
Dysregulation of Inflammatory Pathways in Adult Spinal Deformity Patients with Frailty

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Inclusion and Exclusion Criteria
2.3. Collection of Radiographic, Health-Related Quality of Life (HRQOL), Laboratory Data, and other Demographic Data
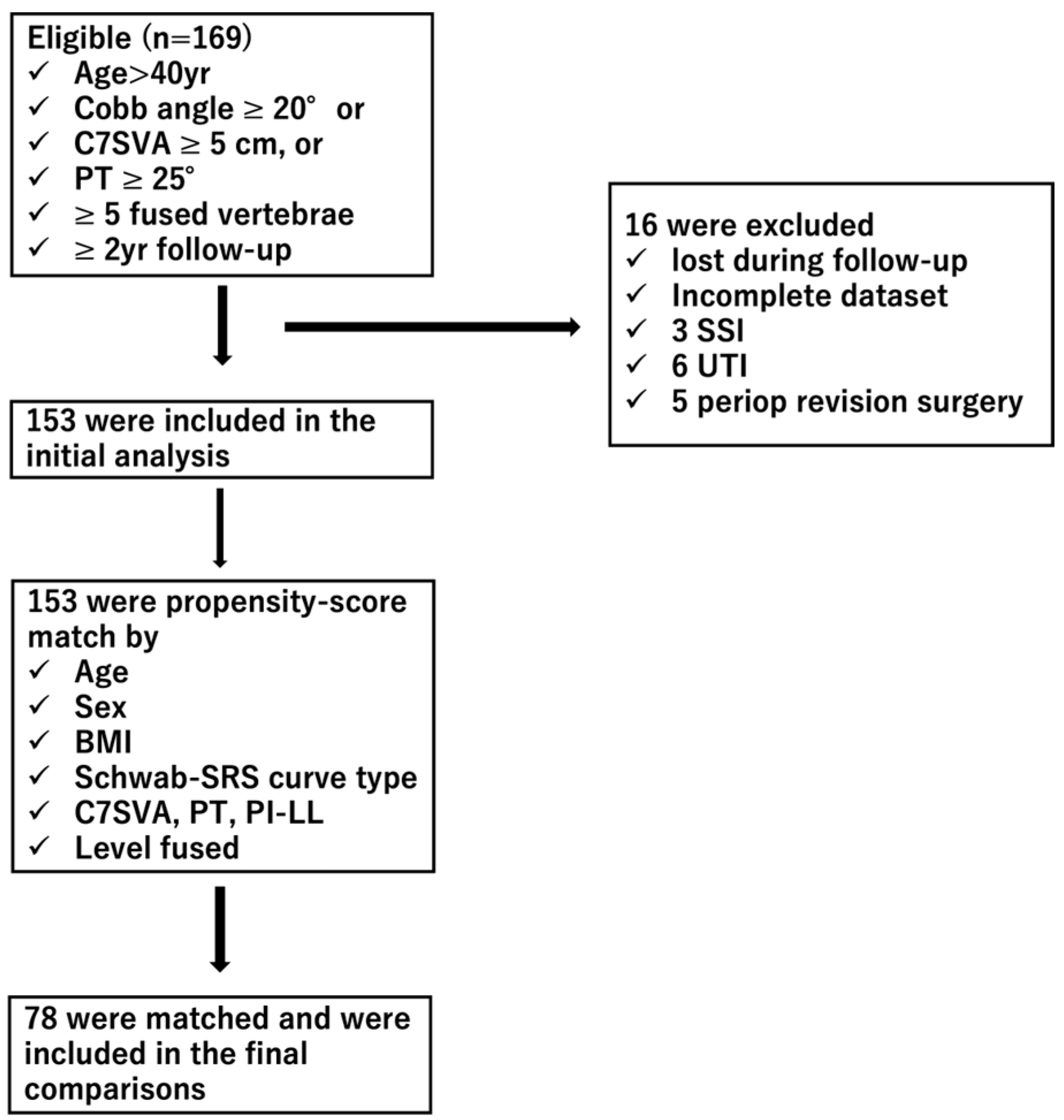
2.4. Propensity Score Matching of the Patient Cohort (Figure 1)
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Patient Cohort
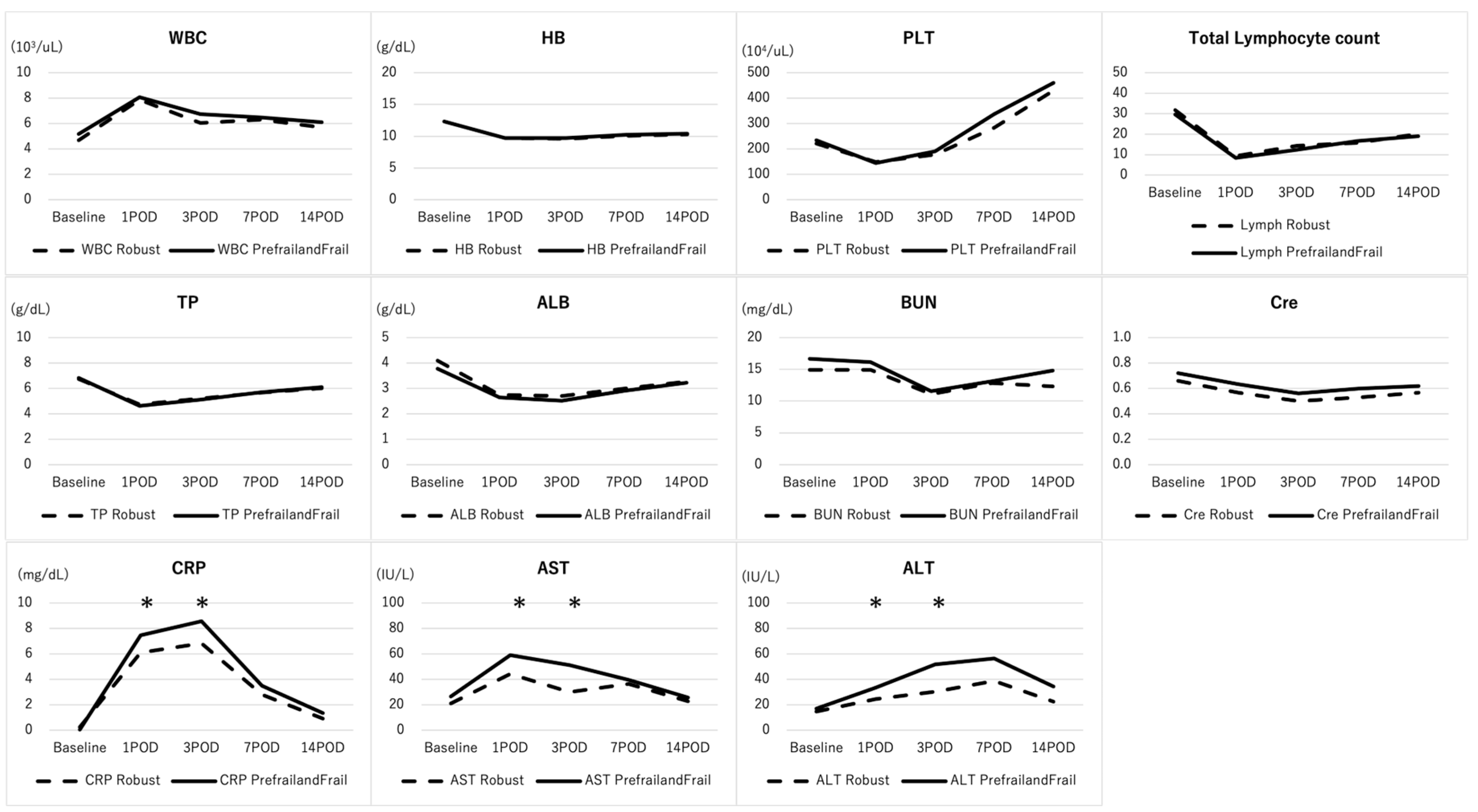
3.2. Comparisons of Baseline and Post-Operative Laboratory Data between the Robust Group and Prefrail/Frail Group
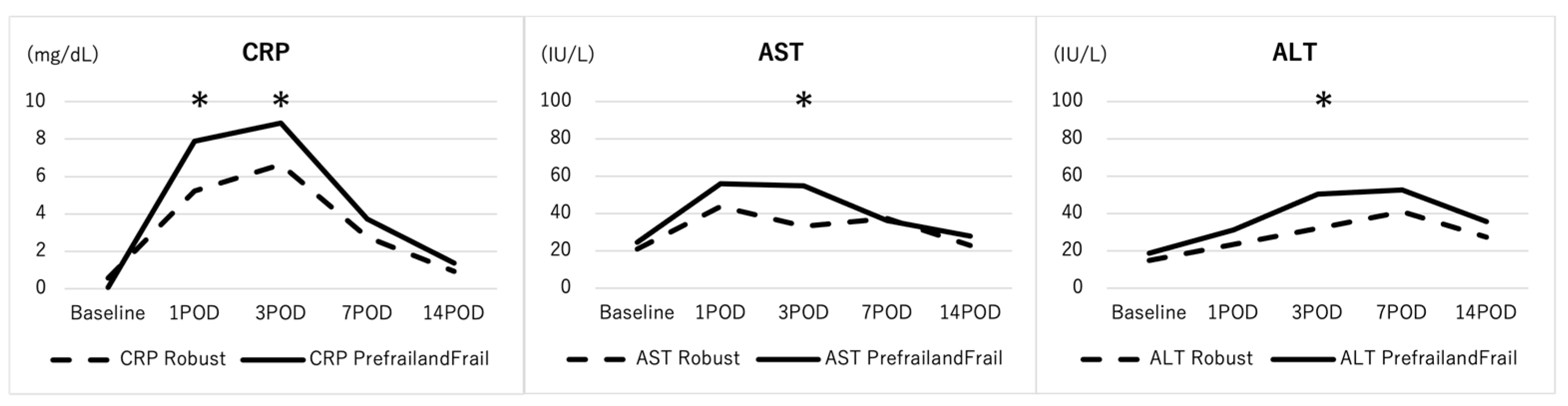
3.3. Comparisons of Baseline and Post-Operative Laboratory Data in the Propensity-Score Matched Patient Cohort
3.4. Correlation between Frailty (mFI-11) and Baseline Biomarkers in the Prefrail and Frail Patient Group
3.5. Correlation between Baseline Biomarkers and Baseline and 2-Year Post-Operative HRQOLs in the Prefrail and Frail Patient Group
3.6. Correlation between Post-Operative Serum CRP Level, Transaminase, and 2-Year Post-Operative HRQOLs in the Prefrail and Frail Patient Group
3.7. Comparison of Baseline Biomarkers between ASD Patients Who Developed Severe Adverse Events during Follow-Up and Those Who Did Not in Prefrail/Frail Patients
4. Discussion
4.1. Baseline Difference for Biomarkers between Robust and Prefrail/Frail Patients in ASD Surgery
4.2. The Elevation of Inflammatory Pathway and Coagulation Pathway Biomarkers in ASD Patients
4.3. The Correlation between Inflammatory Biomarkers and Clinical Outcomes in ASD Patients
4.4. The Correlation between Biomarkers and Clinical Outcomes and Severe Adverse Events in ASD Patients
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirza, S.K.; Deyo, R.A.; Heagerty, P.J.; Turner, J.A.; Lee, L.A.; Goodkin, R. Towards standardized measurement of adverse events in spine surgery: Conceptual model and pilot evaluation. BMC Musculoskelet. Disord. 2006, 7, 53. [Google Scholar] [CrossRef] [PubMed]
