
Impact of Bronchoscopic Lung Volume Reduction with Valves on the Pulmonary Gas Exchange

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection and Valve Implantation
2.2. Clinical and Radiological Data Acquisition
2.3. Selection of the Target Lobe
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Selected Target Lobe Based on HRCT and Perfusion Scan
3.3. Primary Outcome Measures
Pulmonary Gas Exchange
3.4. Secondary Outcome Measures
3.4.1. Target Lobe Volume Reduction
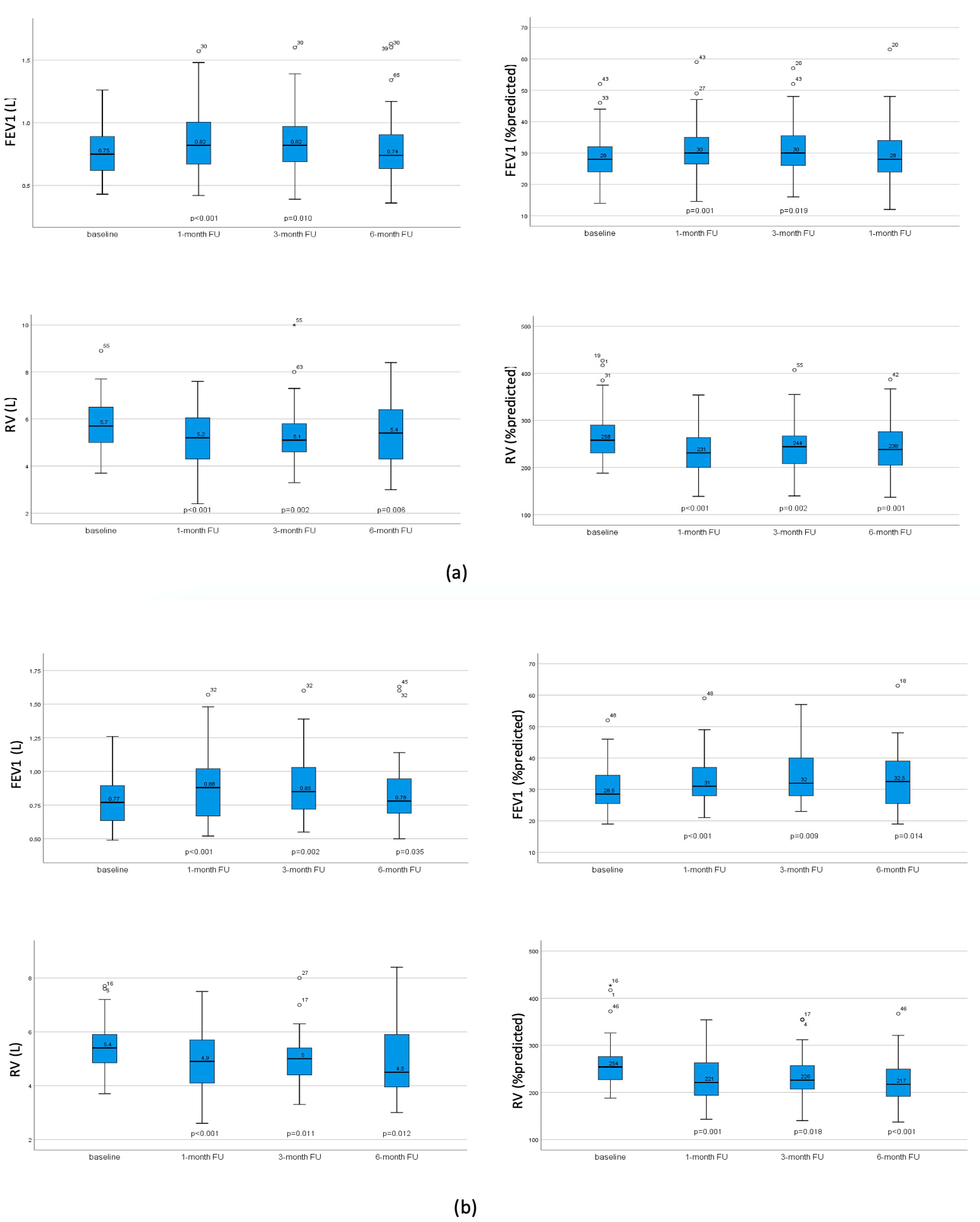
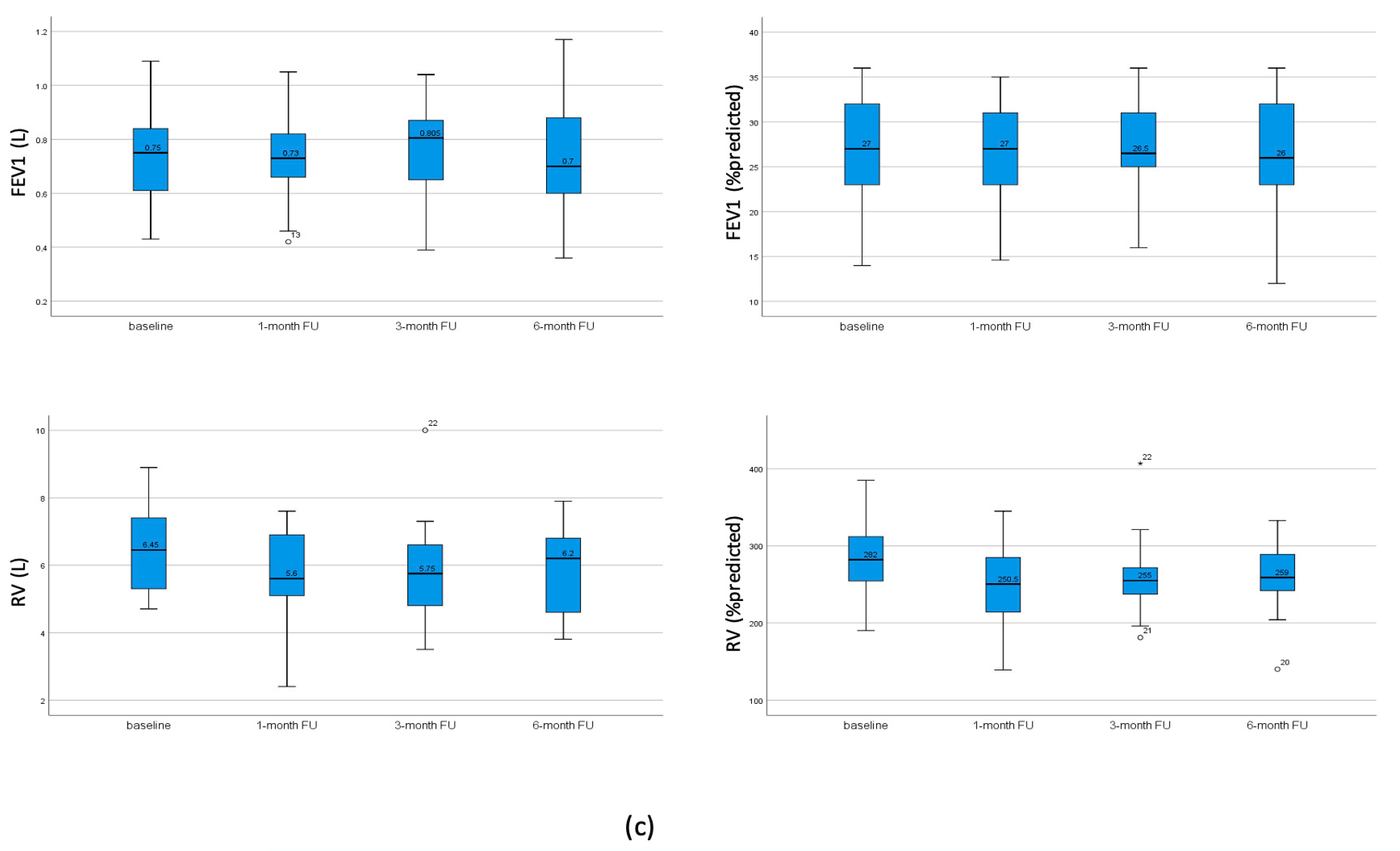
3.4.2. Pulmonary Function Test and Exercise Capacity
3.4.3. Impact of Discrepancy of the Target Lobe in HRCT and Perfusion Scan on Clinical Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Chronic Respiratory Diseases. Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.emro.who.int/health-topics/chronic-obstructive-pulmonary-disease-copd/index.html (accessed on 11 April 2024).
