

Patient-Reported Outcomes following Tibial Plateau Fractures: Mid- to Short-Term Implications for Knee Function and Activity Level
 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
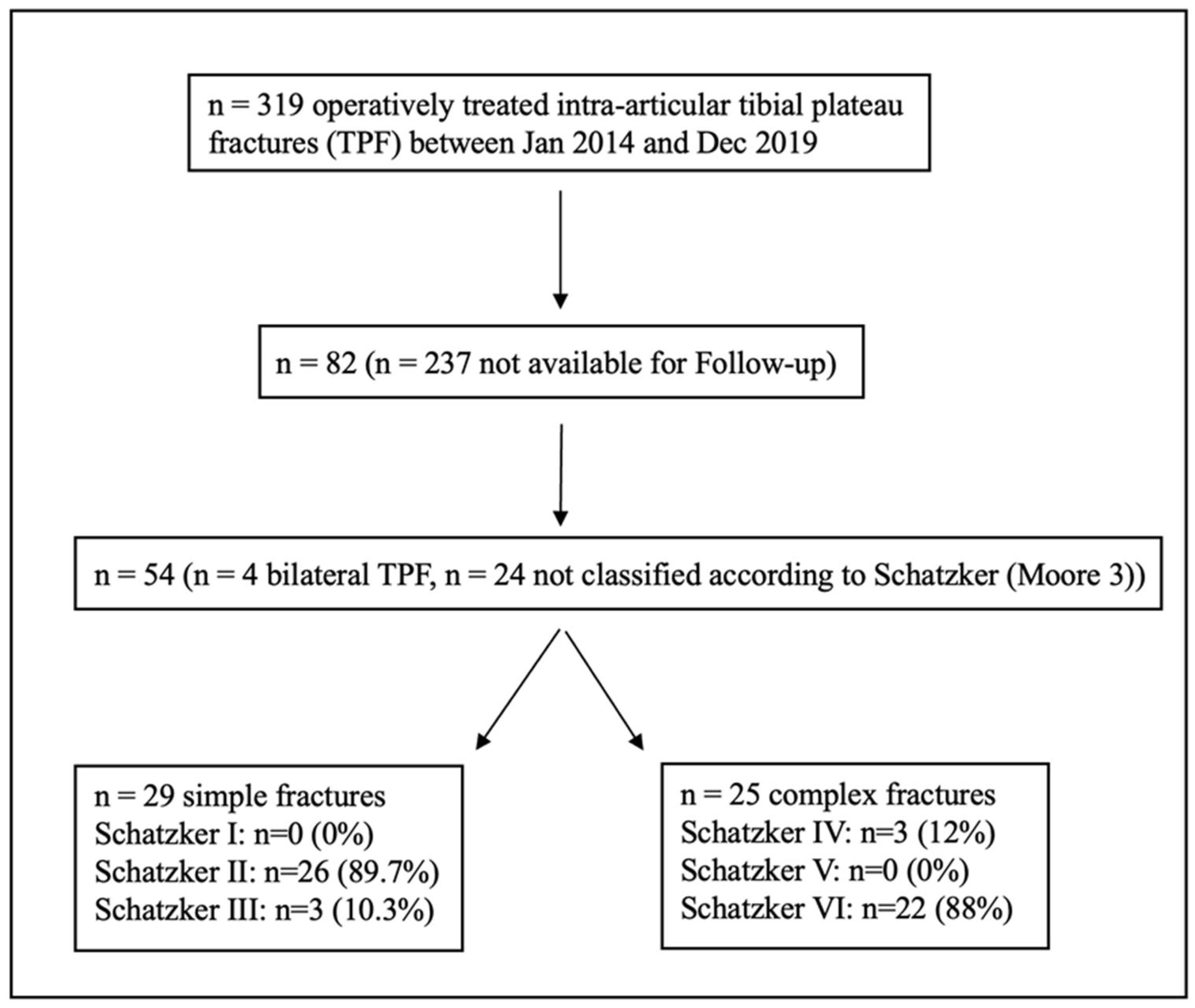
2.1. Patient Selection
2.2. Surgical Treatment
2.2.1. Osteosynthetic Treatment
2.2.2. Bone Grafting
2.2.3. Meniscal and Ligament Repair
2.3. Patient-Reported Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographics
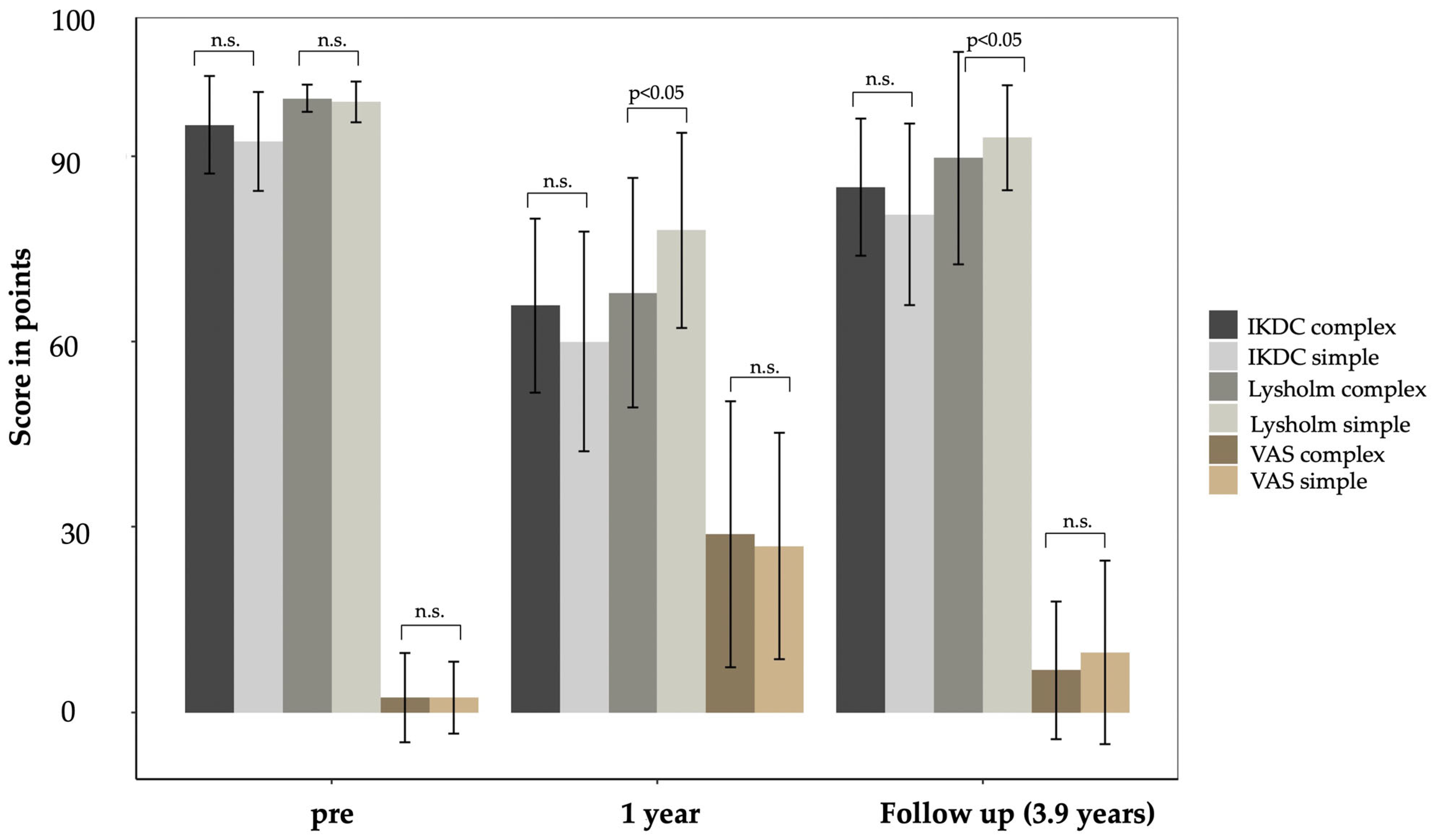
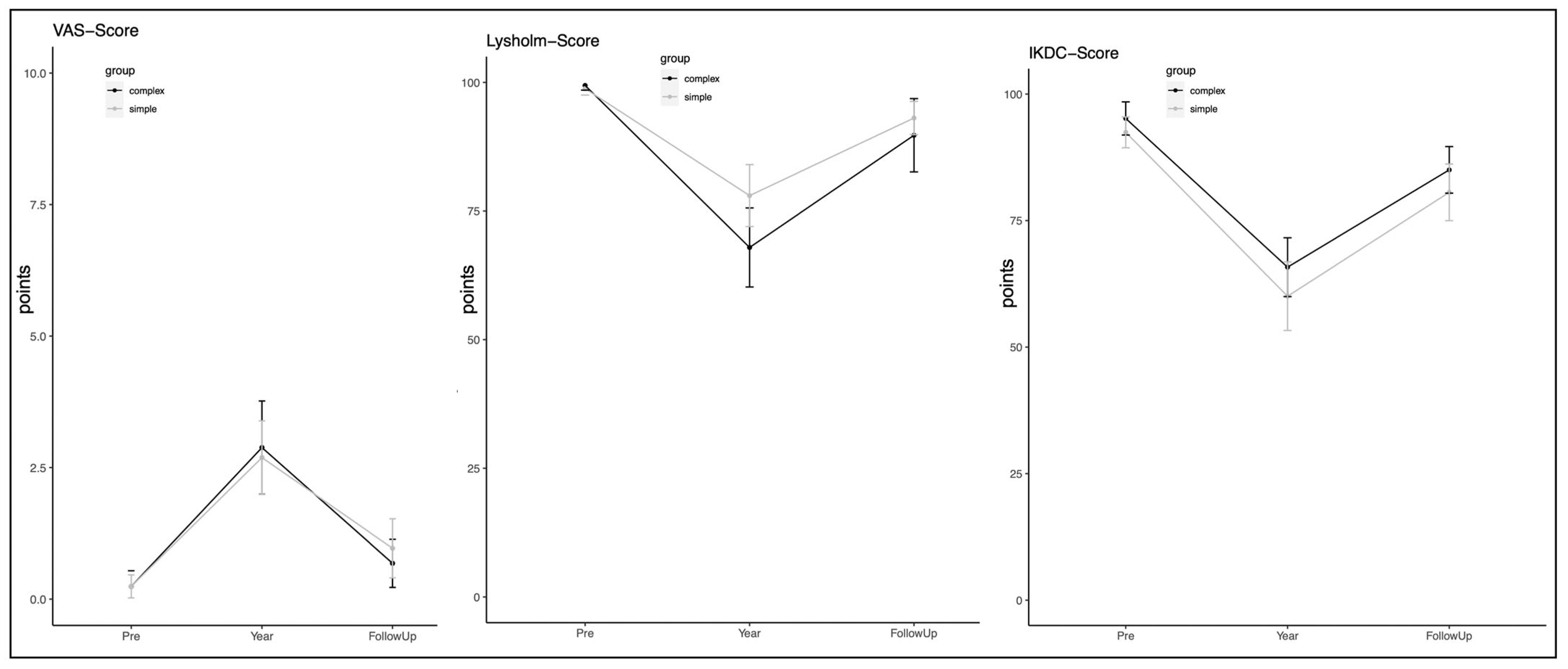
3.2. Outcomes
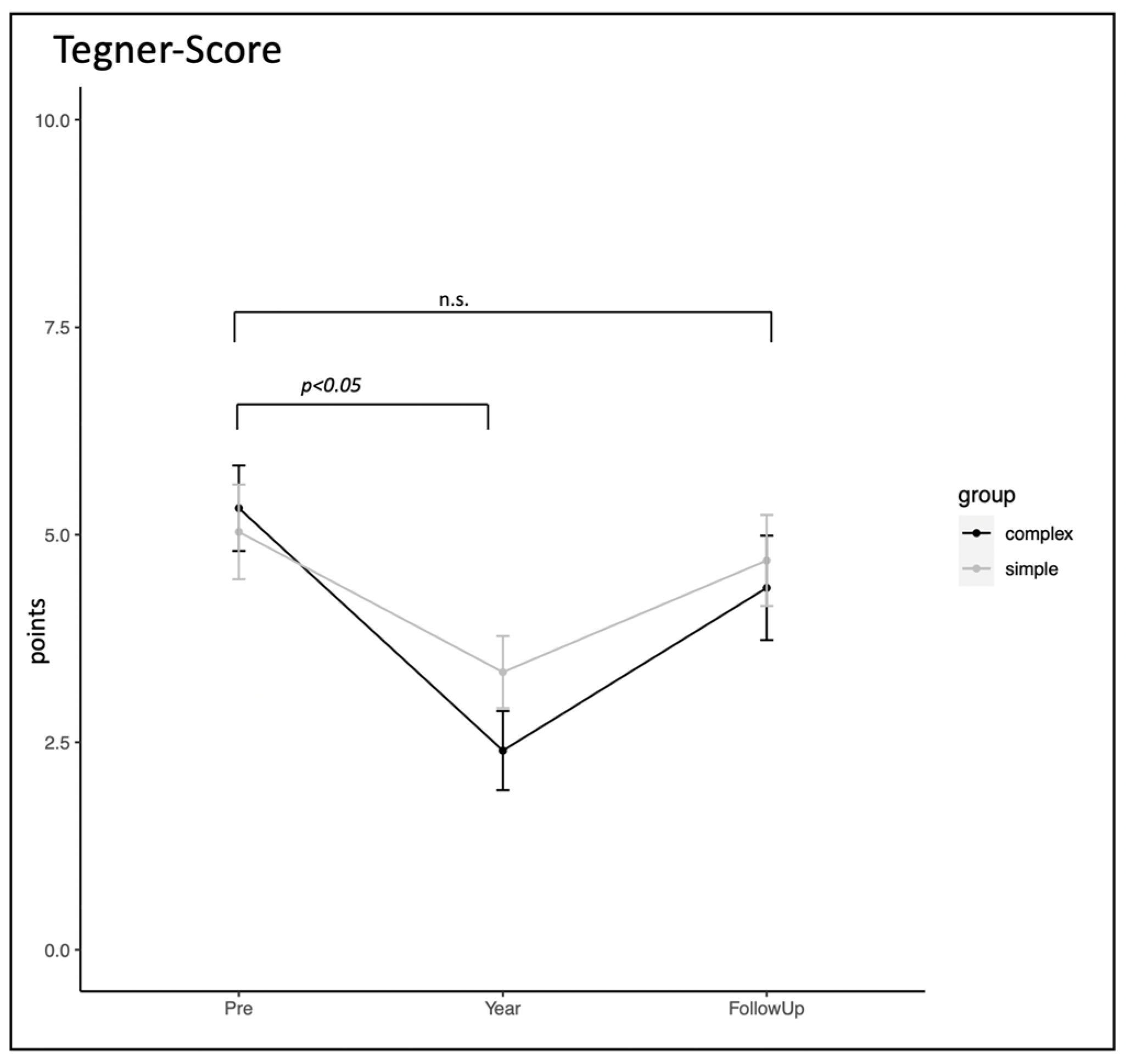
3.3. Return to Sports (RTS)
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keppler, L.; Keppler, A.M.; Ihle, C.; Minzlaff, P.; Fürmetz, J.; Beck, M.; Saier, T. Patients with Complex Proximal Tibial Fractures Overestimate the Prognosis of Their Injury. Eur. J. Trauma Emerg. Surg. 2022, 48, 1479–1486. [Google Scholar] [CrossRef]
- Gill, T.J.; Moezzi, D.M.; Oates, K.M.; Sterett, W.I. Arthroscopic Reduction and Internal Fixation of Tibial Plateau Fractures in Skiing. Clin. Orthop. Relat. Res. 2001, 383, 243–249. [Google Scholar] [CrossRef]
- Rupp, M.; Walter, N.; Pfeifer, C.; Lang, S.; Kerschbaum, M.; Krutsch, W.; Baumann, F.; Alt, V. The Incidence of Fractures among the Adult Population of Germany. Dtsch. Arztebl. Int. 2021, 118, 665–669. [Google Scholar] [CrossRef]
- Bormann, M.; Neidlein, C.; Gassner, C.; Keppler, A.M.; Bogner-Flatz, V.; Ehrnthaller, C.; Prall, W.C.; Böcker, W.; Fürmetz, J. Changing Patterns in the Epidemiology of Tibial Plateau Fractures: A 10-Year Review at a Level-I Trauma Center. Eur. J. Trauma Emerg. Surg. 2023, 49, 401–409. [Google Scholar] [CrossRef]
