
Autoimmune and Non-Autoimmune Comorbidities in Myasthenic Patients of East-European Descent: A Case–Control Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Patient Clinical and Paraclinical Data
2.3. Statistical Analysis
3. Results
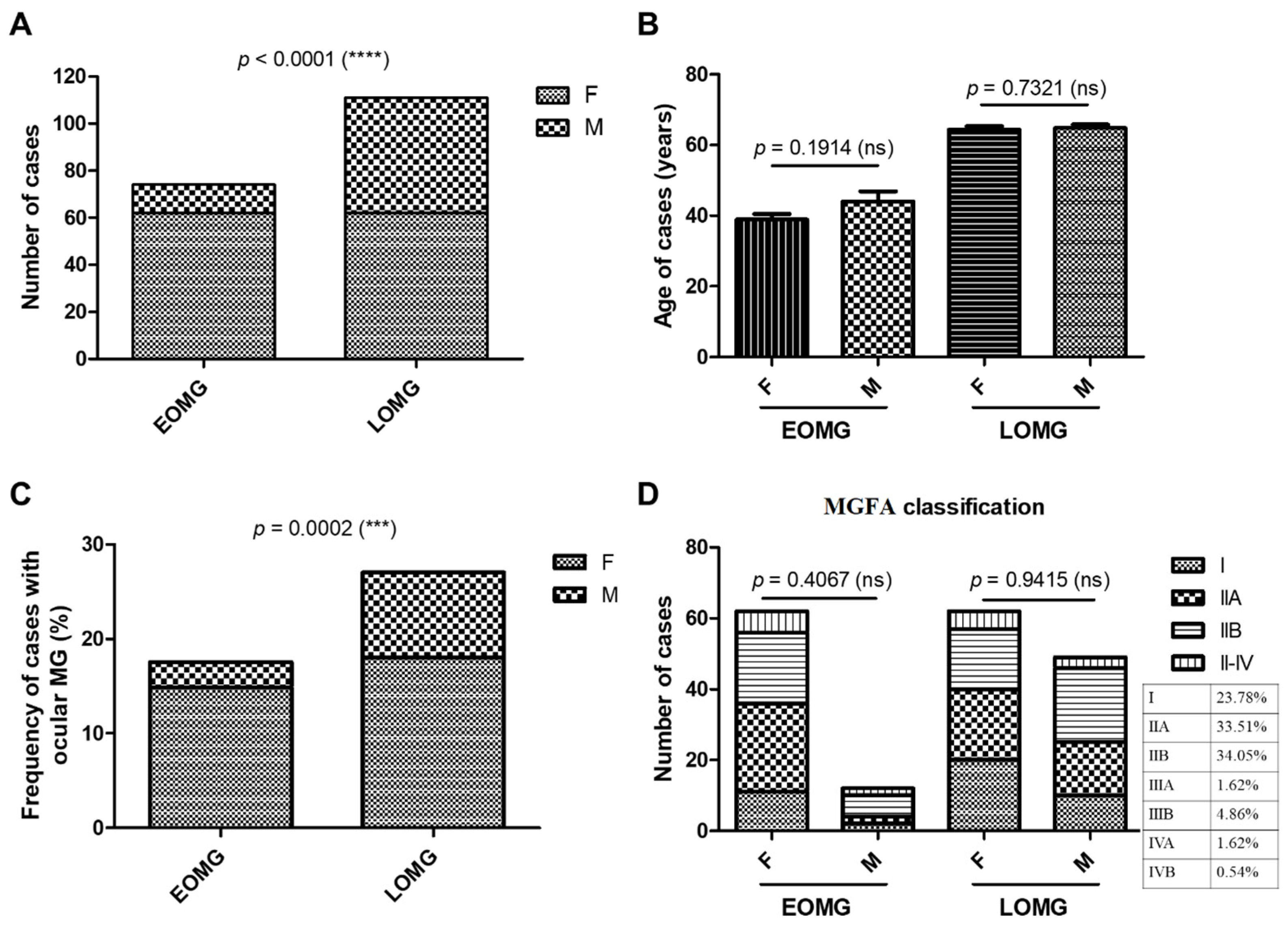
3.1. General Characteristics of MG Subjects
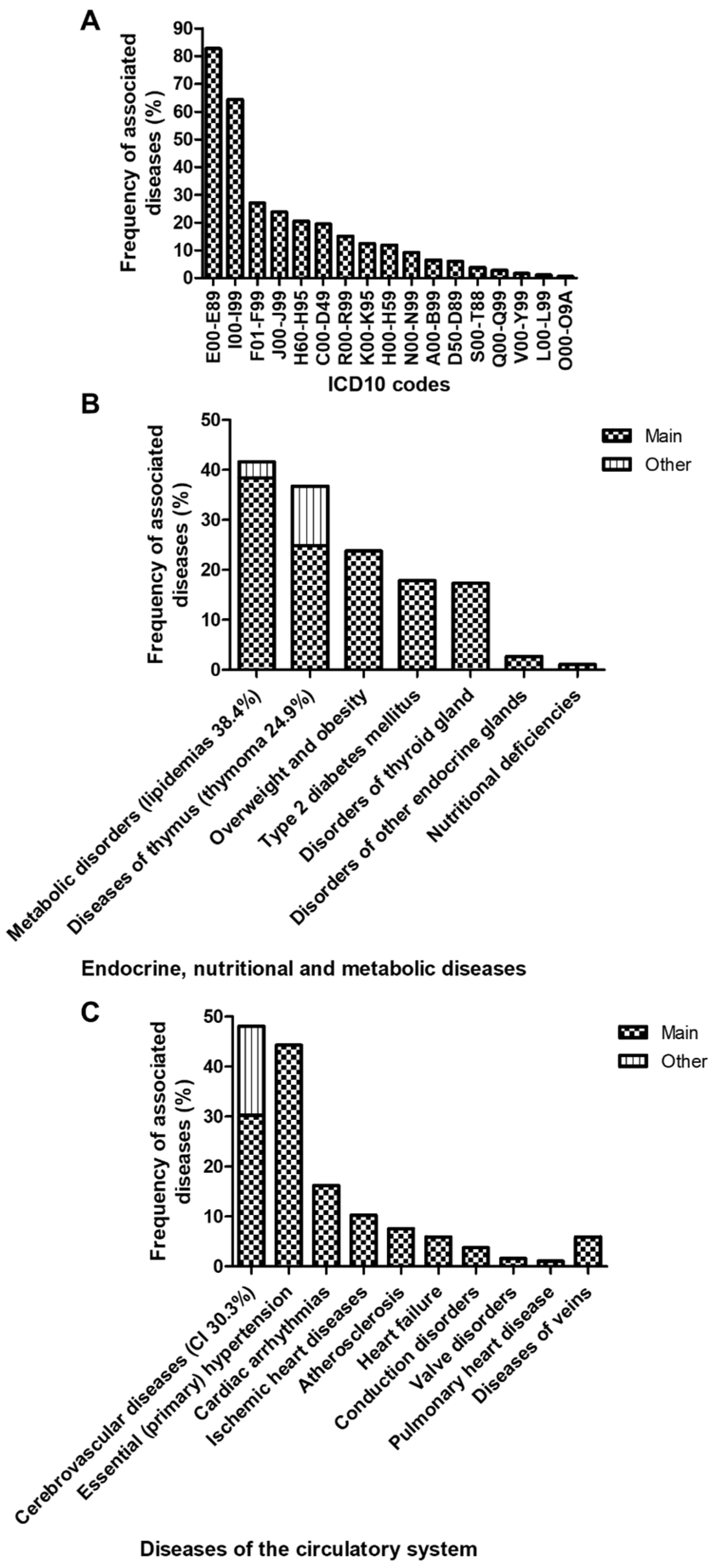
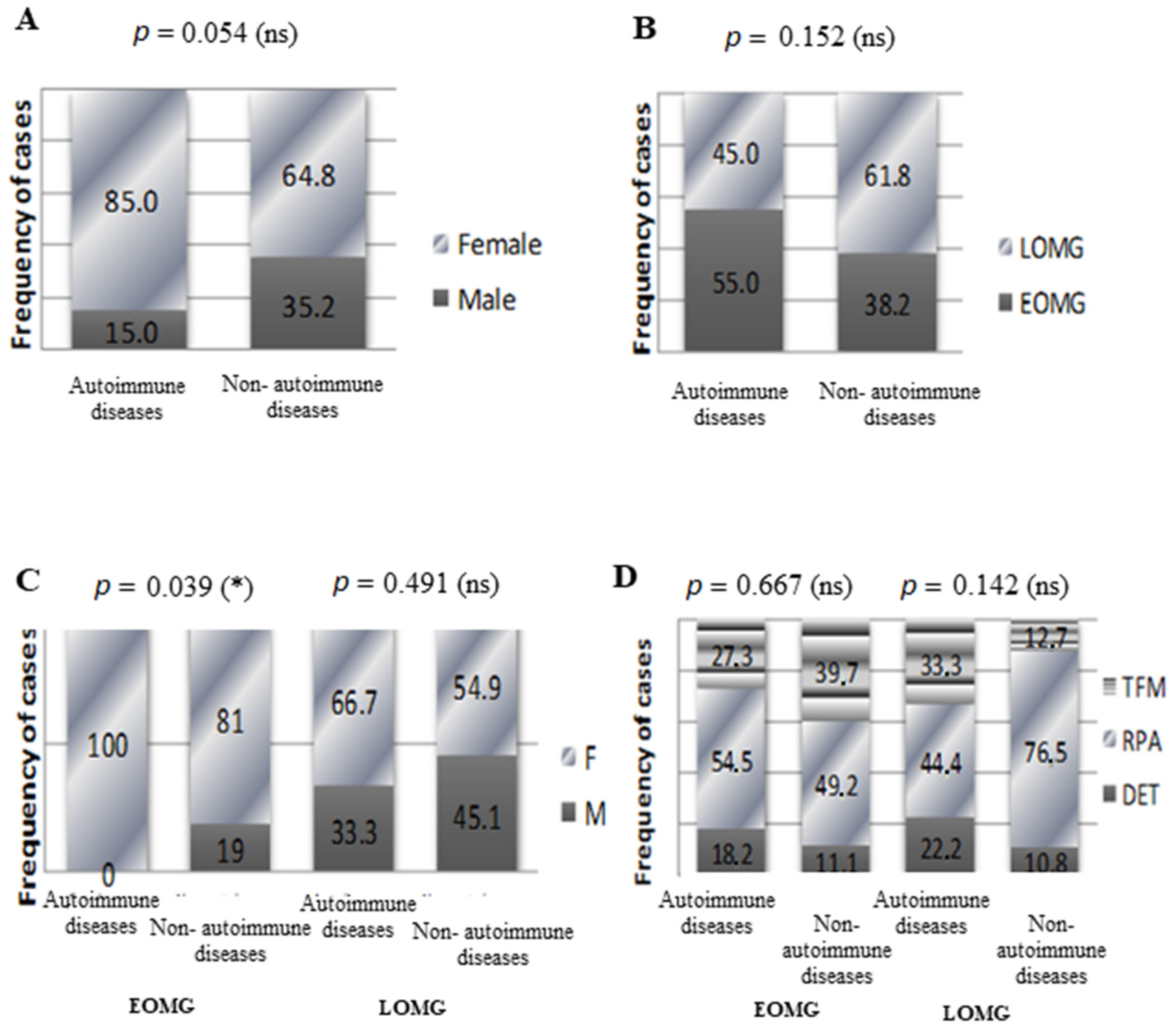
3.2. Associated Diseases in Myasthenic Patients
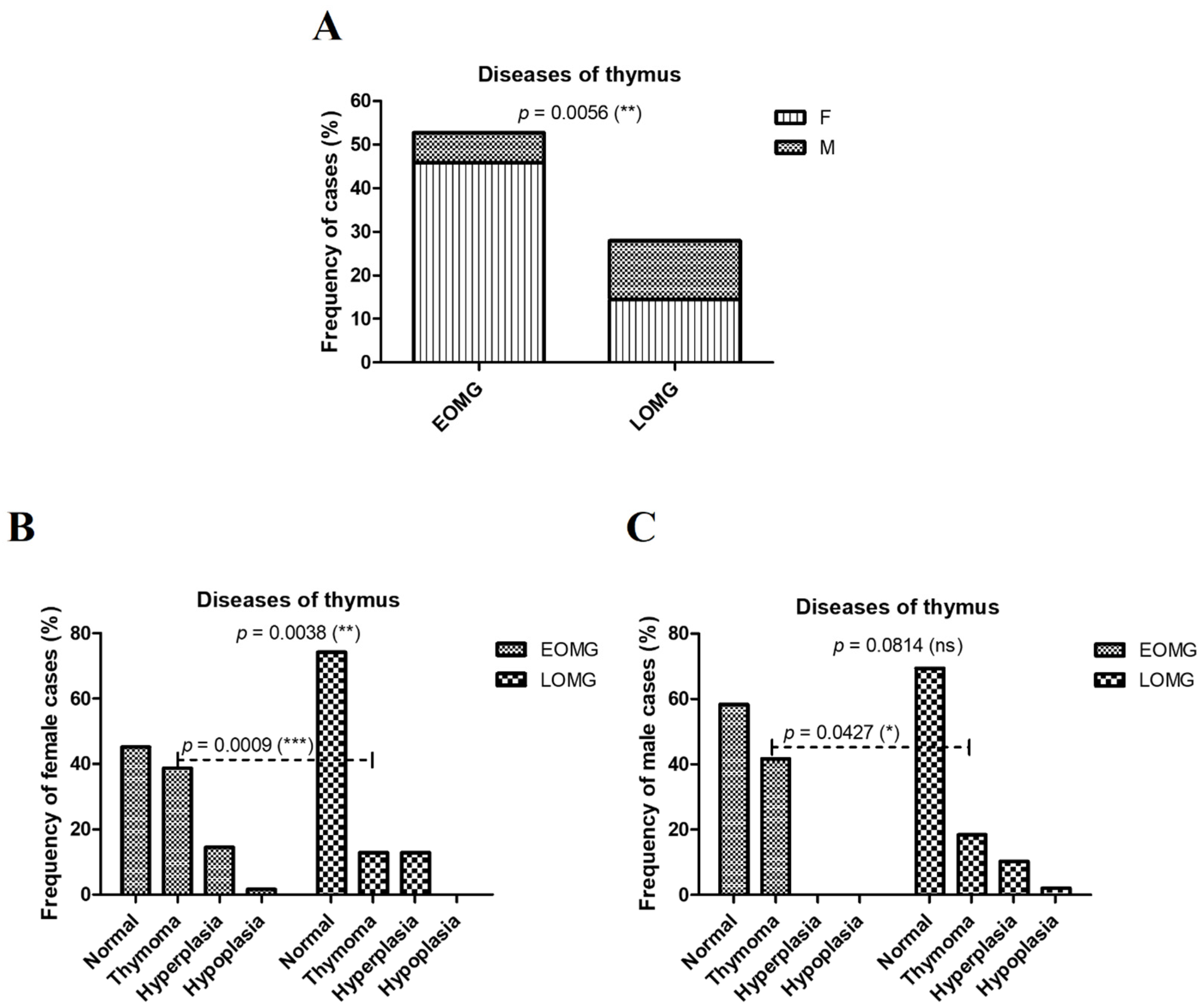
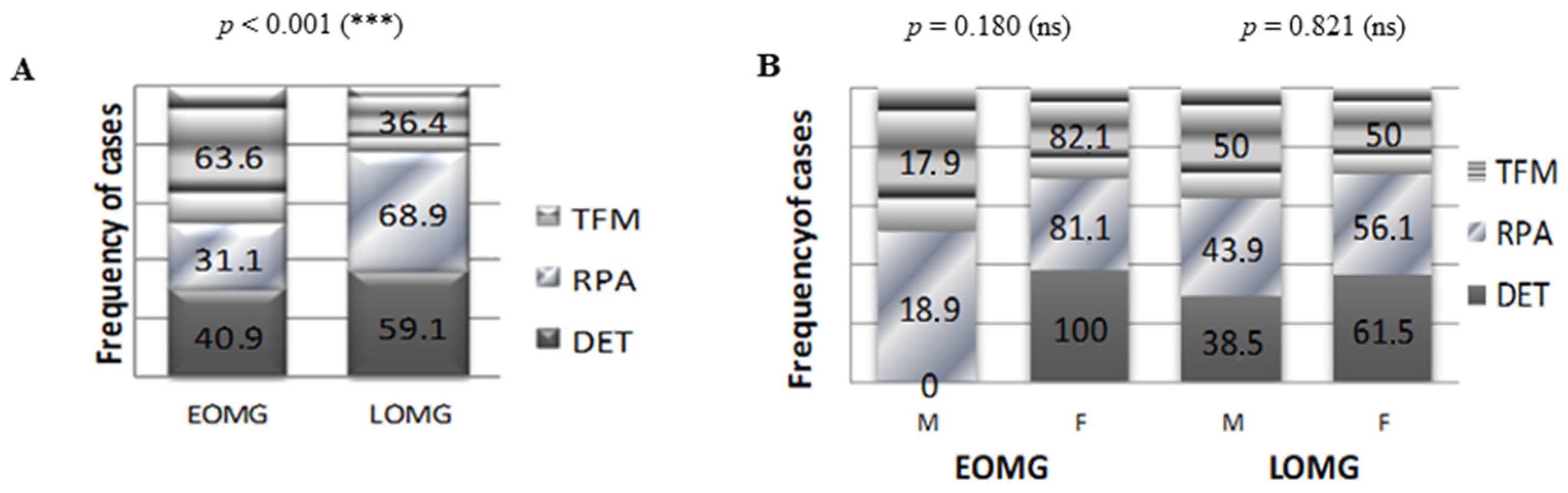
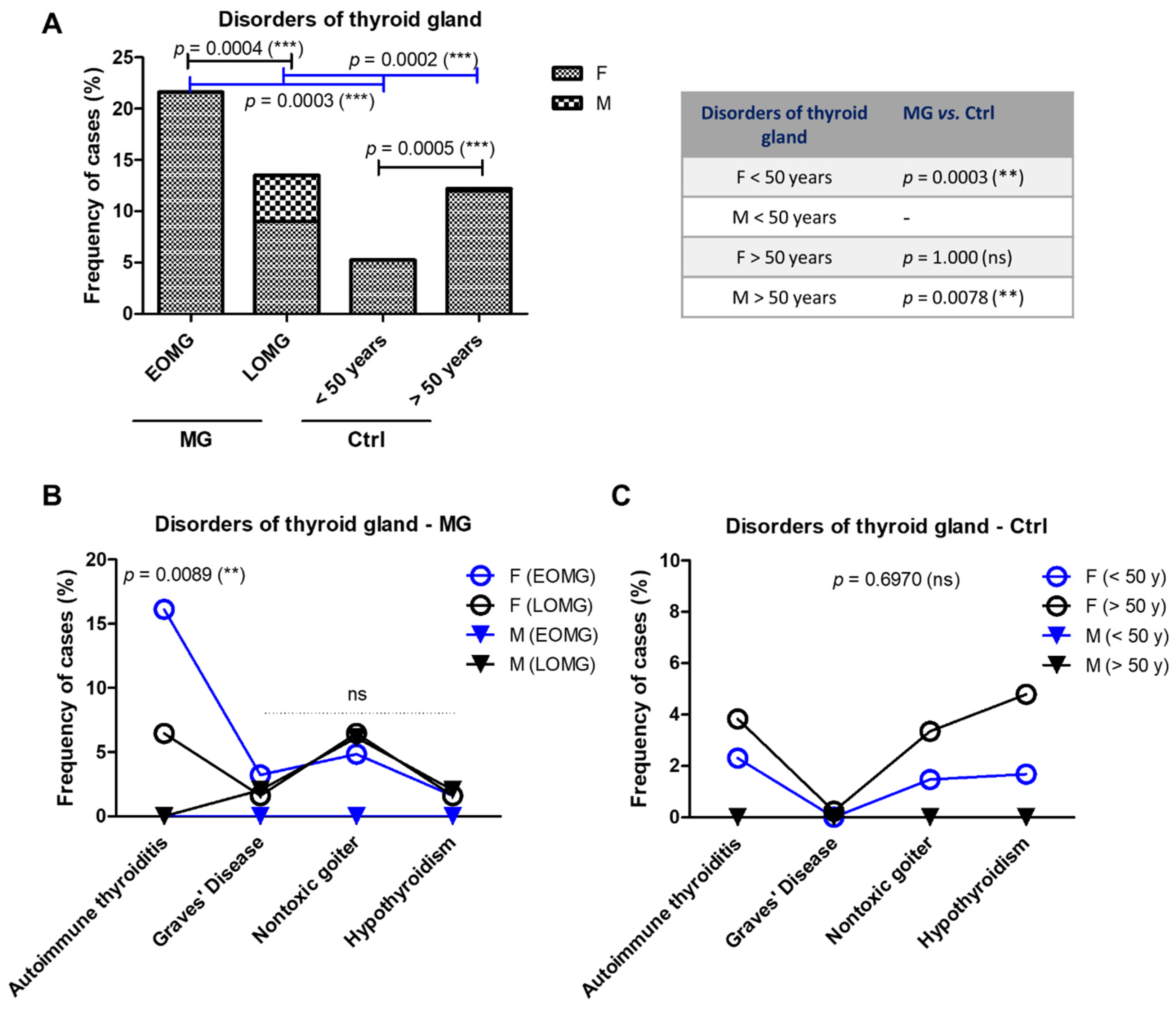
3.3. Endocrine Comorbidities in MG Patients Versus Controls
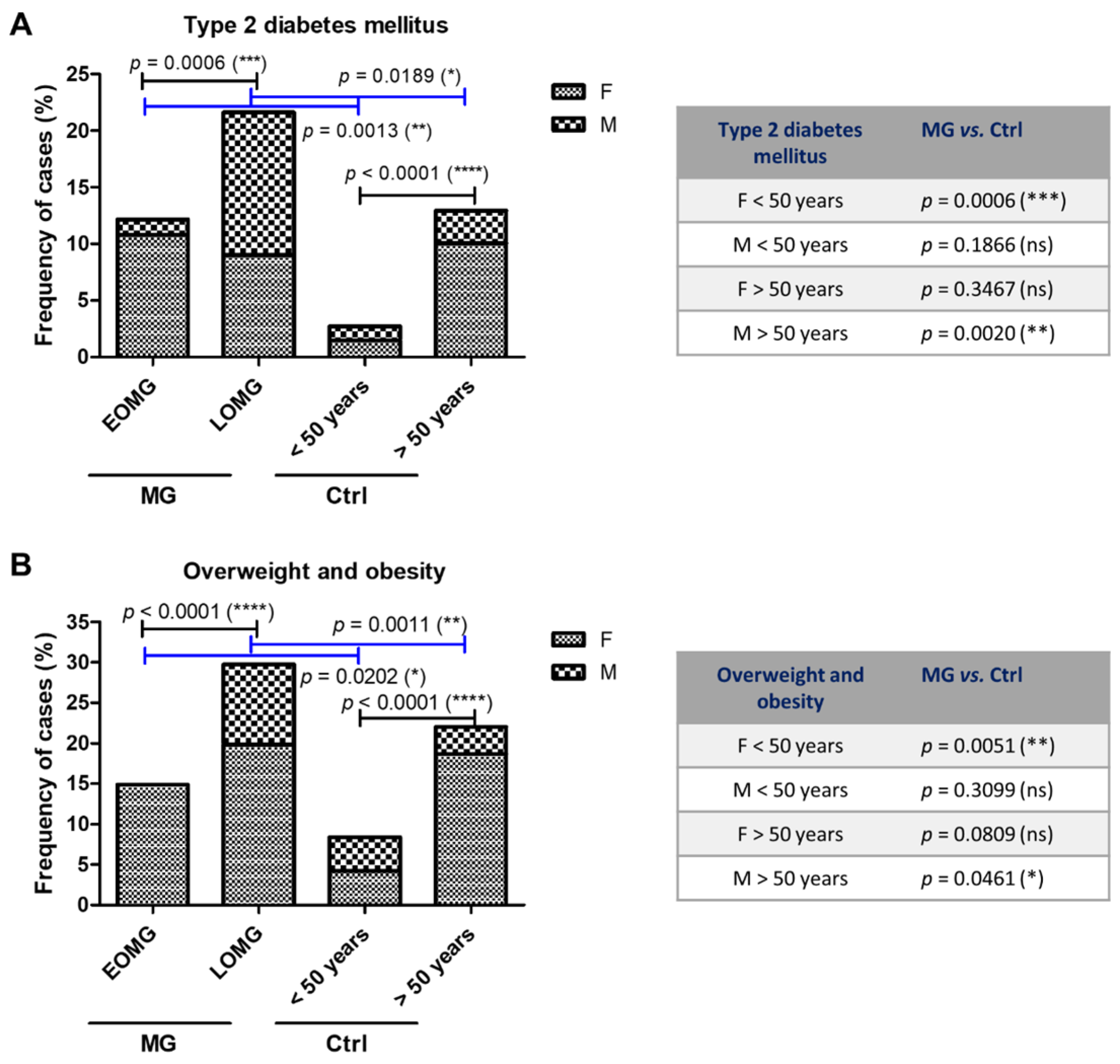
3.4. Metabolic Comorbidities in MG Patients Versus Controls
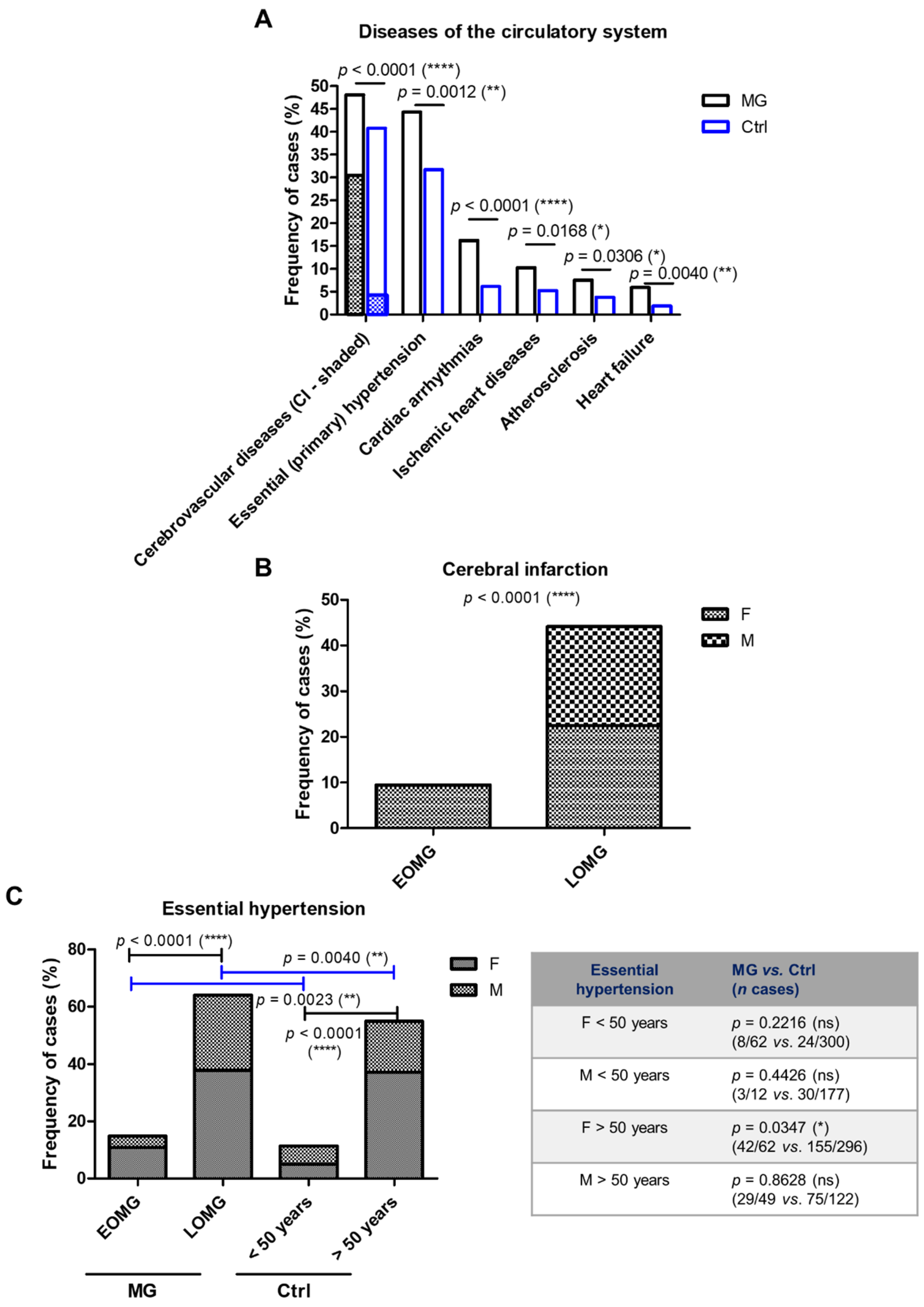
3.5. Cardiovascular Comorbidities in MG Patients Versus Controls
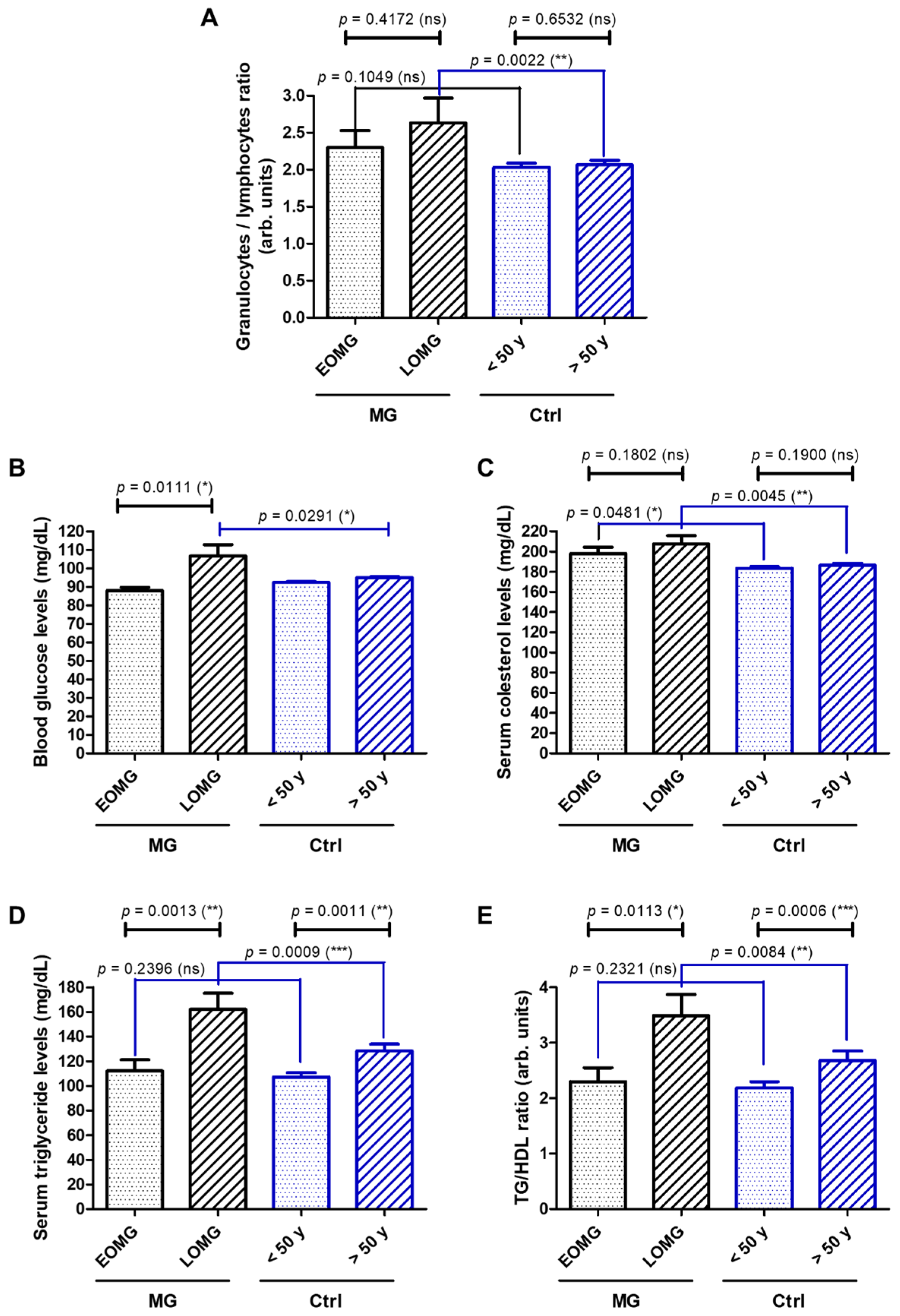
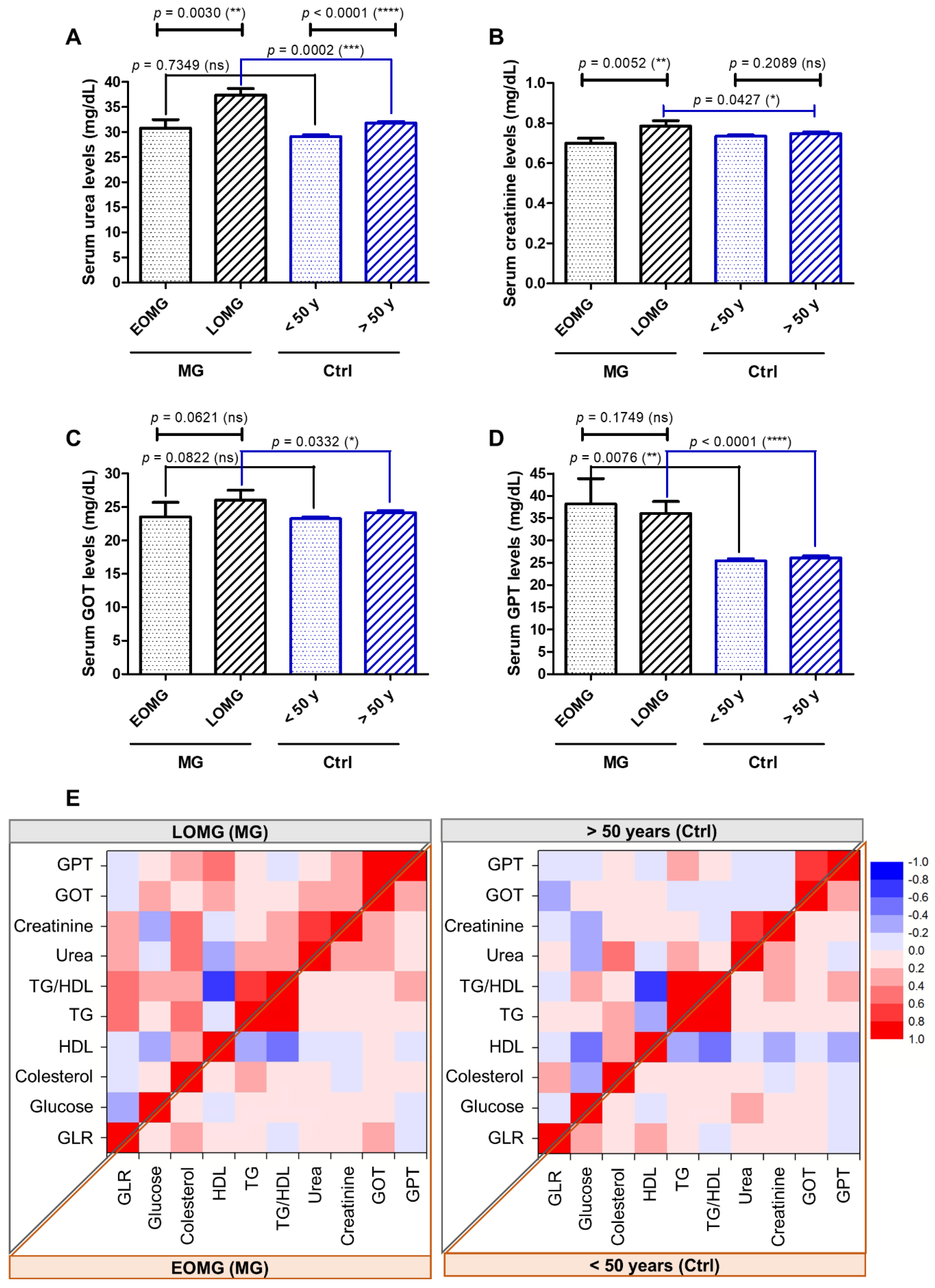
3.6. GLR, Blood Glucose, Lipidogram, and Liver and Hepatic Function in MG Patients Versus Controls
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sieb, J.P. Myasthenia gravis: An update for the clinician. Clin. Exp. Immunol. 2014, 175, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.; Palace, J.; Hilton-Jones, D. Myasthenia Gravis. Lancet 2001, 357, 2122–2128. [Google Scholar] [CrossRef] [PubMed]
- LeBien, T.W.; Tedder, T.F. B lymphocytes: How they develop and function. Blood 2008, 112, 1570–1580. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E. Myasthenia Gravis. N. Engl. J. Med. 2016, 375, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Meriggioli, M.N.; Sanders, D.B. Autoimmune myasthenia gravis: Emerging clinical and biological heterogeneity. Lancet Neurol. 2009, 8, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Melzer, N.; Ruck, T.; Fuhr, P.; Gold, R.; Hohlfeld, R.; Marx, A.; Melms, A.; Tackenberg, B.; Schalke, B.; Schneider-Gold, C.; et al. Clinical features, pathogenesis, and treatment of myasthenia gravis: A supplement to the Guidelines of the German Neurological Society. J. Neurol. 2016, 263, 1473–1494. [Google Scholar] [CrossRef] [PubMed]
- Huda, R. Inflammation and autoimmune myasthenia gravis. Front. Immunol. 2023, 14, 1110499. [Google Scholar] [CrossRef] [PubMed]
