

Impact of Body Mass Index on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Searches
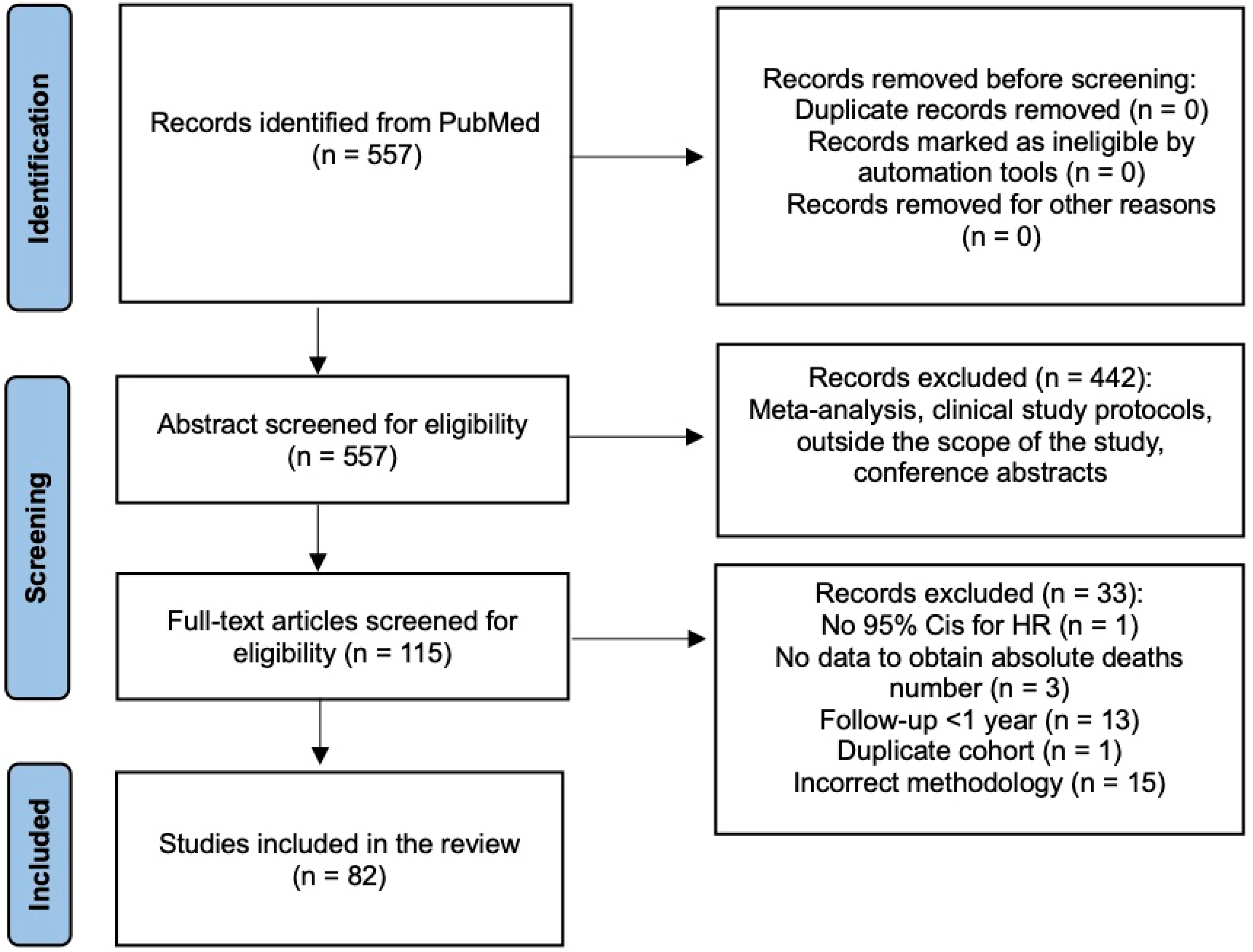
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 19 March 2024).