- Wennergren, D.; Bergdahl, C.; Ekelund, J.; Juto, H.; Sundfeldt, M.; Möller, M. Epidemiology and Incidence of Tibia Fractures in the Swedish Fracture Register. Injury 2018, 49, 2068–2074. [Google Scholar] [CrossRef]
- Lansinger, O.; Bergman, B.; Körner, L.; Andersson, G.B. Tibial Condylar Fractures. A Twenty-Year Follow-Up. J. Bone Jt. Surg. Am. 1986, 68, 13–19. [Google Scholar] [CrossRef]
- Papagelopoulos, P.J.; Partsinevelos, A.A.; Themistocleous, G.S.; Mavrogenis, A.F.; Korres, D.S.; Soucacos, P.N. Complications after Tibia Plateau Fracture Surgery. Injury 2006, 37, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Honkonen, S.E. Degenerative Arthritis after Tibial Plateau Fractures. J. Orthop. Trauma 1995, 9, 273–277. [Google Scholar] [CrossRef]
- Elsoe, R.; Larsen, P.; Nielsen, N.P.H.; Swenne, J.; Rasmussen, S.; Ostgaard, S.E. Population-Based Epidemiology of Tibial Plateau Fractures. Orthopedics 2015, 38, e780–e786. [Google Scholar] [CrossRef] [PubMed]
- Herteleer, M.; Van Brandt, C.; Vandoren, C.; Nijs, S.; Hoekstra, H. Tibial Plateau Fractures in Belgium: Epidemiology, Financial Burden and Costs Curbing Strategies. Eur. J. Trauma Emerg. Surg. 2022, 48, 3643–3650. [Google Scholar] [CrossRef]
- Kugelman, D.N.; Qatu, A.M.; Haglin, J.M.; Konda, S.R.; Egol, K.A. Participation in Recreational Athletics after Operative Fixation of Tibial Plateau Fractures: Predictors and Functional Outcomes of Those Getting Back in the Game. Orthop. J. Sports Med. 2017, 5, 232596711774391. [Google Scholar] [CrossRef]