- Hasselbalch, I.C.; Søndergaard, H.B.; Koch-Henriksen, N.; Olsson, A.; Ullum, H.; Sellebjerg, F.; Oturai, A.B. The neutrophil-to-lymphocyte ratio is associated with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2018, 4, 2055217318813183. [Google Scholar] [CrossRef] [PubMed]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek Listy 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Huang, X.; Xu, M.; Wang, Y.; Zhang, Z.; Li, F.; Chen, X.; Zhang, Y. The systemic inflammation markers as possible indices for predicting respiratory failure and outcome in patients with myasthenia gravis. Ann. Clin. Transl. Neurol. 2023, 10, 98–110. [Google Scholar] [CrossRef]
- Liu, H.; Tabuchi, T.; Takemura, A.; Kasuga, T.; Motohashi, G.; Hiraishi, K.; Katano, M.; Nakada, I.; Ubukata, H.; Tabuchi, T. The granulocyte/lymphocyte ratio as an independent predictor of tumour growth, metastasis and progression: Its clinical applications. Mol. Med. Rep. 2008, 1, 699–704. [Google Scholar] [CrossRef]
- Tabuchi, T.; Shimazaki, J.; Satani, T.; Nakachi, T.; Watanabe, Y.; Tabuchi, T. The perioperative granulocyte/lymphocyte ratio is a clinically relevant marker of surgical stress in patients with colorectal cancer. Cytokine 2011, 53, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Misra, U.K.; Kalita, J.; Singh, V.K.; Kumar, S. A study of comorbidities in myasthenia gravis. Acta Neurol. Belg. 2020, 120, 59–64. [Google Scholar] [CrossRef]
- Alfaidin, A.M.R.; Kalanjati, V.P.; Basuki, M. Comorbidities of myasthenic crisis patients according to age and gender in Dr. Soetomo General Academic Hospital, Surabaya, Indonesia in 2017-2019. Maj. Biomorfologi 2022, 32, 1–5. [Google Scholar] [CrossRef]
- Laakso, S.M.; Myllynen, C.; Strbian, D.; Atula, S. Comorbidities worsen the prognosis of generalized myasthenia gravis post-thymectomy. J. Neurol. Sci. 2021, 427, 117549. [Google Scholar] [CrossRef] [PubMed]
- Dresser, L.; Wlodarski, R.; Rezania, K.; Soliven, B. Myasthenia Gravis: Epidemiology, Pathophysiology and Clinical Manifestations. J. Clin. Med. 2021, 10, 2235. [Google Scholar] [CrossRef]
- Jaretzki, A., 3rd; Barohn, R.J.; Ernstoff, R.M.; Kaminski, H.J.; Keesey, J.C.; Penn, A.S.; Sanders, D.B. Myasthenia gravis: Recommendations for clinical research standards. Task Force of the Medical Scientific Advisory Board of the Myasthenia Gravis Foundation of America. Neurology 2000, 55, 16–23. [Google Scholar] [CrossRef]