- Janson, C.; Marks, G.; Buist, S.; Gnatiuc, L.; Gislason, T.; McBurnie, M.A.; Nielsen, R.; Studnicka, M.; Toelle, B.; Benediktsdottir, B.; et al. The impact of COPD on health status: Findings from the BOLD study. Eur. Respir. J. 2013, 42, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Criner, G.J.; Sternberg, A.L. National Emphysema Treatment Trial: The major outcomes of lung volume reduction surgery in severe emphysema. Proc. Am. Thorac. Soc. 2008, 5, 393–405. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sciurba, F.C.; Ernst, A.; Herth, F.J.; Strange, C.; Criner, G.J.; Marquette, C.H.; Kovitz, K.L.; Chiacchierini, R.P.; Goldin, J.; McLennan, G.; et al. A randomized study of endobronchial valves for advanced emphysema. N. Engl. J. Med. 2010, 363, 1233–1244. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.L.; Herth, F.J. Current status of bronchoscopic lung volume reduction with endobronchial valves. Thorax 2014, 69, 280. [Google Scholar] [CrossRef] [PubMed]
- Criner, G.J.; Sue, R.; Wright, S.; Dransfield, M.; Rivas-Perez, H.; Wiese, T.; Sciurba, F.C.; Shah, P.L.; Wahidi, M.M.; de Oliveira, H.G.; et al. A Multicenter RCT of Zephyr(R) Endobronchial Valve Treatment in Heterogeneous Emphysema (LIBERATE). Am. J. Respir. Crit. Care Med. 2018, 198, 1151–1164. [Google Scholar] [CrossRef] [PubMed]
- Valipour, A.; Slebos, D.J.; Herth, F.; Darwiche, K.; Wagner, M.; Ficker, J.H.; Petermann, C.; Hubner, R.H.; Stanzel, F.; Eberhardt, R.; et al. Endobronchial Valve Therapy in Patients with Homogeneous Emphysema. Results from the IMPACT Study. Am. J. Respir. Crit. Care Med. 2016, 194, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, R.; Gompelmann, D.; Schuhmann, M.; Reinhardt, H.; Ernst, A.; Heussel, C.P.; Herth, F.J.F. Complete unilateral vs partial bilateral endoscopic lung volume reduction in patients with bilateral lung emphysema. Chest 2012, 142, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Mantri, S.; Macaraeg, C.; Shetty, S.; Aljuri, N.; Freitag, L.; Herth, F.; Eberhardt, R.; Ernst, A. Technical advances: Measurement of collateral flow in the lung with a dedicated endobronchial catheter system. J. Bronchol. Interv. Pulmonol. 2009, 16, 141–144. [Google Scholar] [CrossRef] [PubMed]
- Herth, F.J.; Noppen, M.; Valipour, A.; Leroy, S.; Vergnon, J.M.; Ficker, J.H.; Egan, J.J.; Gasparini, S.; Agusti, C.; Holmes-Higgin, D.; et al. Efficacy predictors of lung volume reduction with Zephyr valves in a European cohort. Eur. Respir. J. 2012, 39, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Herth, F.J.F.; Slebos, D.J.; Criner, G.J.; Valipour, A.; Sciurba, F.; Shah, P.L. Endoscopic Lung Volume Reduction: An Expert Panel Recommendation—Update 2019. Respiration 2019, 97, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Darwiche, K.; Karpf-Wissel, R.; Eisenmann, S.; Aigner, C.; Welter, S.; Zarogoulidis, P.; Hohenforst-Schmidt, W.; Freitag, L.; Oezkan, F. Bronchoscopic Lung Volume Reduction with Endobronchial Valves in Low-FEV1 Patients. Respiration 2016, 92, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.C.; Peters, M.J.; Chen, S.; Emmett, L.; Ing, A.J. Effect of unilateral endobronchial valve insertion on pulmonary ventilation and perfusion: A pilot study. Respirology 2010, 15, 1079–1083. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, C.; Ahmadzadehfar, H.; Essler, M.; Fimmers, R.; Nickenig, G.; Skowasch, D. Volumetric and scintigraphic changes following endoscopic lung volume reduction. Eur. Respir. J. 2015, 45, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, C.; Ahmadzadehfar, H.; Essler, M.; Tuleta, I.; Fimmers, R.; Nickenig, G.; Skowasch, D. Effect of endobronchial valve therapy on pulmonary perfusion and ventilation distribution. PLoS ONE 2015, 10, e0118976. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, C.; Schueler, R.; Hammerstingl, C.; Tuleta, I.; Nickenig, G.; Skowasch, D. Impact of endoscopic lung volume reduction on right ventricular myocardial function. PLoS ONE 2015, 10, e0121377. [Google Scholar] [CrossRef] [PubMed]