- Narayan, B.; Harris, C.; Nayagam, S. Treatment of High-Energy Tibial Plateau Fractures. Strateg. Trauma Limb Reconstr. 2006, 1, 18–28. [Google Scholar] [CrossRef]
- Stevens, D.G.; Beharry, R.; McKee, M.D.; Waddell, J.P.; Schemitsch, E.H. The Long-Term Functional Outcome of Operatively Treated Tibial Plateau Fractures. J. Orthop. Trauma 2001, 15, 312–320. [Google Scholar] [CrossRef]
- Bormann, M.; Bitschi, D.; Neidlein, C.; Berthold, D.P.; Jörgens, M.; Pätzold, R.; Watrinet, J.; Böcker, W.; Holzapfel, B.M.; Fürmetz, J. Mismatch between Clinical–Functional and Radiological Outcome in Tibial Plateau Fractures: A Retrospective Study. J. Clin. Med. 2023, 12, 5583. [Google Scholar] [CrossRef]
- Bäumlein, M.; Hanke, A.; Gueorguiev, B.; Nerlich, M.; Liodakis, E.; Perren, T.; Rillmann, P.; Ryf, C.; Loibl, M. Long-Term Outcome after Surgical Treatment of Intra-Articular Tibial Plateau Fractures in Skiers. Arch. Orthop. Trauma Surg. 2019, 139, 951–959. [Google Scholar] [CrossRef]
- Hap, D.X.F.; Kwek, E.B.K. Functional Outcomes after Surgical Treatment of Tibial Plateau Fractures. J. Clin. Orthop. Trauma 2020, 11, S11–S15. [Google Scholar] [CrossRef]
- Jagdev, S.S.; Pathak, S.; Kanani, H.; Salunke, A. Functional Outcome and Incidence of Osteoarthritis in Operated Tibial Plateau Fractures. Arch. Bone Jt. Surg. 2018, 6, 508–516. [Google Scholar]
- Kugelman, D.N.; Qatu, A.M.; Strauss, E.J.; Konda, S.R.; Egol, K.A. Knee Stiffness after Tibial Plateau Fractures: Predictors and Outcomes (OTA-41). J. Orthop. Trauma 2018, 32, e421–e427. [Google Scholar] [CrossRef]