- Popa, G.A.; Scheau, C.; Preda, E.M.; Lupescu, I.G. The thymus in myasthenic patients: Correlation between mediastinal CT imaging and histopathological findings. J. Med. Life 2012, 5, 78–84. [Google Scholar] [PubMed]
- Angum, F.; Khan, T.; Kaler, J.; Siddiqui, L.; Hussain, A. The prevalence of autoimmune disorders in women: A narrative review. Cureus 2020, 12, e8094. [Google Scholar] [CrossRef]
- Basoff, D.; Parthan, A.; Bandaru, R.; Thanataveerat, A.; Kent, M.; Hehir, M.; Habib, A. Comorbidities in patients with myasthenia gravis in the USA: A retrospective claims database analysis. Neurology 2023, 100, 2189. [Google Scholar] [CrossRef]
- Harris, L.; Graham, S.; MacLachlan, S.; Exuzides, A.; Jacob, S. A retrospective longitudinal cohort study of the clinical burden in myasthenia gravis. BMC Neurol. 2022, 22, 172. [Google Scholar] [CrossRef] [PubMed]
- Thorlacius, S.; Aarli, J.A.; Riise, T.; Matre, R.; Johnsen, H.J. Associated disorders in myasthenia gravis: Autoimmune diseases and their relation to thymectomy. Acta Neurol. Scand. 1989, 80, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Christensen, P.B.; Jensen, T.S.; Tsiropoulos, I.; Sørensen, T.; Kjaer, M.; Højer-Pedersen, E.; Rasmussen, M.J.; Lehfeldt, E. Associated autoimmune diseases in myasthenia gravis. A population-based study. Acta Neurol. Scand. 1995, 91, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Huan, X.; Zhou, L.; Xi, J.; Song, J.; Wang, Y.; Luo, S.; Zhao, C. Comorbid Autoimmune Diseases in Patients With Myasthenia Gravis: A Retrospective Cross-Sectional Study of a Chinese Cohort. Front. Neurol. 2021, 12, 790941. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, M.; Shimohata, T.; Tanaka, K.; Nishizawa, M. Clinical features of patients with myasthenia gravis associated with autoimmune diseases. Eur. J. Neurol. 2007, 14, 1403–1404. [Google Scholar] [CrossRef] [PubMed]
- Kubiszewska, J.; Szyluk, B.; Szczudlik, P.; Bartoszewicz, Z.; Dutkiewicz, M.; Bielecki, M.; Bednarczuk, T.; Kostera-Pruszczyk, A. Prevalence and impact of autoimmune thyroid disease on myasthenia gravis course. Brain Behav. 2016, 6, e00537. [Google Scholar] [CrossRef]
- Amin, S.; Aung, M.; Gandhi, F.R.; Pena Escobar, J.A.; Gulraiz, A.; Malik, B.H. Myasthenia Gravis and its Association With Thyroid Diseases. Cureus 2020, 12, e10248. [Google Scholar] [CrossRef]
