

Fluoroscopy- and Endoscopy-Guided Transoral Sclerotherapy Using Foamed Polidocanol for Oropharyngolaryngeal Venous Malformations in a Hybrid Operation Room: A Case Series

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Hybrid Operation Room and the Endoscopy
2.2. Patients and Treatment Indications
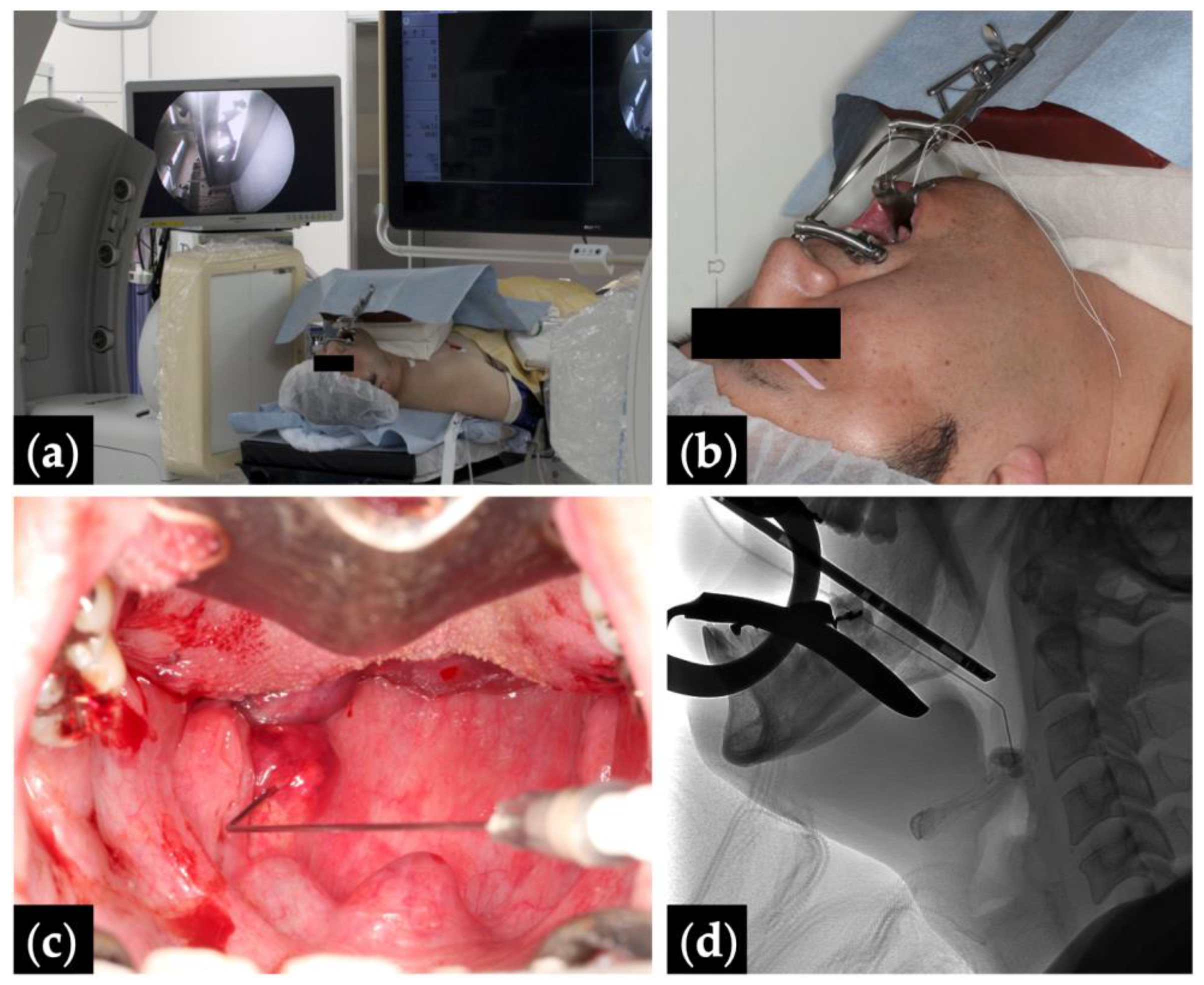
2.3. Sclerotherapy Procedures
2.4. Airway Management after Sclerotherapy
2.5. Evaluation of Outcomes
3. Results
3.1. Patients’ Characteristics
3.2. Treatment Outcomes
4. Discussion



5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CT | computed tomography |
| DSA | digital subtraction angiography |
| MRI | magnetic resonance imaging |
| OR | operation room |
| VM | venous malformation |
| WI | weighted imaging |
References
- Iihara, K.; Satow, T.; Matsushige, T.; Kataoka, H.; Nakajima, N.; Fukuda, K.; Isozaki, M.; Maruyama, D.; Nakae, T.; Hashimoto, N. Hybrid operating room for the treatment of complex neurovascular and brachiocephalic lesions. J. Stroke Cerebrovasc. Dis. 2013, 22, e277–e285. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, T.; Davidson, M.J. Use of the hybrid operating room in cardiovascular medicine. Circulation 2014, 130, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Schuetze, K.; Rau, B.; Dehner, C.; Schultheiss, M.; Richter, P.; Cintean, R.; Gebhard, F.; Eickhoff, A. Spine surgery in a state-of-the-art hybrid operating room: An experience of 1745 implanted pedicle screws in the thoracolumbar spine. J. Robot. Surg. 2023, 17, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Berenguer, B.; Burrows, P.E.; Zurakowski, D.; Mulliken, J.B. Sclerotherapy of craniofacial venous malformations: Complications and results. Plast. Reconstr. Surg. 1999, 104, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, A.; Hatsushika, K.; Kanemaru, S.; Moriyama, M.; Kase, Y.; Masuyama, K. Five adult laryngeal venous malformation cases treated effectively with sclerotherapy. Laryngoscope 2013, 123, 2766–2769. [Google Scholar] [CrossRef] [PubMed]
- Bourgouin, P.; Thomas-Chausse, F.; Gilbert, P.; Giroux, M.F.; Perigny, S.; Guertin, L.; Dubois, J.; Soulez, G. Effectiveness and safety of sclerotherapy for treatment of low-flow vascular malformations of the oropharyngeal region. J. Vasc. Interv. Radiol. 2018, 29, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Stimpson, P.; Hewitt, R.; Barnacle, A.; Roebuck, D.J.; Hartley, B. Sodium tetradecyl sulphate sclerotherapy for treating venous malformations of the oral and pharyngeal regions in children. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 569–573. [Google Scholar] [CrossRef]