- Rademakers, M.V.; Kerkhoffs, G.M.M.J.; Sierevelt, I.N.; Raaymakers, E.L.F.B.; Marti, R.K. Operative Treatment of 109 Tibial Plateau Fractures: Five- to 27-Year Follow-up Results. J. Orthop. Trauma 2007, 21, 5–10. [Google Scholar] [CrossRef]
- Touliatos, A.S.; Xenakis, T.; Soucacos, P.K.; Soucacos, P.N. Surgical Management of Tibial Plateau Fractures. Acta Orthop. Scand. Suppl. 1997, 275, 92–96. [Google Scholar] [CrossRef]
- Weigel, D.P.; Marsh, J.L. High-energy fractures of the tibial plateau: Knee function after longer follow-up. J. Bone Jt. Surg. -Am. Vol. 2002, 84, 1541–1551. [Google Scholar] [CrossRef]
- Bormann, M.; Neidlein, C.; Keppler, A.M.; Prall, W.C.; Böcker, W.; Fürmetz, J. Einfluss der COVID-19-Pandemie auf die Frakturepidemiologie am Beispiel der Tibiaplateaufraktur. Unfallchirurgie 2023, 126, 967–974. [Google Scholar] [CrossRef]
- Schatzker, J.; McBroom, R.; Bruce, D. The Tibial Plateau Fracture. The Toronto Experience 1968–1975. Clin. Orthop. Relat. Res. 1979, 138, 94–104. [Google Scholar]
- Van Meer, B.L.; Meuffels, D.E.; Vissers, M.M.; Bierma-Zeinstra, S.M.A.; Verhaar, J.A.N.; Terwee, C.B.; Reijman, M. Knee Injury and Osteoarthritis Outcome Score or International Knee Documentation Committee Subjective Knee Form: Which Questionnaire Is Most Useful to Monitor Patients with an Anterior Cruciate Ligament Rupture in the Short Term? Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 701–715. [Google Scholar] [CrossRef]