- Ropper, A.H.; Samuels, M.A.; Klein, J.P. Adams and Victor’s Principles of Neurology, 10th ed.; McGraw Hill Education: New York, NY, USA; Chicago, CA, USA, 2014; pp. 1472–1483. [Google Scholar]
- Law, C.; Flaherty, C.V.; Bandyopadhyay, S. A Review of Psychiatric Comorbidity in Myasthenia Gravis. Cureus 2020, 12, e9184. [Google Scholar] [CrossRef] [PubMed]
- Schneider-Gold, C.; Gilhus, N.E. Advances and challenges in the treatment of myasthenia gravis. Ther. Adv. Neurol. Disord. 2021, 14, 17562864211065406. [Google Scholar] [CrossRef]
- Brown, E.S.; Chandler, P.A. Mood and Cognitive Changes During Systemic Corticosteroid Therapy. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 17–21. [Google Scholar] [CrossRef]
- Pasqualin, F.; Guidoni, S.V.; Ermani, M.; Pegoraro, E.; Bonifati, D.M. Outcome measures and treatment effectiveness in late onset myasthenia gravis. Neurol. Res. Pr. 2020, 2, 45. [Google Scholar] [CrossRef]
- Shivamurthy, P.; Parker, M.W. Cardiac manifestations of myasthenia gravis: A systematic review. IJC Metab. Endocr. 2014, 5, 3–6. [Google Scholar] [CrossRef]
- Suzuki, S.; Utsugisawa, K.; Yoshikawa, H.; Motomura, M.; Matsubara, S.; Yokoyama, K.; Nagane, Y.; Maruta, T.; Satoh, T.; Sato, H.; et al. Autoimmune targets of heart and skeletal muscles in myasthenia gravis. Arch. Neurol. 2009, 66, 1334–1338. [Google Scholar] [CrossRef] [PubMed]
- Kufukihara, K.; Watanabe, Y.; Inagaki, T.; Takamatsu, K.; Nakane, S.; Nakahara, J.; Ando, Y.; Suzuki, S. Cytometric cell-based assays for anti-striational antibodies in myasthenia gravis with myositis and/or myocarditis. Sci. Rep. 2019, 9, 5284. [Google Scholar] [CrossRef] [PubMed]
- Sholter, D.E.; Armstrong, P.W. Adverse effects of corticosteroids on the cardiovascular system. Can. J. Cardiol. 2000, 16, 505–511. [Google Scholar] [PubMed]
- Chen, X.; Andresen, B.T.; Hill, M.; Zhang, J.; Booth, F.; Zhang, C. Role of Reactive Oxygen Species in Tumor Necrosis Factor-alpha Induced Endothelial Dysfunction. Curr. Hypertens. Rev. 2008, 4, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Okdahl, T.; Wegeberg, A.M.; Pociot, F.; Brock, B.; Størling, J.; Brock, C. Low-grade inflammation in type 2 diabetes: A cross-sectional study from a Danish diabetes outpatient clinic. BMJ Open 2022, 12, e062188. [Google Scholar] [CrossRef]