- Flexman, A.M.; Charest-Morin, R.; Stobart, L.; Street, J.; Ryerson, C.J. Frailty and postoperative outcomes in patients undergoing surgery for degenerative spine disease. Spine J. 2016, 16, 1315–1323. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Fujita, N.; Okada, E.; Tsuji, O.; Nagoshi, N.; Asazuma, T.; Watanabe, K. Clinical outcomes, complications and cost-effectiveness in surgically treated adult spinal deformity over 70-years -A propensity-score matched analysis. Clin. Spine Surg. 2020, 33, E14–E20. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Michikawa, T.; Suzuki, S.; Okada, E.; Nori, S.; Tsuji, O.; Nagoshi, N.; Asazuma, T.; Hosogane, N.; Fujita, N.; et al. Characterization of Patients with Poor Risk for Clinical Outcomes in Adult Symptomatic Lumbar Deformity Surgery. Spine 2021, 46, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Shaffrey, C.I.; Lafage, V.; Schwab, F.; Scheer, J.K.; Protopsaltis, T.; Klineberg, E.; Gupta, M.; Hostin, R.; Fu, K.-M.G.; et al. Comparison of best versus worst clinical outcomes for adult spinal deformity surgery: A retrospective review of a prospectively collected, multicenter database with 2-year follow-up. J. Neurosurg. Spine 2015, 23, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Michikawa, T.; Hosogane, N.; Fujita, N.; Okada, E.; Suzuki, S.; Tsuji, O.; Nagoshi, N.; Asazuma, T.; Tsuji, T.; et al. The 5-Item Modified Frailty Index Is Predictive of Severe Adverse Events in Patients Undergoing Surgery for Adult Spinal Deformity. Spine 2019, 44, E1083–E1091. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Fujita, N.; Okada, E.; Tsuji, O.; Nagoshi, N.; Tsuji, T.; Asazuma, T.; Nakamura, M.; Matsumoto, M.; Watanabe, K. Impact of Frailty and Comorbidities on Surgical Outcomes and Complications in Adult Spinal Disorders. Spine 2018, 43, 1259–1267. [Google Scholar] [CrossRef] [PubMed]
- Leven, D.M.; Lee, N.J.; Kothari, P.; Steinberger, J.; Guzman, J.; Skovrlj, B.; Shin, J.I.; Caridi, J.M.; Cho, S.K. Frailty Index Is a Significant Predictor of Complications and Mortality After Surgery for Adult Spinal Deformity. Spine 2016, 41, E1394–E1401. [Google Scholar] [CrossRef]