- Watz, H.; Waschki, B.; Meyer, T.; Kretschmar, G.; Kirsten, A.; Claussen, M.; Magnussen, H. Decreasing cardiac chamber sizes and associated heart dysfunction in COPD: Role of hyperinflation. Chest 2010, 138, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Zoumot, Z.; LoMauro, A.; Aliverti, A.; Nelson, C.; Ward, S.; Jordan, S.; Polkey, M.I.; Shah, P.L.; Hopkinson, N.S. Lung Volume Reduction in Emphysema Improves Chest Wall Asynchrony. Chest 2015, 148, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, C.; Theilig, D.; Herzog, D.; Poellinger, A.; Doellinger, F.; Schreiter, N.; Schreiter, V.; Schurmann, D.; Temmesfeld-Wollbrueck, B.; Hippenstiel, S.; et al. Lung perfusion and emphysema distribution affect the outcome of endobronchial valve therapy. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1245–1259. [Google Scholar]
- Criner, G.J.; Delage, A.; Voelker, K.; Hogarth, D.K.; Majid, A.; Zgoda, M.; Lazarus, D.R.; Casal, R.; Benzaquen, S.B.; Holladay, R.C.; et al. Improving Lung Function in Severe Heterogenous Emphysema with the Spiration Valve System (EMPROVE). A Multicenter, Open-Label Randomized Controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2019, 200, 1354–1362. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S.V.; Slebos, D.J.; Kirk, A.; Kornaszewska, M.; Carron, K.; Ek, L.; Broman, G.; Hillerdal, G.; Mal, H.; Pison, C.; et al. A Multicenter Randomized Controlled Trial of Zephyr Endobronchial Valve Treatment in Heterogeneous Emphysema (TRANSFORM). Am. J. Respir. Crit. Care Med. 2017, 196, 1535–1543. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | 32 males (41.6%) 45 females (58.4%) |
| Age (years) | 62.36 ± 7.17 |
| BMI (kg/m2) | 22.79 ± 4.0 |
| FEV1 (L) | 0.77 ± 0.2 |
| FEV1 (%predicted) | 28.64 ± 6.6 |
| IVC (L) | 2.3 ± 0.8 |
| IVC (%predicted) | 66.2 ± 16.1 |
| RV (L) | 5.79 ± 1.08 |
| RV (%predicted) | 268.29 ± 53.03 |
| KCO (%predicted) | 32.8 ± 11.9 |
| AaDO2 (mmHg) | 29.09 ± 9.95 |
| Patients on long-term oxygen therapy | 43 (55.8%) |
| 6-MWD (m) | 286.86 ± 77.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Winantea, J.; Stiehl, K.; Karpf-Wissel, R.; Funke, F.; Hautzel, H.; Schwarz, B.; Steveling, H.; Taube, C.; Oezkan, F.; Darwiche, K. Impact of Bronchoscopic Lung Volume Reduction with Valves on the Pulmonary Gas Exchange. J. Clin. Med. 2024, 13, 2354. https://doi.org/10.3390/jcm13082354
Winantea J, Stiehl K, Karpf-Wissel R, Funke F, Hautzel H, Schwarz B, Steveling H, Taube C, Oezkan F, Darwiche K. Impact of Bronchoscopic Lung Volume Reduction with Valves on the Pulmonary Gas Exchange. Journal of Clinical Medicine. 2024; 13(8):2354. https://doi.org/10.3390/jcm13082354
Chicago/Turabian StyleWinantea, Jane, Katharina Stiehl, Ruediger Karpf-Wissel, Faustina Funke, Hubertus Hautzel, Birte Schwarz, Heinz Steveling, Christian Taube, Filiz Oezkan, and Kaid Darwiche. 2024. "Impact of Bronchoscopic Lung Volume Reduction with Valves on the Pulmonary Gas Exchange" Journal of Clinical Medicine 13, no. 8: 2354. https://doi.org/10.3390/jcm13082354
APA StyleWinantea, J., Stiehl, K., Karpf-Wissel, R., Funke, F., Hautzel, H., Schwarz, B., Steveling, H., Taube, C., Oezkan, F., & Darwiche, K. (2024). Impact of Bronchoscopic Lung Volume Reduction with Valves on the Pulmonary Gas Exchange. Journal of Clinical Medicine, 13(8), 2354. https://doi.org/10.3390/jcm13082354