- León-Pedroza, J.I.; González-Tapia, L.A.; del Olmo-Gil, E.; Castellanos-Rodríguez, D.; Escobedo, G.; González-Chávez, A. Inflamación sistémica de grado bajo y su relación con el desarrollo de enfermedades metabólicas: De la evidencia molecular a la aplicación clínica [Low-grade systemic inflammation and the development of metabolic diseases: From the molecular evidence to the clinical practice]. Cir 2015, 83, 543–551. (In Spanish) [Google Scholar] [CrossRef]
- Danesh, J.; Whincup, P.; Walker, M.; Lennon, L.; Thomson, A.; Appleby, P.; Gallimore, J.R.; Pepys, M.B. Low grade inflammation and coronary heart disease: Prospective study and updated meta-analyses. BMJ 2000, 321, 199–204. [Google Scholar] [CrossRef]
- Arnold, N.; Lechner, K.; Waldeyer, C.; Shapiro, M.D.; Koenig, W. Inflammation and Cardiovascular Disease: The Future. Eur. Cardiol. 2021, 16, e20. [Google Scholar] [CrossRef]
- Kelley, C.; Vander Molen, J.; Choi, J.; Bhai, S.; Martin, K.; Cochran, C.; Puthanveetil, P. Impact of Glucocorticoids on Cardiovascular System-The Yin Yang Effect. J. Pers. Med. 2022, 12, 1829. [Google Scholar] [CrossRef] [PubMed]
- McKay, L.I.; Cidlowski, J.A. Physiologic and Pharmacologic Effects of Corticosteroids. In Holland-Frei Cancer Medicine, 6th ed.; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Bast, R.C., Gansler, T.S., Holland, J.F., Frei, E., Eds.; BC Decker Inc.: Hamilton, ON, Canada, 2003. [Google Scholar]
- Johnson, S.; Katyal, N.; Narula, N.; Govindarajan, R. Adverse Side Effects Associated with Corticosteroid Therapy: A Study in 39 Patients with Generalized Myasthenia Gravis. Med. Sci. Monit. 2021, 27, e933296. [Google Scholar] [CrossRef]
- Molin, C.J.; Westerberg, E.; Punga, A.R. Profile of upregulated inflammatory proteins in sera of Myasthenia Gravis patients. Sci. Rep. 2017, 7, 39716. [Google Scholar] [CrossRef]
- Wulaningsih, W.; Holmberg, L.; Abeler-Doner, L.; Ng, T.; Rohrmann, S.; Van Hemelrijck, M. Associations of C-Reactive Protein, Granulocytes and Granulocyte-to-Lymphocyte Ratio with Mortality from Breast Cancer in Non-Institutionalized American Women. PLoS ONE 2016, 11, e0157482, Erratum in: PLoS ONE 2016, 11, e0161418. [Google Scholar] [CrossRef]