- Miller, E.K.; Neuman, B.J.; Jain, A.; Daniels, A.H.; Ailon, T.; Sciubba, D.M.; Kebaish, K.M.; Lafage, V.; Scheer, J.K.; Bess, S.; et al. An assessment of frailty as a tool for risk stratification in adult spinal deformity surgery. Neurosurg. Focus. 2017, 43, E3. [Google Scholar] [CrossRef]
- Pitter, F.T.; Lindberg-Larsen, M.; Pedersen, A.B.; Dahl, B.; GehrchenReadmissions, M. Length of Stay and Mortality after Primary Surgery for Adult Spinal Deformity: A Ten-Year Danish Nationwide Cohort Study. Spine 2019, 44, E107–E116. [Google Scholar] [CrossRef]
- Parfentjev, I.A. Frailty of old age and bacterial allergy. Geriatrics 1956, 11, 260–262. [Google Scholar] [PubMed]
- Ali, R.; Schwalb, J.M.; Nerenz, D.R.; Antoine, H.J.; Rubinfeld, I. Use of the modified frailty index to predict 30-day morbidity and mortality from spine surgery. J. Neurosurg. Spine 2016, 25, 537–541. [Google Scholar] [CrossRef]
- Velanovich, V.; Antoine, H.; Swartz, A.; Peters, D.; Rubinfeld, I. Accumulating deficits model of frailty and postoperative mortality and morbidity: Its application to a national database. J. Surg. Res. 2013, 183, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Karam, J.; Tsiouris, A.; Shepard, A.; Velanovich, V.; Rubinfeld, I. Simplified frailty index to predict adverse outcomes and mortality in vascular surgery patients. Ann. Vasc. Surg. 2013, 27, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Manwani, B.; Leng, S.X. Frailty, inflammation, and immunity. Aging Dis. 2011, 2, 466–473. [Google Scholar] [PubMed]
- Gao, X.; Li, H.; Leng, S.X. Inflammation and immune system alterations in frailty. Clin. Geriatr. Med. 2011, 27, 79–87. [Google Scholar]
- Kanapuru, B.; Ershler, W.B. Inflammation, coagulation, and the pathway to frailty. Am. J. Med. 2009, 122, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Le Couteur, D.G.; Blyth, F.M.; Creasey, H.M.; Handelsman, D.J.; Naganathan, V.; Sambrook, P.N.; Seibel, M.J.; Waite, L.M.; Cumming, R.G. The association of alanine transaminase with aging, frailty, and mortality. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 712–717. [Google Scholar] [CrossRef]