- Briggs, K.K.; Steadman, J.R.; Hay, C.J.; Hines, S.L. Lysholm Score and Tegner Activity Level in Individuals with Normal Knees. Am. J. Sports Med. 2009, 37, 898–901. [Google Scholar] [CrossRef]
- Manidakis, N.; Dosani, A.; Dimitriou, R.; Stengel, D.; Matthews, S.; Giannoudis, P. Tibial Plateau Fractures: Functional Outcome and Incidence of Osteoarthritis in 125 Cases. Int. Orthop. (SICOT) 2010, 34, 565–570. [Google Scholar] [CrossRef]
- Milenkovic, S.; Mitkovic, M.; Mitkovic, M.; Stojiljkovic, P.; Stojanovic, M. Lateral Tibial Plateau Fractures—Functional Outcomes and Complications after Open Reduction and Internal Fixation. Int. Orthop. (SICOT) 2021, 45, 1071–1076. [Google Scholar] [CrossRef]
- Park, H.-J.; Lee, H.-D.; Cho, J.H. The Efficacy of Meniscal Treatment Associated with Lateral Tibial Plateau Fractures. Knee Surg. Relat. Res. 2017, 29, 137–143. [Google Scholar] [CrossRef]
- Houben, P.F.J.; van der Linden, E.S.; van den Wildenberg, F.A.J.M.; Stapert, J.W.J.L. Functional and Radiological Outcome after Intra-Articular Tibial Plateau Fractures. Injury 1997, 28, 459–462. [Google Scholar] [CrossRef]
- Jansen, H.; Frey, S.P.; Doht, S.; Fehske, K.; Meffert, R.H. Medium-Term Results after Complex Intra-Articular Fractures of the Tibial Plateau. J. Orthop. Sci. 2013, 18, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.M.; Martetschläger, F.; Müller, D.; Braun, K.F.; Ahrens, P.; Siebenlist, S.; Stöckle, U.; Sandmann, G.H. Return to Sports Activity after Tibial Plateau Fractures: 89 Cases with Minimum 24-Month Follow-Up. Am. J. Sports Med. 2012, 40, 2845–2852. [Google Scholar] [CrossRef]