- Oomen, K.P.; Paramasivam, S.; Waner, M.; Niimi, Y.; Fifi, J.T.; Berenstein, A.; Teresa, M.O. Endoscopic transmucosal direct puncture sclerotherapy for management of airway vascular malformations. Laryngoscope 2016, 126, 205–211. [Google Scholar] [CrossRef]
- Azene, E.; Mitchell, S.; Radvany, M.; Agrawal, N.; Eisele, D.; Weiss, C. Foamed bleomycin sclerosis of airway venous malformations: The role of interspecialty collaboration. Laryngoscope 2016, 126, 2726–2732. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.S.; Hoffer, F.A.; Barnes, P.D.; Mulliken, J.B. Biological classification of soft-tissue vascular anomalies: MR correlation. AJR Am. J. Roentgenol. 1991, 157, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Legiehn, G.M.; Heran, M.K. Venous malformations: Classification, development, diagnosis, and interventional radiologic management. Radiol. Clin. N. Am. 2008, 46, 545–597, vi. [Google Scholar] [CrossRef] [PubMed]
- Arnold, R.; Chaudry, G. Diagnostic imaging of vascular anomalies. Clin. Plast. Surg. 2011, 38, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Ameer, F.; Singh, A.K.; Kumar, S. The story of mouth gags. J. Cleft Lip Palate Craniofacial Anom. 2014, 1, 70–77. [Google Scholar] [CrossRef]
- Tessari, L.; Cavezzi, A.; Frullini, A. Preliminary experience with a new sclerosing foam in the treatment of varicose veins. Dermatol. Surg. 2001, 27, 58–60. [Google Scholar] [PubMed]
- Ishikawa, K.; Sasaki, S.; Furukawa, H.; Nagao, M.; Iwasaki, D.; Saito, N.; Yamamoto, Y. Preliminary experience with intraoperative near-infrared fluorescence imaging in percutaneous sclerotherapy of soft-tissue venous malformations. Dermatol. Surg. 2013, 39, 907–912. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, K.; Sasaki, S.; Furukawa, H.; Maeda, T.; Miura, T.; Sasaki, Y.; Yamamoto, Y.; Funayama, E. Effectiveness and safety of percutaneous sclerotherapy using absolute ethanol and/or polidocanol for maxillofacial venous malformations involving the masticatory muscles: A case series. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2023, 135, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Rabe, E.; Pannier, F. Sclerotherapy of varicose veins with polidocanol based on the guidelines of the German Society of Phlebology. Dermatol. Surg. 2010, 36 (Suppl. S2), 968–975. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Lin, X.; Chen, H.; Li, W.; Hu, X.; Ma, G.; Zhu, L.; Sun, M.; Yang, C.; Wang, W. Craniofacial venous malformations: Magnetic resonance imaging features that predict treatment outcome. J. Oral Maxillofac. Surg. 2009, 67, 2388–2396. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Hoogstraten, B.; Staquet, M.; Winkler, A. Reporting results of cancer treatment. Cancer 1981, 47, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Iwashina, Y.; Ozaki, M.; Wong, M.; Ihara, A.; Fujiki, M.; Takushima, A.; Harii, K. Sclerotherapy for venous malformations of the pharynx or the tongue base without tracheostomy: Treatment protocol with intubation and outcomes. J. Craniofac. Surg. 2020, 31, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Mulliken, J.B.; Glowacki, J. Hemangiomas and vascular malformations in infants and children: A classification based on endothelial characteristics. Plast. Reconstr. Surg. 1982, 69, 412–422. [Google Scholar] [CrossRef] [PubMed]
- ISSVA Classification of Vascular Anomalies ©2018 International Society for the Study of Vascular Anomalies. Available online: https://www.issva.org/classification (accessed on 29 January 2024).
- Rikihisa, N.; Akita, S.; Osuga, K.; Mimura, H.; Yuzuriha, S.; Sasaki, S. Evaluation of pain incidence due to venous malformation based on data from 85 institutions in Japan. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, V.F.; Masthoff, M.; Czihal, M.; Cucuruz, B.; Haberle, B.; Brill, R.; Wohlgemuth, W.A.; Wildgruber, M. Imaging of peripheral vascular malformations—Current concepts and future perspectives. Mol. Cell Pediatr. 2021, 8, 19. [Google Scholar] [CrossRef]
- Johnson, P.L.; Eckard, D.A.; Brecheisen, M.A.; Girod, D.A.; Tsue, T.T. Percutaneous ethanol sclerotherapy of venous malformations of the tongue. AJNR Am. J. Neuroradiol. 2002, 23, 779–782. [Google Scholar] [PubMed]
- Araslanova, R.; Min-Jung, O.T.; Waner, M. Endoscopic multimodal approach to the treatment of airway venous malformations. Laryngoscope 2021, 131, E521–E524. [Google Scholar] [CrossRef] [PubMed]
- Higgins, L.J.; Koshy, J.; Mitchell, S.E.; Weiss, C.R.; Carson, K.A.; Huisman, T.A.; Tekes, A. Time-resolved contrast-enhanced MRA (TWIST) with gadofosveset trisodium in the classification of soft-tissue vascular anomalies in the head and neck in children following updated 2014 ISSVA classification: First report on systematic evaluation of MRI and TWIST in a cohort of 47 children. Clin. Radiol. 2016, 71, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Moukaddam, H.; Pollak, J.; Haims, A.H. MRI characteristics and classification of peripheral vascular malformations and tumors. Skelet. Radiol. 2009, 38, 535–547. [Google Scholar] [CrossRef] [PubMed]
- van Rijswijk, C.S.; van der Linden, E.; van der Woude, H.J.; van Baalen, J.M.; Bloem, J.L. Value of dynamic contrast-enhanced MR imaging in diagnosing and classifying peripheral vascular malformations. AJR Am. J. Roentgenol. 2002, 178, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Hein, K.D.; Mulliken, J.B.; Kozakewich, H.P.; Upton, J.; Burrows, P.E. Venous malformations of skeletal muscle. Plast. Reconstr. Surg. 2002, 110, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Lamba, S.; Keshava, S.K.N.; Moses, V.; Surendrababu, N.; Gupta, A.K. Ethanol sclerotherapy for treatment of venous malformations of face and neck— a single centre experience. Eur. J. Plast. Surg. 2012, 35, 345–350. [Google Scholar] [CrossRef]