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef] [PubMed]
- Landsberg, L.; Aronne, L.J.; Beilin, L.J.; Burke, V.; Igel, L.I.; Lloyd-Jones, D.; Sowers, J. Obesity-related hypertension: Pathogenesis, cardiovascular risk and treatment: A position paper of The Obesity Society and the American Society of Hypertension. J. Clin. Hypertens. 2013, 15, 14–33. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2021, 143, 984–1010. [Google Scholar] [CrossRef] [PubMed]
- Maggio, C.A.; Pi-Sunyer, F.X. Obesity and type 2 diabetes. Endocrinol. Metab. Clin. 2003, 32, 805–822. [Google Scholar] [CrossRef] [PubMed]
- Grewal, G.; Joshi, G.P. Obesity and obstructive sleep apnea in the ambulatory patient. Anesthesiol. Clin. 2019, 37, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism 2019, 92, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Graubard, B.I.; Williamson, D.F.; Gail, M.H. Excess deaths associated with underweight, overweight, and obesity. JAMA 2005, 293, 1861–1867. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, N. Downsizing obesity: On Ancel Keys, the origins of BMI, and the neglect of excess weight as a health hazard in the United States from the 1950s to 1970s. J. Hist. Behav. Sci. 2019, 55, 299–318. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Dos-Santos-Silva, I.; Leon, D.A.; Douglas, I.J.; Smeeth, L. Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3.6 million adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef]
- Rhee, C.M.; Ahmadi, S.F.; Kalantar-Zadeh, K. The dual roles of obesity in chronic kidney disease: A review of the current literature. Curr. Opin Nephrol. Hypertens. 2016, 25, 208–216. [Google Scholar] [CrossRef]