- Jiang, Z.; Ning, Z.; Yang, L.; Chen, B.; Tang, J.; Zhang, J.; Fang, H.; Xu, R.; Guo, F.; Chen, M.; et al. The correlation of neutrophil-to-lymphocyte ratio with the presence and short-time curative effect of myasthenia gravis in children: A retrospectively study. Int. J. Neurosci. 2021, 131, 894–901. [Google Scholar] [CrossRef]
- Yang, D.H.; Qian, M.Z.; Wei, M.M.; Li, J.; Yu, M.M.; Lu, X.M.; Yang, H.; Lin, H.; Li, X.; Zhu, J.Y.; et al. The correlation of neutrophil-to-lymphocyte ratio with the presence and activity of myasthenia gravis. Oncotarget 2017, 8, 76099–76107. [Google Scholar] [CrossRef] [PubMed]
- Duan, Z.; Jia, A.; Cui, W.; Feng, J. Correlation between neutrophil-to-lymphocyte ratio and severity of myasthenia gravis in adults: A retrospective study. J. Clin. Neurosci. 2022, 106, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Breedveld, A.; Groot Kormelink, T.; van Egmond, M.; de Jong, E.C. Granulocytes as modulators of dendritic cell function. J. Leukoc. Biol. 2017, 102, 1003–1016. [Google Scholar] [CrossRef]
- Tecchio, C.; Micheletti, A.; Cassatella, M.A. Neutrophil-derived cytokines: Facts beyond expression. Front. Immunol. 2014, 5, 508. [Google Scholar] [CrossRef]
- Uzawa, A.; Kuwabara, S.; Suzuki, S.; Imai, T.; Murai, H.; Ozawa, Y.; Yasuda, M.; Nagane, Y.; Utsugisawa, K. Roles of cytokines and T cells in the pathogenesis of myasthenia gravis. Clin. Exp. Immunol. 2021, 203, 366–374. [Google Scholar] [CrossRef]
- Conti-Fine, B.M.; Milani, M.; Kaminski, H.J. Myasthenia gravis: Past, present, and future. J. Clin. Inv. 2006, 116, 2843–2854. [Google Scholar] [CrossRef]
- Marx, A.; Willcox, N.; Leite, M.I.; Chuang, W.Y.; Schalke, B.; Nix, W.; Ströbel, P. Thymoma and paraneoplastic myasthenia gravis. Autoimmunity 2010, 43, 413–427. [Google Scholar] [CrossRef]
- Marx, A.; Yamada, Y.; Simon-Keller, K.; Schalke, B.; Willcox, N.; Ströbel, P.; Weis, C.A. Thymus and autoimmunity. Semin. Immunopathol. 2021, 43, 45–64. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, P.; Cufi, P.; Mantegazza, R.; Berrih-Aknin, S.; Bernasconi, P.; Le Panse, R. Etiology of myasthenia gravis: Innate immunity signature in pathological thymus. Autoimmun. Rev. 2013, 12, 863–874. [Google Scholar] [CrossRef] [PubMed]