- Vespasiani-Gentilucci, U.; De Vincentis, A.; Ferrucci, L.; Bandinelli, S.; Incalzi, R.A.; Picardi, A. Low Alanine Aminotransferase Levels in the Elderly Population: Frailty, Disability, Sarcopenia, and Reduced Survival. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 925–930. [Google Scholar] [CrossRef]
- Maeda, D.; Kagiyama, N.; Jujo, K.; Saito, K.; Kamiya, K.; Saito, H.; Ogasahara, Y.; Maekawa, E.; Konishi, M.; Kitai, T.; et al. Aspartate aminotransferase to alanine aminotransferase ratio is associated with frailty and mortality in older patients with heart failure. Sci. Rep. 2021, 11, 11957. [Google Scholar] [CrossRef]
- Pillatt, A.P.; Silva, B.D.; Franz, L.B.B.; Berlezi, E.M.; Schneider, R.H. Muscle, endocrine, and immunological markers of frailty in older people. Exp. Gerontol. 2021, 151, 111405. [Google Scholar] [CrossRef]
- Wilhelm-Leen, E.R.; Hall, Y.N.; Tamura, M.K.; Chertow, G.M. Frailty and chronic kidney disease: The Third National Health and Nutrition Evaluation Survey. Am. J. Med. 2009, 122, 664–671.e2. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Zhuo, Y.; Xie, L.; Wang, H.; Yang, M. Sarcopenia index based on serum creatinine and cystatin C is associated with 3-year mortality in hospitalized older patients. Sci. Rep. 2020, 10, 1260. [Google Scholar] [CrossRef]
- Patel, A.; Zhang, M.; Liao, G.; Karkache, W.; Montroy, J.; Fergusson, D.A.; Khadaroo, R.G.; Tran, D.T.T.; McIsaac, D.I.; Lalu, M.M. A Systematic Review and Meta-analysis Examining the Impact of Age on Perioperative Inflammatory Biomarkers. Anesth. Analg. 2022, 134, 751–764. [Google Scholar] [CrossRef] [PubMed]
- Plas, M.; Rutgers, A.; van der Wal-Huisman, H.; de Haan, J.J.; Absalom, A.R.; de Bock, G.H.; van Leeuwen, B.L. The association between the inflammatory response to surgery and postoperative complications in older patients with cancer; a prospective prognostic factor study. J. Geriatr. Oncol. 2020, 11, 873–879. [Google Scholar] [CrossRef]
