. Curr. Diabetes Rep. 2015, 15, 47. [Google Scholar] [CrossRef]
- Perantie, D.C.; Lim, A.; Wu, J.; Weaver, P.; Warren, S.L.; Sadler, M.; White, N.H.; Hershey, T. Effects of prior hypoglycemia and hyperglycemia on cognition in children with type 1 diabetes mellitus. Pediatr. Diabetes 2008, 9, 87–95. [Google Scholar] [CrossRef]
- Malone, J.I.; Hanna, S.; Saporta, S.; Mervis, R.F.; Park, C.R.; Chong, L.; Diamond, D.M. Hyperglycemia not hypoglycemia alters neuronal dendrites and impairs spatial memory. Pediatr. Diabetes 2008, 9, 531–539. [Google Scholar] [CrossRef]
- Araszkiewicz, A.; Bandurska-Stankiewicz, E.; Borys, S.; Budzyński, A.; Cyganek, K.; Cypryk, K.; Czech, A.; Czupryniak, L.; Drzewoski, J.; Dzida, G.; et al. 2023 Guidelines on the management of patients with diabetes—A position of Diabetes Poland. Curr. Top. Diabetes 2023, 3, 1–133. [Google Scholar] [CrossRef]
- Małkowska-Szkutnik, A. Choroby przewlekłe u dzieci i młodzieży jako narastający problem społeczny. Stud. BAS 2014, 89–112. [Google Scholar]
- Rybka-Król, Z. Cukrzyca, choroba przewlekła—Wybrane zagadnienia psychologiczne. In Cukrzyca. Personalizacja Terapii i Opieki nad Pacjentem; Pańkowska, E., Ed.; PZWL: Warsaw, Poland, 2017; pp. 205–256. [Google Scholar]
- Delamater, A.M.; de Wit, M.; McDarby, V.; Malik, J.A.; Hilliard, M.E.; Northam, E.; Acerini, C.L. Psychological care of children and adolescents with type 1 diabetes. Pediatr. Diabetes 2014, 15 (Suppl. S20), 232–244. [Google Scholar] [CrossRef] [PubMed]
- Bickett, A.; Tapp, H. Anxiety and Diabetes: Innovative Approaches to Management in Primary Care. Exp. Biol. Med. 2016, 241, 1724–1731. [Google Scholar] [CrossRef] [PubMed]
- Beesdo, K.; Knappe, S.; Pine, D.S. Anxiety and Anxiety Disorders in Children and Adolescents: Developmental Issues and Implications for DSM-V. Psychiatr. Clin. N. Am. 2009, 32, 483–524. [Google Scholar] [CrossRef] [PubMed]
- Butwicka, A.; Frisén, L.; Almqvist, C.; Zethelius, B.; Lichtenstein, P. Risks of Psychiatric Disorders and Suicide Attempts in Children and Adolescents with Type 1 Diabetes: A Population-Based Cohort Study. Diabetes Care 2015, 38, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Hanlan, M.E.; Griffith, J.; Patel, N.; Jaser, S.S. Eating Disorders and Disordered Eating in Type 1 Diabetes: Prevalence, Screening, and Treatment Options. Curr. Diab. Rep. 2013, 13, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Balhara, Y.P. Diabetes Mellitus and Suicide. Indian J. Endocrinol. Metab. 2014, 18, 468. [Google Scholar] [CrossRef] [PubMed]
- Pisula, A. Zaburzenia psychiczne w cukrzycy. In Cukrzyca. Personalizacja Terapii i Opieki nad Pacjentem; Pańkowska, E., Ed.; PZWL: Warsaw, Poland, 2017. [Google Scholar]
- Corathers, S.D.; Kichler, J.; Jones, N.-H.Y.; Houchen, A.; Jolly, M.; Morwessel, N.; Crawford, P.; Dolan, L.M.; Hood, K.K. Improving Depression Screening for Adolescents with Type 1 Diabetes. Pediatrics 2013, 132, e1395–e1402. [Google Scholar] [CrossRef] [PubMed]
- Juruć, A.; Kubiak, M.; Wierusz-Wysocka, B. Psychological and medical problems in prevention and treatment of eating disorders among people with type 1 diabetes. Clin. Diabetol. 2016, 5, 26–31. [Google Scholar] [CrossRef][Green Version]
- Young, V.; Eiser, C.; Johnson, B.; Brierley, S.; Epton, T.; Elliott, J.; Heller, S. Eating problems in adolescents with type 1 diabetes: Systematic review with meta-analysis. Diabet. Med. 2013, 30, 189–198. [Google Scholar] [CrossRef]
- Kamińska, A.; Bronisz, A.; Bronisz, M.; Bonisławska, E.; Mielcarek, M.; Gierach, M.; Junik, R. Ocena realizacji zaleceń Polskiego Towarzystwa Diabetologicznego w zakresie wyrównania cukrzycy u chorych leczonych w poradni endokrynologiczno-diabetologicznej. Diabetol. Prakt. 2010, 11, 160–166. [Google Scholar]
- Kamińska-Jackowiak, O.; Malatyńska, A.; Chobot, A.; Gajewska, A.K. Dostępność opieki psychologicznej w placówkach diabetologii dziecięcej—Realna potrzeba? Pediatr. Endocrinol. Diabetes Metab. 2023, 29, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Golińska, P.; Bidzan, M. Poczucie obciążenia opiekunów z chorobą Parkinsona. Przegląd badań. Geriatria 2017, 11, 22–28. [Google Scholar]
- Wojnarowska, B. Uczniowie z Chorobami Przewlekłymi. Jak Wspierać Ich Rozwój, Zdrowie, Edukację; Wydawnictwo Naukowe PWN: Warsaw, Poland, 2010. [Google Scholar]
- Karta Praw Nauczyciela (Dz. U. z 2017r. 1189 i 2203) Rozdz. 2 art. 6. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19820030019/U/D19820019Lj.pdf (accessed on 10 April 2024).