- Loibl, M.; Bäumlein, M.; Massen, F.; Gueorguiev, B.; Glaab, R.; Perren, T.; Rillmann, P.; Ryf, C.; Naal, F.D. Sports Activity after Surgical Treatment of Intra-Articular Tibial Plateau Fractures in Skiers. Am. J. Sports Med. 2013, 41, 1340–1347. [Google Scholar] [CrossRef]
- Krause, M.; Preiss, A.; Müller, G.; Madert, J.; Fehske, K.; Neumann, M.V.; Domnick, C.; Raschke, M.; Südkamp, N.; Frosch, K.-H. Intra-Articular Tibial Plateau Fracture Characteristics According to the “Ten Segment Classification”. Injury 2016, 47, 2551–2557. [Google Scholar] [CrossRef]
- Charalambous, C.; Tryfonidis, M.; Alvi, F.; Moran, M.; Fang, C.; Samaraji, R.; Hirst, P. Inter- and Intra-Observer Variation of the Schatzker and AO/OTA Classifications of Tibial Plateau Fractures and a Proposal of a New Classification System. Ann. R. Coll. Surg. Engl. 2007, 89, 400–404. [Google Scholar] [CrossRef]
- Millar, S.C.; Arnold, J.B.; Thewlis, D.; Fraysse, F.; Solomon, L.B. A Systematic Literature Review of Tibial Plateau Fractures: What Classifications Are Used and How Reliable and Useful Are They? Injury 2018, 49, 473–490. [Google Scholar] [CrossRef]
- Sabatini, L.; Aprato, A.; Camazzola, D.; Bistolfi, A.; Capella, M.; Massè, A. Primary Total Knee Arthroplasty in Tibial Plateau Fractures: Literature Review and Our Institutional Experience. Injury 2023, 54, S15–S23. [Google Scholar] [CrossRef]
- Jensen, D.; Rude, C.; Duus, B.; Bjerg-Nielsen, A. Tibial Plateau Fractures. A Comparison of Conservative and Surgical Treatment. J. Bone Jt. Surg. Br. Vol. 1990, 72-B, 49–52. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Simple Fractures (n = 29) | Complex Fractures (n = 25) | p-Value |