- Jerant, A.; Franks, P. Body mass index, diabetes, hypertension, and short-term mortality: A population-based observational study, 2000–2006. J. Am. Board Fam. Med. 2012, 25, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.; Monjazeb, A.M.; Decock, J. The obesity paradox in cancer, tumor immunology, and immunotherapy: Potential therapeutic implications in triple negative breast cancer. Front. Immunol. 2019, 10, 1940. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.D.; Ejike, C.O.; Wise, R.A.; McCormack, M.C.; Brigham, E.P. Investigation of the obesity paradox in chronic obstructive pulmonary disease, according to smoking status, in the United States. Am. J. Epidemiol. 2019, 188, 1977–1983. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Morales, F.; Montserrat-de la Paz, S.; Leon, M.J.; Rivero-Pino, F. Effects of malnutrition on the immune system and infection and the role of nutritional strategies regarding improvements in children’s health status: A literature review. Nutrients 2023, 16, 1. [Google Scholar] [CrossRef] [PubMed]
- Hong, N.-S.; Kim, K.-S.; Lee, I.-K.; Lind, P.M.; Lind, L.; Jacobs, D.R.; Lee, D.-H. The association between obesity and mortality in the elderly differs by serum concentrations of persistent organic pollutants: A possible explanation for the obesity paradox. Int. J. Obes. 2012, 36, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Lennon, H.; Sperrin, M.; Badrick, E.; Renehan, A.G. The obesity paradox in cancer: A review. Curr. Oncol. Rep. 2016, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Li, R.; Wolk, A.; Khudyakov, P.; Spiegelman, D. Meta-Analysis for Linear and Nonlinear Dose-Response Relations: Examples, an Evaluation of Approximations, and Software. Am. J. Epidemiol. 2012, 175, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Crippa, A.; Orsini, N. Multivariate Dose-Response Meta-Analysis: The dosresmeta R Package. J. Stat. Softw. Code Snippets 2016, 72, 1–15. [Google Scholar]
- Freedman, D.M.; Ron, E.; Ballard-Barbash, R.; Doody, M.M.; Linet, M.S. Body mass index and all-cause mortality in a nationwide US cohort. Int. J. Obes. 2006, 30, 822–829. [Google Scholar] [CrossRef]