- Blaise, S.; Charavin-Cocuzza, M.; Riom, H.; Brix, M.; Seinturier, C.; Diamand, J.M.; Gachet, G.; Carpentier, P.H. Treatment of low-flow vascular malformations by ultrasound-guided sclerotherapy with polidocanol foam: 24 cases and literature review. Eur. J. Vasc. Endovasc. Surg. 2011, 41, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.D.; McTaggart, R.A.; Choudhri, O.A.; Marcellus, M.L.; Do, H.M. Percutaneous sclerotherapy with ethanolamine oleate for venous malformations of the head and neck. J. Neurointerv. Surg. 2014, 6, 695–698. [Google Scholar] [CrossRef] [PubMed]
- Spence, J.; Krings, T.; TerBrugge, K.G.; Agid, R. Percutaneous treatment of facial venous malformations: A matched comparison of alcohol and bleomycin sclerotherapy. Head Neck 2011, 33, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Horbach, S.E.; Lokhorst, M.M.; Saeed, P.; de Gouyon Matignon de Pontouraude, C.M.; Rothova, A.; van der Horst, C.M. Sclerotherapy for low-flow vascular malformations of the head and neck: A systematic review of sclerosing agents. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 295–304. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Yang, B.; Nie, Q.Q.; Zhang, J.B.; Chen, J.; Liu, P.; Fan, X.Q.; Ye, Z.D. Comparison of polidocanol foam versus bleomycin polidocanol foam for treatment of venous malformations. J. Vasc. Surg. Venous Lymphat. Disord. 2023, 11, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, H.; Sasaki, S.; Oyama, A.; Funayama, E.; Hayashi, T.; Saito, N.; Nagao, M.; Mol, W.; Yamamoto, Y. Efficacy of percutaneous ethanol sclerotherapy for venous malformation in lower extremities: A retrospective review of 21 cases. Eur. J. Plast. Surg. 2013, 36, 105–110. [Google Scholar] [CrossRef]
- Ishikawa, K.; Sasaki, S.; Furukawa, H.; Nagao, M.; Iwasaki, D.; Fujita, M.; Saito, N.; Oyama, A.; Yamamoto, Y. A case of combined soft tissue and intraosseous venous malformation of the thumb treated with sclerotherapy using a bone marrow aspiration needle. Cas. Rep. Plast. Surg. Hand Surg. 2015, 2, 37–39. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age, Years | Distribution of Lesions | Symptoms | Tracheostomy (Duration, Months) |
|---|---|---|---|---|---|
| 1 | F | 67 | Extensive | Swallowing difficulties | Temporary * (55) |
| 2 | M | 71 | Extensive | − | Temporary (89) |
| 3 | F | 59 | Extensive | – | – |
| 4 | M | 11 | Extensive | Snoring | – |
| 5 | F | 17 | Extensive | – | – |
| 6 | F | 59 | Extensive | Breathing difficulties | Temporary * (2) |