- Dyczewski, L.; Wadowski, D. Wstęp. In Tożsamość Polska w Odmiennych Kontekstach; Dyczewski, L., Wadowski, D., Eds.; Wydawnictwo KUL: Lublin, Poland, 2009; pp. 5–8. [Google Scholar]
- Stunża, G.D. Edukacja wersja beta. Pokolenie Z i pokolenie Alfa a kompetencje uczestnictwa w kulturze. Kult. Pop. 2017, 86–94. [Google Scholar] [CrossRef]
- Hysa, B. Zarządzanie różnorodnością pokoleniową. Zesz. Nauk. Politech. Śląskiej 2016, 389–390. [Google Scholar]
- Twenge, J.M. iGen. Dlaczego Dzieciaki Dorastające w Sieci są Mniej Zbuntowane, Bardziej Tolerancyjne, Mniej Szczęśliwe—I Zupełnie Nieprzygotowane do Dorosłości i co to Oznacza dla Nas Wszystkich; Smak Słowa: Sopot, Poland, 2019; pp. 26–27. [Google Scholar]
- Dębski, M. Raport z Badań „Nałogowe Korzystanie z Telefonów Komórkowych. Szczegółowa Charakterystyka zjawiska Fonoholizmu w Polsce”; Fundacja Dbam o Mój Z@sięg: Gdynia, Poland, 2017. [Google Scholar]
- Kabali, H.K.; Irigoyen, M.M.; Nunez-Davis, R.; Budacki, J.G.; Mohanty, S.H.; Leister, K.P.; Bonner, R.L., Jr. Exposure and Use of Mobile Media Devices by Young Children. Pediatrics 2015, 136, 1044–1050. [Google Scholar] [CrossRef]
- Bąk, A. Korzystanie z Urządzeń Mobilnych Przez Małe Dzieci w Polsce. Wyniki Badania Ilościowego; Fundacja Dzieci Niczyje: Warsaw, Poland, 2015; Available online: http://www.mamatatatablet.pl/pliki/uploads/2015/11/Korzystanie_z_urzadzen_mobilnych_raport_final.pdf (accessed on 24 September 2023).
- Turkle, S. Samotni Razem. Dlaczego Oczekujemy Więcej od Zdobyczy Techniki, a Mniej od Siebie Nawzajem; Wydawnictwo Uniwersytetu Jagiellońskiego: Kraków, Poland, 2013; p. 7. [Google Scholar]
- Cypryk, K.; Żurawska-Kliś, M. Pompy insulinowe w dużych badaniach klinicznych. In Zastosowanie Osobistych Pomp Insulinowych w Leczeniu Chorych na Cukrzycę; Sieradzki, N.J., Ed.; PZWL: Warsaw, Poland, 2015; pp. 70–83. [Google Scholar]
- Szadkowska, A.; Gawrecki, A.; Jarosz-Chobot, P.; Myśliwiec, M.; Zozulińska-Ziółkiewicz, D. Propozycje decyzji terapeutycznych w zależności od trendów glikemii u pacjentów z cukrzycą typu 1. Pediatr. Endocrinol. Diabetes Metab. 2016, 22, 105–117. [Google Scholar] [CrossRef]
- Szredzińska, R. Zdrowie psychiczne dzieci i młodzieży. In Dzieci Się Liczą 2022. Raport o Zagrożeniach Bezpieczeństwa i Rozwoju Dzieci w Polsce; Fundacja dajemy dzieciom siłę: Warsaw, Poland, 2022; pp. 133–157. [Google Scholar]
- Kulik, M.; Małowicka, M.; Mucha, E.; Górka, A.; Ziobro, M.; Chudzicka, A. Edukacja w Cukrzycy. Brakujące Ogniwo do Osiągnięcia Sukcesu; Polskiej Federacji Edukacji w Diabetologii: Warsaw, Poland, 2015; pp. 44–52. Available online: https://www.pfed.org.pl/aktualno347ci/raport-edukacja-w-cukrzycy (accessed on 24 September 2023).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzuszek, M.; Kochman, M.; Mazur, A. Psychodiabetology: The Challenge of the Future? J. Clin. Med. 2024, 13, 2236. https://doi.org/10.3390/jcm13082236
Brzuszek M, Kochman M, Mazur A. Psychodiabetology: The Challenge of the Future? Journal of Clinical Medicine. 2024; 13(8):2236. https://doi.org/10.3390/jcm13082236
Chicago/Turabian StyleBrzuszek, Marta, Maciej Kochman, and Artur Mazur. 2024. "Psychodiabetology: The Challenge of the Future?" Journal of Clinical Medicine 13, no. 8: 2236. https://doi.org/10.3390/jcm13082236
APA StyleBrzuszek, M., Kochman, M., & Mazur, A. (2024). Psychodiabetology: The Challenge of the Future? Journal of Clinical Medicine, 13(8), 2236. https://doi.org/10.3390/jcm13082236