- Hjartåker, A.; Adami, H.O.; Lund, E.; Weiderpass, E. Body mass index and mortality in a prospectively studied cohort of Scandinavian women: The women’s lifestyle and health cohort study. Eur. J. Epidemiol. 2005, 20, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Reeder, B.A.; Elliott, S.; Joffres, M.R.; Pahwa, P.; Raine, K.D.; Kirkland, S.A.; Paradis, G. Body mass index and risk of cardiovascular disease, cancer and all-cause mortality. Can. J. Public Health 2012, 103, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Tsai, S.L.; Albu, J.B.; Lin, C.C.; Li, T.C.; Pi-Sunyer, F.X.; Sung, P.K.; Huang, K.C. Body mass index and all-cause mortality in a large Chinese cohort. CMAJ 2011, 183, 329–336. [Google Scholar] [CrossRef]
- Nagai, M.; Kuriyama, S.; Kakizaki, M.; Ohmori-Matsuda, K.; Sugawara, Y.; Sone, T.; Hozawa, A.; Tsuji, I. Effect of age on the association between body mass index and all-cause mortality: The Ohsaki cohort study. J. Epidemiol. 2010, 20, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, T.; Kuriyama, S.; Ohmori-Matsuda, K.; Kikuchi, N.; Nakaya, N.; Tsuji, I. Increase in body mass index category since age 20 years and all-cause mortality: A prospective cohort study (the Ohsaki Study). Int. J. Obes. 2009, 33, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Zahir, S.F.; Griffin, A.; Veerman, J.L.; Magliano, D.J.; Shaw, J.E.; Cao, K.-A.L.; Mehdi, A.M. Exploring the association between BMI and mortality in Australian women and men with and without diabetes: The AusDiab study. Diabetologia 2019, 62, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.S.; Dehlendorff, C.; Petersen, H.G.; Andersen, K.K. Body mass index and poststroke mortality. Neuroepidemiology 2008, 30, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Alhambra, D.; Premaor, M.O.; Avilés, F.F.; Castro, A.S.; Javaid, M.K.; Nogués, X.; Arden, N.K.; Cooper, C.; Compston, J.E.; Diez-Perez, A. Relationship