| Age | 49.8 ± 12.5 | 52.5 ± 11.4 | n.s. |
| Female | 58.6% | 60% | n.s. |
| Male | 41.4% | 40% | n.s. |
| Schatzker | |||
| I | n = 0 (0%) | n = 0 (0%) | - |
| II | n = 26 (89.7%) | n = 0 (0%) | - |
| III | n = 3 (10.3%) | n = 0 (0%) | - |
| IV | n = 0 (0%) | n = 3 (12%) | - |
| V | n = 0 (0%) | n = 0 (0%) | - |
| VI | n = 0 (0%) | n = 22 (88%) | - |
| Cause of accident (%) | |||
| Fall | 42.9% | 23.1% | p < 0.05 |
| Traffic | 14.3% | 26.9% | p < 0.05 |
| Ski | 21.4% | 19.2% | n.s. |
| Biking | 10.7% | 26.9% | p < 0.05 |
| Other | 10.7% | 3.8% | p < 0.05 |
| BMI pre-injury | 23.6 ± 3.6 | 24.8 ± 2.6 | n.s. |
| BMI follow-up | 24.7 ± 3.8 | 29 ± 4.5 | n.s. |
| Score | Pre-Injury (Simple) | One Year (Simple) | Follow-Up (Simple) | p-Value |
| VAS | 0.24 ± 0.57 | 2.69 ± 1.83 | 0.96 ± 1.48 | p < 0.05 |
| Lysholm score | 98.79 ± 3.29 | 78 ± 15.81 | 93.06 ± 8.49 | p < 0.05 |
| IKDC score | 92.42 ± 8.01 | 60.04 ± 17.79 | 80.57 ± 14.70 | p < 0.05 |
| Tegner score | 5.03 ± 1.49 | 3.34 ± 1.14 | 4.69 ± 1.44 | n.s. |
| Score | Pre-Injury (Complex) | One Year (Complex) | Follow-Up (Complex) | p-Value |
| VAS | 0.24 ± 0.72 | 2.88 ± 2.15 | 0.68 ± 1.10 | n.s. |
| Lysholm score | 99.40 ± 2.19 | 67.92 ± 18.61 | 89.72 ± 17.25 | n.s. |
| IKDC score | 95.17 ± 7.91 | 65.79 ± 14.12 | 85.01 ± 11.15 | n.s. |
| Tegner score | 5.32 ± 1.25 | 2.4 ± 1.15 | 4.36 ± 1.52 | n.s. |
| Range of Motion | Complex Fractures | Simple Fractures | p-Value |
| Flexion injured | 126 ± 14 | 127 ± 7 | n.s. |
| Flexion healthy (control) | 129 ± 6 | 129 ± 0 | n.s. |