- Saedi, A.A.; Feehan, J.; Phu, S.; Duque, G. Current and emerging biomarkers of frailty in the elderly. Clin. Interv. Aging 2019, 14, 389–398. [Google Scholar] [CrossRef]
- Terran, J.; Schwab, F.; Shaffrey, C.I.; Smith, J.S.; Moal, B.; Klineberg, E.O.; Ames, C.P.; Hostin, R.; Fu, K.-M.G.; Kebaish, K.M.; et al. The SRS-Schwab adult spinal deformity classification: Assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery 2013, 73, 559–568. [Google Scholar] [CrossRef]
- Abbott, D. Applied Predictive Analytics: Principles and Techniques for the Professional Data Analyst, 1st ed.; John Wiley & Sons, Inc.: Indianapolis, IN, USA, 2014. [Google Scholar]
- Moldovan, F.; Ivanescu, A.D.; Fodor, P.; Moldovan, L.; Bataga, T. Correlation between Inflammatory Systemic Biomarkers and Surgical Trauma in Elderly Patients with Hip Fractures. J. Clin. Med. 2023, 12, 5147. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F. Sterile Inflammatory Response and Surgery-Related Trauma in Elderly Patients with Subtrochanteric Fractures. Biomedicines 2024, 12, 354. [Google Scholar] [CrossRef]
- Shlipak, M.G.; Stehman-Breen, C.; Fried, L.F.; Psaty, B.M.; Newman, A.B. The presence of frailty in elderly persons with chronic renal insufficiency. Am. J. Kidney Dis. 2004, 43, 861–867. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Robust | Prefrail/Frail | p Value |
|---|---|---|---|
| No. of samples | 97 | 56 | |
| Age (yr.) | 61.2 ± 10.5 | 67.5 ± 8.7 | <0.01 * |
| Gender (female) | 90 (92%) | 61 (92%) | 0.97 |
| BMI (kg/m2) | 21.8 ± 3.2 | 22.2 ± 3.9 | 0.47 |
| BMD (T-score) | −1.0 ± 0.8 | −1.3 ± 0.9 | 0.03 * |
| Frailty (mFI-11) | 0 | 0.16 ± 0.09 | <0.01 * |
| Schwab-SRS type (T:D:L:N) | 8:27:43:19 (8%:28%:44%:20%) | 2:9:21:24 (4%:16%:38%:43%) | 0.01 * |
| Level fused | 9.8 ± 3.0 | 9.9 ± 2.8 | 0.89 |
| LIV (pelvis) | 48 (49%) | 34 (61%) | 0.18 |
| Application of LIF | 29 (30%) | 20 (36%) | 0.46 |
| Application of PSO | 7 (7%) | 7 (13%) | 0.27 |
| Revision surgery | 8 (8%) | 5 (9%) | 0.88 |