- Gradolatto, A.; Nazzal, D.; Truffault, F.; Bismuth, J.; Fadel, E.; Foti, M.; Berrih-Aknin, S. Both Treg cells and Tconv cells are defective in the Myasthenia gravis thymus: Roles of IL-17 and TNF-α. J. Autoimmun. 2014, 52, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Cufi, P.; Dragin, N.; Weiss, J.M.; Martinez-Martinez, P.; De Baets, M.H.; Roussin, R.; Fadel, E.; Berrih-Aknin, S.; Le Panse, R. Implication of double-stranded RNA signaling in the etiology of autoimmune myasthenia gravis. Ann. Neurol. 2013, 73, 281–293. [Google Scholar] [CrossRef]
- Cavalcante, P.; Barzago, C.; Baggi, F.; Antozzi, C.; Maggi, L.; Mantegazza, R.; Bernasconi, P. Toll-like receptors 7 and 9 in myasthenia gravis thymus: Amplifiers of autoimmunity? Ann. N. Y. Acad. Sci. 2018, 1413, 11–24. [Google Scholar] [CrossRef]
- Kawasaki, T.; Kawai, T. Toll-like receptor signaling pathways. Front. Immunol. 2014, 5, 461. [Google Scholar] [CrossRef]
- Jurado, J.; Javidfar, J.; Newmark, A.; Lavelle, M.; Bacchetta, M.; Gorenstein, L.; D’Ovidio, F.; Ginsburg, M.E.; Sonett, J.R. Minimally invasive thymectomy and open thymectomy: Outcome analysis of 263 patients. Ann. Thorac. Surg. 2012, 94, 974–981; discussion 981–982. [Google Scholar] [CrossRef]
- Kent, M.S.; Wang, T.; Gangadharan, S.P.; Whyte, R.I. What is the prevalence of a "nontherapeutic" thymectomy? Ann. Thorac. Surg. 2014, 97, 276–282; discussion 282. [Google Scholar] [CrossRef]
- Askani, E.; Schlett, C.L.; Bamberg, F.; Agarwal, P. Läsionen des prävaskulären Mediastinums [Lesions of the prevascular mediastinum]. Radiologie 2023, 63, 160–171. (In German) [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CT | All Cases | p Value for Chi2 Test | |
|---|---|---|---|
| M (n = 61) | F (n = 124) | ||
| DET | 5 (8.2%) | 17 (13.7%) | 0.277 |
| RPA | 43 (70.5%) | 76 (61.3%) | 0.221 |
| TFM | 13 (21.3%) | 31 (25.0%) | 0.581 |
| p value for Chi2 test | p = 0.390 | ||
| MGF Class | Autoimmune Diseases (n = 20) | Non-autoimmune Diseases (n = 165) | Chi2 Test p |
|---|---|---|---|
| I | 2 (41.0%) | 41 (24.8%) | 0.139 |
| IIA | 7 (35.0%) | 55 (33.3%) | 0.882 |
| IIB | 10 (50.0%) | 54 (32.7%) | 0.126 |
| IIIA | 0 (0.0%) | 3 (1.8%) | 0.544 |
| IIIB | 0 (0.0%) | 9 (5.5%) | 0.286 |
| IVA | 1 (5.0%) | 1 (0.6%) | 0.074 |
| IVB | 0 (0.0%) | 2 (1.2%) | 0.622 |
| Parameter | MG Cases with Oral Corticotherapy (n = 48) | MG Cases (Chronic + New) Without Oral Corticotherapy (n = 59) | Chi-Squared Test p |
|---|---|---|---|
| Type 2 diabetes | 7 (14.60%) | 10 (16.90%) | 0.739 |