| 7 | M | 35 | Extensive | Breathing difficulties, sleep apnea | Permanent |
| 8 | M | 41 | Extensive | Breathing difficulties | Permanent |
| 9 | M | 8 | Extensive | – | – |
| 10 | M | 43 | Limited | – | Temporary * (9) |
| 11 | F | 4 | Limited | – | – |
| 12 | M | 11 | Limited | – | Temporary * (28) |
| 13 | M | 16 | Limited | – | – |
| 14 | F | 4 | Limited | Snoring | – |
| Patient | Treated Regions | Number of Sclerotherapy Treatments * | Follow-Up, Months | Treatment Outcomes | Complications |
|---|---|---|---|---|---|
| 1 | Pharynx | 9 | 92 | Excellent | – |
| 2 | Soft palate, pharynx | 7 | 83 | Good † | – |
| 3 | Soft palate, pharynx | 2 | 141 | Good | – |
| 4 | Soft palate | 2 | 6 | Good † | – |
| 5 | Pharynx | 1 | 50 | Good † | – |
| 6 | Tongue | 1 | 36 | Good | Bleeding |
| 7 | Soft palate, tongue | 5 | 138 | Fair † | – |
| 8 | Soft palate | 2 | 130 | Fair † | – |
| 9 | Soft palate, pharynx | 6 | 138 | Fair † | – |
| 10 | Pharynx | 3 | 43 | Excellent | – |
| 11 | Soft palate, tongue | 3 | 79 | Good † | – |
| 12 | Tongue, epiglottis | 5 | 29 | Good | – |
| 13 | Pharynx | 1 | 97 | Fair | – |
| 14 | Soft palate | 1 | 16 | Fair † | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishikawa, K.; Maeda, T.; Funayama, E.; Murao, N.; Miura, T.; Sasaki, Y.; Seo, D.; Mitamura, S.; Oide, S.; Yamamoto, Y.; et al. Fluoroscopy- and Endoscopy-Guided Transoral Sclerotherapy Using Foamed Polidocanol for Oropharyngolaryngeal Venous Malformations in a Hybrid Operation Room: A Case Series. J. Clin. Med. 2024, 13, 2369. https://doi.org/10.3390/jcm13082369
Ishikawa K, Maeda T, Funayama E, Murao N, Miura T, Sasaki Y, Seo D, Mitamura S, Oide S, Yamamoto Y, et al. Fluoroscopy- and Endoscopy-Guided Transoral Sclerotherapy Using Foamed Polidocanol for Oropharyngolaryngeal Venous Malformations in a Hybrid Operation Room: A Case Series. Journal of Clinical Medicine. 2024; 13(8):2369. https://doi.org/10.3390/jcm13082369
Chicago/Turabian StyleIshikawa, Kosuke, Taku Maeda, Emi Funayama, Naoki Murao, Takahiro Miura, Yuki Sasaki, Dongkyung Seo, Shintaro Mitamura, Shunichi Oide, Yuhei Yamamoto, and et al. 2024. "Fluoroscopy- and Endoscopy-Guided Transoral Sclerotherapy Using Foamed Polidocanol for Oropharyngolaryngeal Venous Malformations in a Hybrid Operation Room: A Case Series" Journal of Clinical Medicine 13, no. 8: 2369. https://doi.org/10.3390/jcm13082369
APA StyleIshikawa, K., Maeda, T., Funayama, E., Murao, N., Miura, T., Sasaki, Y., Seo, D., Mitamura, S., Oide, S., Yamamoto, Y., & Sasaki, S. (2024). Fluoroscopy- and Endoscopy-Guided Transoral Sclerotherapy Using Foamed Polidocanol for Oropharyngolaryngeal Venous Malformations in a Hybrid Operation Room: A Case Series. Journal of Clinical Medicine, 13(8), 2369. https://doi.org/10.3390/jcm13082369