| TOS (min.) | 244.3 ± 85.2 | 283.3 ± 115.2 | 0.02 * |
| EBL (L) | 0.7 ± 0.6 | 0.6 ± 0.4 | 0.39 |
| Major complication | 40 (41%) | 38 (68%) | <0.01 |
| Robust | Prefrail/Frail | p Value | |
|---|---|---|---|
| Spinal alignment | |||
| Cobb angle (°) | 56.2 ± 19.1 | 36.6 ± 9.1 | 0.13 |
| C7SVA (mm) | 57.7 ± 51.3 | 100.3 ± 66.8 | <0.01 * |
| PT (°) | 31.2 ± 13.1 | 36.4 ± 9.9 | 0.02 * |
| PI-LL (°) | 34.2 ± 20.4 | 43.2 ± 23.4 | 0.04 * |
| SRS22r score | |||
| Function | 3.0 ± 0.8 | 2.8 ± 0.9 | 0.11 |
| Pain | 3.1 ± 0.8 | 2.9 ± 0.8 | 0.10 |
| Self-image | 2.1 ± 0.8 | 2.2 ± 0.7 | 0.89 |
| Mental heath | 2.8 ± 0.9 | 2.8 ± 1.1 | 0.82 |
| Satisfaction | 3.8 ± 1.2 | 3.5 ± 1.0 | 0.32 |
| Total | 2.8 ± 0.7 | 2.7 ± 0.7 | 0.44 |
| Robust | Prefrail/Frail | p Value | |
|---|---|---|---|
| Spinal alignment | |||
| Cobb angle (°) | 18.1 ± 14.3 | 15.3 ± 10.6 | 0.41 |
| C7SVA (mm) | 43.4 ± 51.0 | 77.1 ± 66.8 | <0.01 * |
| PT (°) | 27.2 ± 10.2 | 29.3 ± 10.2 | 0.07 |
| PI-LL (°) | 17.4 ± 16.2 | 20.2 ± 12.7 | 0.20 |
| SRS22r score | |||
| Function | 3.8 ± 0.8 | 3.5 ± 0.8 | 0.10 |
| Pain | 3.8 ± 0.9 | 3.6 ± 0.9 | 0.19 |
| Self-image | 3.4 ± 1.0 | 3.7 ± 0.9 | 0.32 |
| Mental heath | 3.7 ± 0.9 | 3.7 ± 0.9 | 0.60 |
| Satisfaction | 3.9 ± 0.9 | 3.8 ± 1.0 | 0.48 |
| Total | 3.7 ± 0.7 | 3.5 ± 0.7 | 0.19 |
| Variables | Robust | Prefrail/Frail | p Value |
|---|---|---|---|
| No. of samples | 39 | 39 | |
| Age (yr.) | 62.6 ± 11.1 | 66.8 ± 9.5 | 0.25 |
| Gender (female) | 38 (97%) | 35 (90%) | 0.36 |
| BMI (kg/m2) | 21.4 ± 2.9 | 22.0 ± 3.5 | 0.87 |
| BMD (T-score) | −1.0 ± 0.8 | −1.4 ± 0.9 | 0.08 |
| Frailty (mFI-11) | 0 | 0.12 ± 0.09 | <0.01 * |
| Schwab-SRS type (T:D:L:N) | 0:9:16:14 (0%:23%:41%:36%) | 1:5:19:14 (3%:13%:49%:36%) | 0.53 |
| Level fused | 9.8 ± 3.6 | 9.9 ± 2.2 | 0.89 |
| PSO | 2 (5%) | 4 (19%) | 0.68 |
| LLIF | 12 (31%) | 15 (39%) | 0.64 |
| LIV (pelvis) | 17 (44%) | 22 (56%) | 0.37 |
| TOS (min.) | 260 ± 68 | 275 ± 64 | 0.50 |
| EBL (L) | 0.8 ± 0.8 | 0.6 ± 0.3 | 0.20 |
| Baseline spinal alignment | |||
| Cobb angle (°) | 41 ±13 | 39 ± 11 | 0.79 |
| C7SVA (mm) | 84 ± 73 | 75 ± 55 | 0.68 |