| Obesity | 8 (16.60%) | 13 (22.0%) | 0.322 |
| Dyslipidemia | 22 (45.80%) | 27 (45.80%) | 0.994 |
| Hypertension | 21 (43.80%) | 25 (42.40%) | 0.886 |
| Ischemic stroke | 11 (22.90%) | 17 (28.80%) | 0.489 |
| Blood glucose > 100 mg/dL | 19 (39.60%) | 20 (33.90%) | 0.544 |
| Blood glucose mean ± sd | 100.75 ± 28.09 | 96.14 ± 18.07 | 0.579 |
| GLR > 2 | 11 (22.9%) | 10 (16.90%) | 0.441 |
| GLR mean ± sd | 2.57 ± 2.59 | 2.07 ± 0.92 | 0.021 |
| Parameter | MG Cases with Oral Corticotherapy (n = 48) | MG Cases (Chronic + New) Without Oral Corticotherapy (n = 137) | Chi-Squared Test p |
|---|---|---|---|
| Type 2 diabetes | 7 (14.60%) | 26 (19.0%) | 0.486 |
| Obesity | 8 (16.60%) | 37 (27.0%) | 0.071 |
| Dyslipidemia | 22 (45.80%) | 52 (38.0%) | 0.340 |
| Hypertension | 21 (43.80%) | 76 (55.50%) | 0.926 |
| Ischemic stroke | 11 (22.90%) | 45 (32.80%) | 0.190 |
| Blood glucose > 100 mg/dL | 19 (39.60%) | 45 (32.80%) | 0.402 |
| Blood glucose mean ± sd | 100.75 ± 28.09 | 98.27 ± 26.21 | 0.412 |
| GLR > 2 | 11 (22.9%) | 22 (16.10%) | 0.296 |
| GLR mean ± sd | 2.57 ± 2.59 | 2.01 ± 0.70 | 0.349 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Croitoru, C.G.; Pavel-Tanasa, M.; Cuciureanu, D.I.; Hodorog, D.N.; Cianga, P. Autoimmune and Non-Autoimmune Comorbidities in Myasthenic Patients of East-European Descent: A Case–Control Study. J. Clin. Med. 2024, 13, 2273. https://doi.org/10.3390/jcm13082273
Croitoru CG, Pavel-Tanasa M, Cuciureanu DI, Hodorog DN, Cianga P. Autoimmune and Non-Autoimmune Comorbidities in Myasthenic Patients of East-European Descent: A Case–Control Study. Journal of Clinical Medicine. 2024; 13(8):2273. https://doi.org/10.3390/jcm13082273
Chicago/Turabian StyleCroitoru, Cristina Georgiana, Mariana Pavel-Tanasa, Dan Iulian Cuciureanu, Diana Nicoleta Hodorog, and Petru Cianga. 2024. "Autoimmune and Non-Autoimmune Comorbidities in Myasthenic Patients of East-European Descent: A Case–Control Study" Journal of Clinical Medicine 13, no. 8: 2273. https://doi.org/10.3390/jcm13082273
APA StyleCroitoru, C. G., Pavel-Tanasa, M., Cuciureanu, D. I., Hodorog, D. N., & Cianga, P. (2024). Autoimmune and Non-Autoimmune Comorbidities in Myasthenic Patients of East-European Descent: A Case–Control Study. Journal of Clinical Medicine, 13(8), 2273. https://doi.org/10.3390/jcm13082273