| Extension injured | 2 ± 1 | 1 ± 1 | n.s. |
| Extension healthy (control) | 2 ± 0 | 2 ± 0 | n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neidlein, C.; Watrinet, J.; Pätzold, R.; Berthold, D.P.; Prall, W.C.; Böcker, W.; Holzapfel, B.M.; Fürmetz, J.; Bormann, M. Patient-Reported Outcomes following Tibial Plateau Fractures: Mid- to Short-Term Implications for Knee Function and Activity Level. J. Clin. Med. 2024, 13, 2327. https://doi.org/10.3390/jcm13082327
Neidlein C, Watrinet J, Pätzold R, Berthold DP, Prall WC, Böcker W, Holzapfel BM, Fürmetz J, Bormann M. Patient-Reported Outcomes following Tibial Plateau Fractures: Mid- to Short-Term Implications for Knee Function and Activity Level. Journal of Clinical Medicine. 2024; 13(8):2327. https://doi.org/10.3390/jcm13082327
Chicago/Turabian StyleNeidlein, Claas, Julius Watrinet, Robert Pätzold, Daniel P. Berthold, Wolf Christian Prall, Wolfgang Böcker, Boris Michael Holzapfel, Julian Fürmetz, and Markus Bormann. 2024. "Patient-Reported Outcomes following Tibial Plateau Fractures: Mid- to Short-Term Implications for Knee Function and Activity Level" Journal of Clinical Medicine 13, no. 8: 2327. https://doi.org/10.3390/jcm13082327
APA StyleNeidlein, C., Watrinet, J., Pätzold, R., Berthold, D. P., Prall, W. C., Böcker, W., Holzapfel, B. M., Fürmetz, J., & Bormann, M. (2024). Patient-Reported Outcomes following Tibial Plateau Fractures: Mid- to Short-Term Implications for Knee Function and Activity Level. Journal of Clinical Medicine, 13(8), 2327. https://doi.org/10.3390/jcm13082327