between mortality and BMI after fracture: A population-based study of men and women aged ≥40 years. J. Bone Miner. Res. 2014, 29, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and all-cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ 2016, 353, 2156. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Available online: https://adr.usrds.org/2020/chronic-kidney-disease/1-ckd-in-the-general-population (accessed on 28 March 2024).
- Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 28 March 2024).
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [PubMed]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, M.; Bungum, T.J. Mortality and longevity of elite athletes. J. Sci. Med. Sport 2010, 13, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.A. Long-term body mass index and mortality in the Framingham Heart Study: Unpacking an ounce of prevention. JAMA Netw. Open 2018, 1, 184585. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, C.; Ang, T.F.A.; Au, R. BMI decline patterns and relation to dementia risk across four decades of follow-up in the Framingham Study. Alzheimer’s Dement. 2023, 19, 2520–2527. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 186–275. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
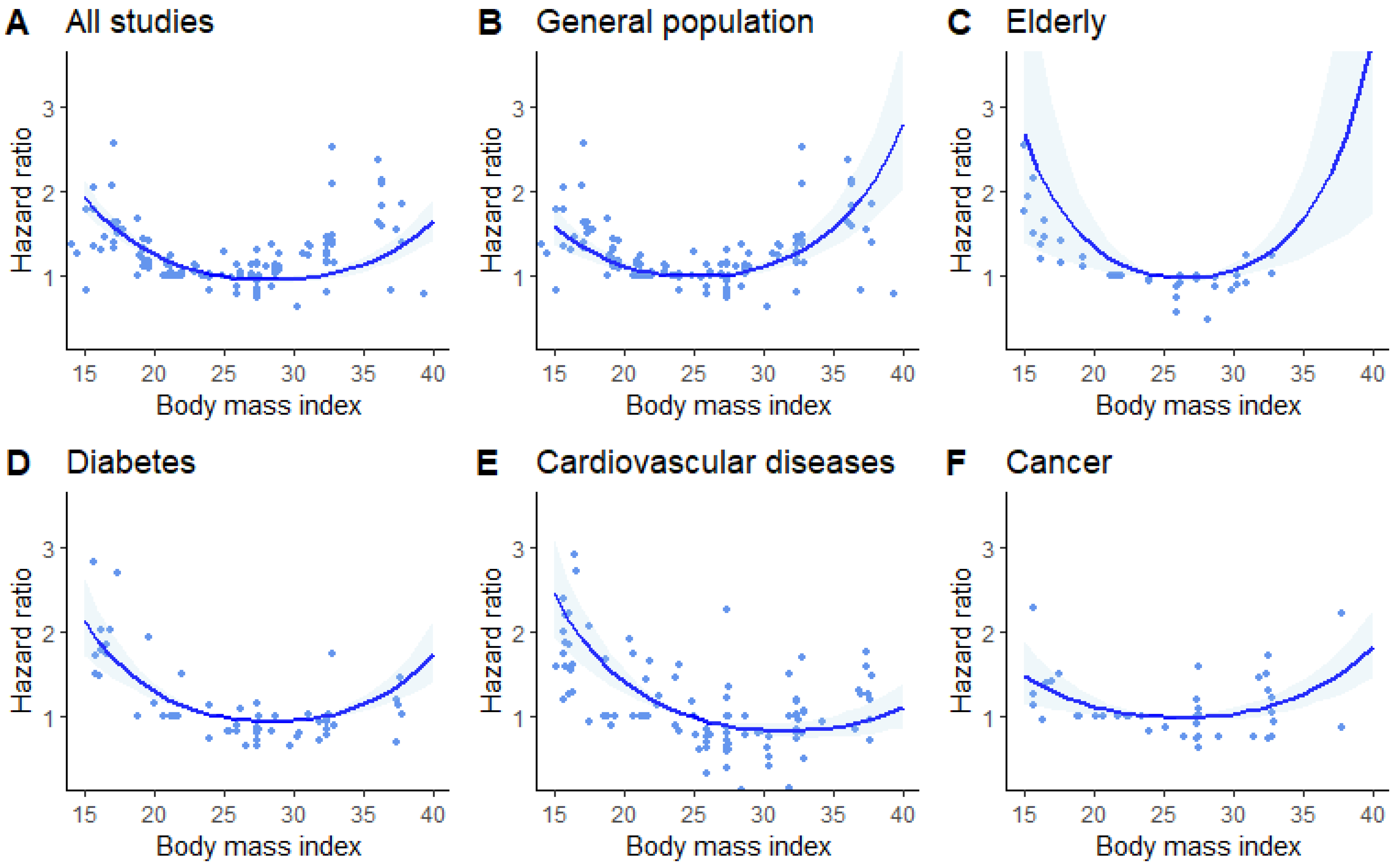
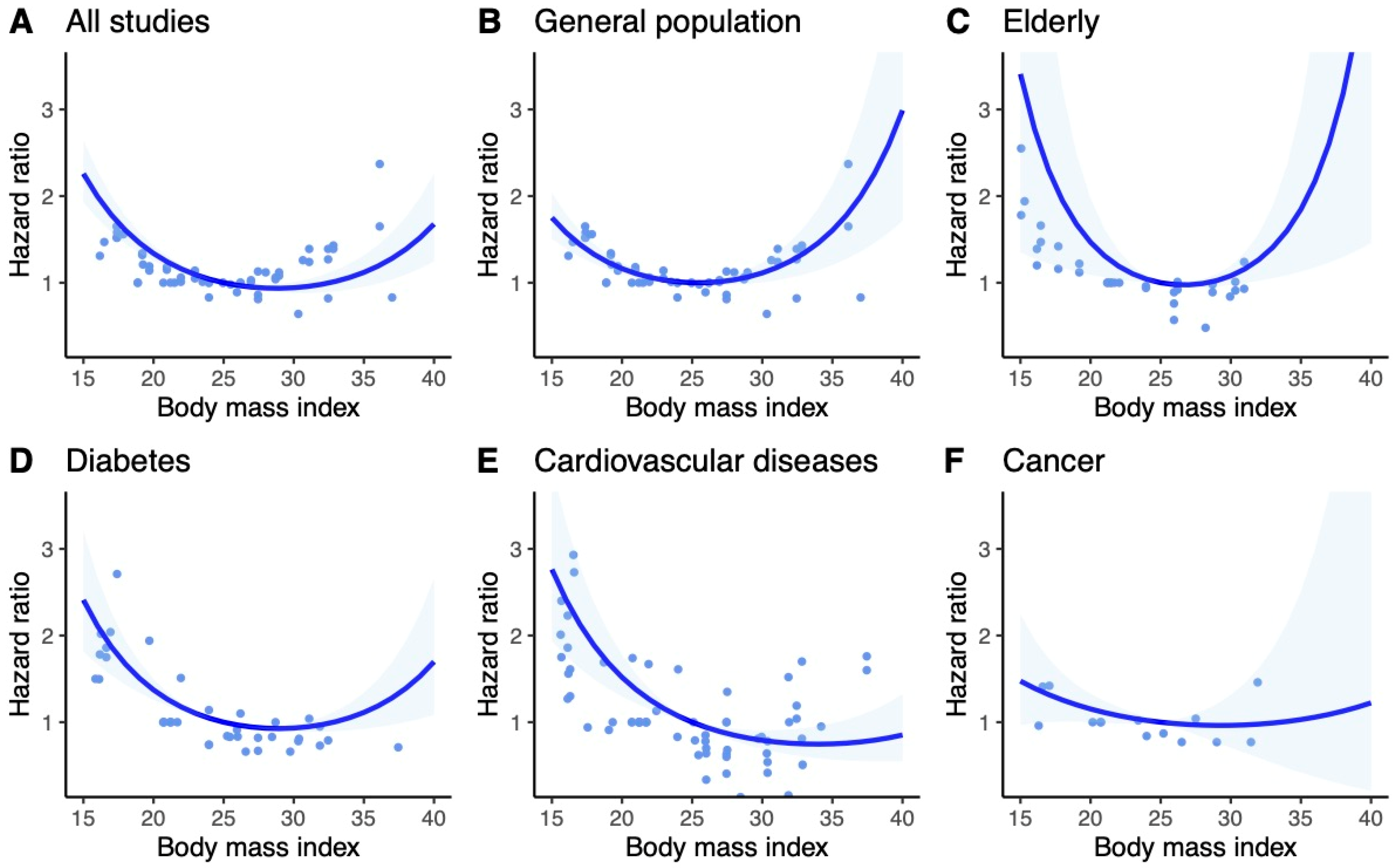
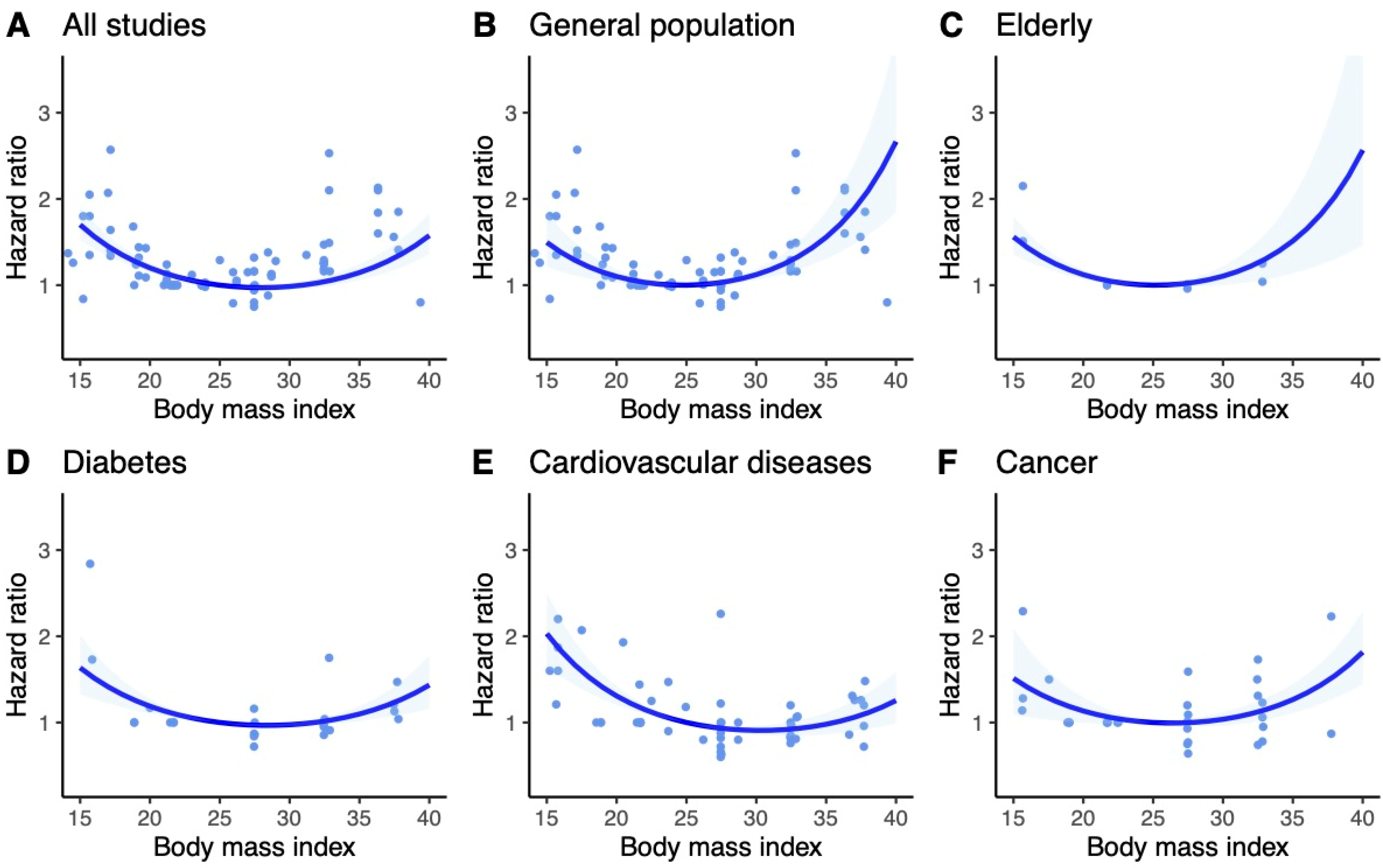
| Subgroup | BMI | HR | 95% CI | I2 | Q-Test | Wald Test |
|---|---|---|---|---|---|---|
| General population | 15 | 1.60 | 1.39–1.84 | 86.1% | p < 0.001 | p < 0.001 |
| 20 | 1.13 | 1.07–1.18 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 1.12 | 1.06–1.18 | ||||
| 35 | 1.58 | 1.35–1.84 | ||||
| 40 | 2.80 | 2.05–3.82 | ||||
| Elderly | 15 | 2.68 | 1.40–5.11 | 81.7% | p < 0.001 | p < 0.001 |