| PT (°) | 33 ± 13 | 34 ± 9 | 0.74 |
| PI-LL (°) | 37 ± 21 | 41 ± 20 | 0.81 |
| Biomarkers | SAE− | SAE+ | p Value |
|---|---|---|---|
| WBC (103/uL) | 5.3 ± 1.6 | 5.3 ± 1.8 | 0.94 |
| Hb (g/dL) | 12.6 ± 1.2 | 12.0 ± 1.3 | 0.52 |
| PLT (104/uL) | 22.8 ± 7.2 | 24.4 ± 10.2 | 0.49 |
| TLC (102/uL) | 29.9 ± 8.8 | 30.0 ± 8.8 | 0.96 |
| TP (g/dL) | 6.7 ± 0.4 | 6.7 ± 0.6 | 0.84 |
| ALB (g/dL) | 4.0 ± 0.2 | 3.6 ± 0.6 | 0.12 |
| BUN (mg/dL) | 16.5 ± 4.4 | 16.4 ± 4.5 | 0.96 |
| Cr (mg/dL) | 0.67 ± 0.18 | 0.78 ± 0.23 | 0.05 * |
| CRP (mg/dL) | 0.06 ± 0.12 | 0.07 ± 0.08 | 0.86 |
| AST (IU/L) | 22.3 ± 8.6 | 23.5 ± 4.8 | 0.83 |
| ALT (IU/L) | 17.5 ± 9.2 | 17.5 ± 6.9 | 0.99 |
| PT-INR (%) | 1.0 ± 0.1 | 0.9 ± 0.1 | 0.58 |
| aPTT (s) | 27.6 ± 3.2 | 27.4 ± 3.2 | 0.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabata, T.; Yagi, M.; Suzuki, S.; Takahashi, Y.; Ozaki, M.; Tsuji, O.; Nagoshi, N.; Matsumoto, M.; Nakamura, M.; Watanabe, K. Dysregulation of Inflammatory Pathways in Adult Spinal Deformity Patients with Frailty. J. Clin. Med. 2024, 13, 2294. https://doi.org/10.3390/jcm13082294
Tabata T, Yagi M, Suzuki S, Takahashi Y, Ozaki M, Tsuji O, Nagoshi N, Matsumoto M, Nakamura M, Watanabe K. Dysregulation of Inflammatory Pathways in Adult Spinal Deformity Patients with Frailty. Journal of Clinical Medicine. 2024; 13(8):2294. https://doi.org/10.3390/jcm13082294
Chicago/Turabian StyleTabata, Tomohisa, Mitsuru Yagi, Satoshi Suzuki, Yohei Takahashi, Masahiro Ozaki, Osahiko Tsuji, Narihito Nagoshi, Morio Matsumoto, Masaya Nakamura, and Kota Watanabe. 2024. "Dysregulation of Inflammatory Pathways in Adult Spinal Deformity Patients with Frailty" Journal of Clinical Medicine 13, no. 8: 2294. https://doi.org/10.3390/jcm13082294
APA StyleTabata, T., Yagi, M., Suzuki, S., Takahashi, Y., Ozaki, M., Tsuji, O., Nagoshi, N., Matsumoto, M., Nakamura, M., & Watanabe, K. (2024). Dysregulation of Inflammatory Pathways in Adult Spinal Deformity Patients with Frailty. Journal of Clinical Medicine, 13(8), 2294. https://doi.org/10.3390/jcm13082294