| 20 | 1.36 | 1.10–1.68 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 1.07 | 1.00–1.15 | ||||
| 35 | 1.68 | 1.23–2.29 | ||||
| 40 | 3.84 | 1.74–8.44 | ||||
| Diabetes | 15 | 2.14 | 1.73–2.65 | 84.3% | p < 0.001 | p < 0.001 |
| 20 | 1.31 | 1.22–1.40 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 0.96 | 0.94–0.98 | ||||
| 35 | 1.15 | 1.07–1.24 | ||||
| 40 | 1.74 | 1.41–2.14 | ||||
| CVD | 15 | 2.45 | 1.95–3.09 | 91.5% | p < 0.001 | p < 0.001 |
| 20 | 1.42 | 1.29–1.57 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 0.85 | 0.79–0.92 | ||||
| 35 | 0.89 | 0.77–1.02 | ||||
| 40 | 1.11 | 0.88–1.40 | ||||
| Cancer | 15 | 1.49 | 1.17–1.90 | 73.9% | p < 0.001 | p < 0.001 |
| 20 | 1.13 | 1.02–1.24 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 1.04 | 0.98–1.11 | ||||
| 35 | 1.27 | 1.12–1.44 | ||||
| 40 | 1.83 | 1.46–2.28 | ||||
| Other | 15 | 2.00 | 1.55–2.58 | 82.3% | p < 0.001 | p < 0.001 |
| 20 | 1.31 | 1.19–1.45 | ||||
| 25 | 1.00 | 1.00–1.00 | ||||
| 30 | 0.88 | 0.83–0.94 | ||||
| 35 | 0.90 | 0.81–1.01 | ||||
| 40 | 1.07 | 0.89–1.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, M.M.; Niemczyk, M.; Gołębiewski, S.; Pączek, L. Impact of Body Mass Index on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 2305. https://doi.org/10.3390/jcm13082305
Nowak MM, Niemczyk M, Gołębiewski S, Pączek L. Impact of Body Mass Index on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(8):2305. https://doi.org/10.3390/jcm13082305
Chicago/Turabian StyleNowak, Marcin M., Mariusz Niemczyk, Sławomir Gołębiewski, and Leszek Pączek. 2024. "Impact of Body Mass Index on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 8: 2305. https://doi.org/10.3390/jcm13082305
APA StyleNowak, M. M., Niemczyk, M., Gołębiewski, S., & Pączek, L. (2024). Impact of Body Mass Index on All-Cause Mortality in Adults: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(8), 2305. https://doi.org/10.3390/jcm13082305