

The Influence of Inset and Shaping of Abdominal-Based Free Flap Breast Reconstruction on Patient-Reported Aesthetic Outcome Scores—A Systematic Review


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Data Extraction
2.3. Assessment of Risk of Bias and Quality of Evidence of the Included Studies
2.4. Statistical Analysis
2.5. Graphical Illustration
3. Results
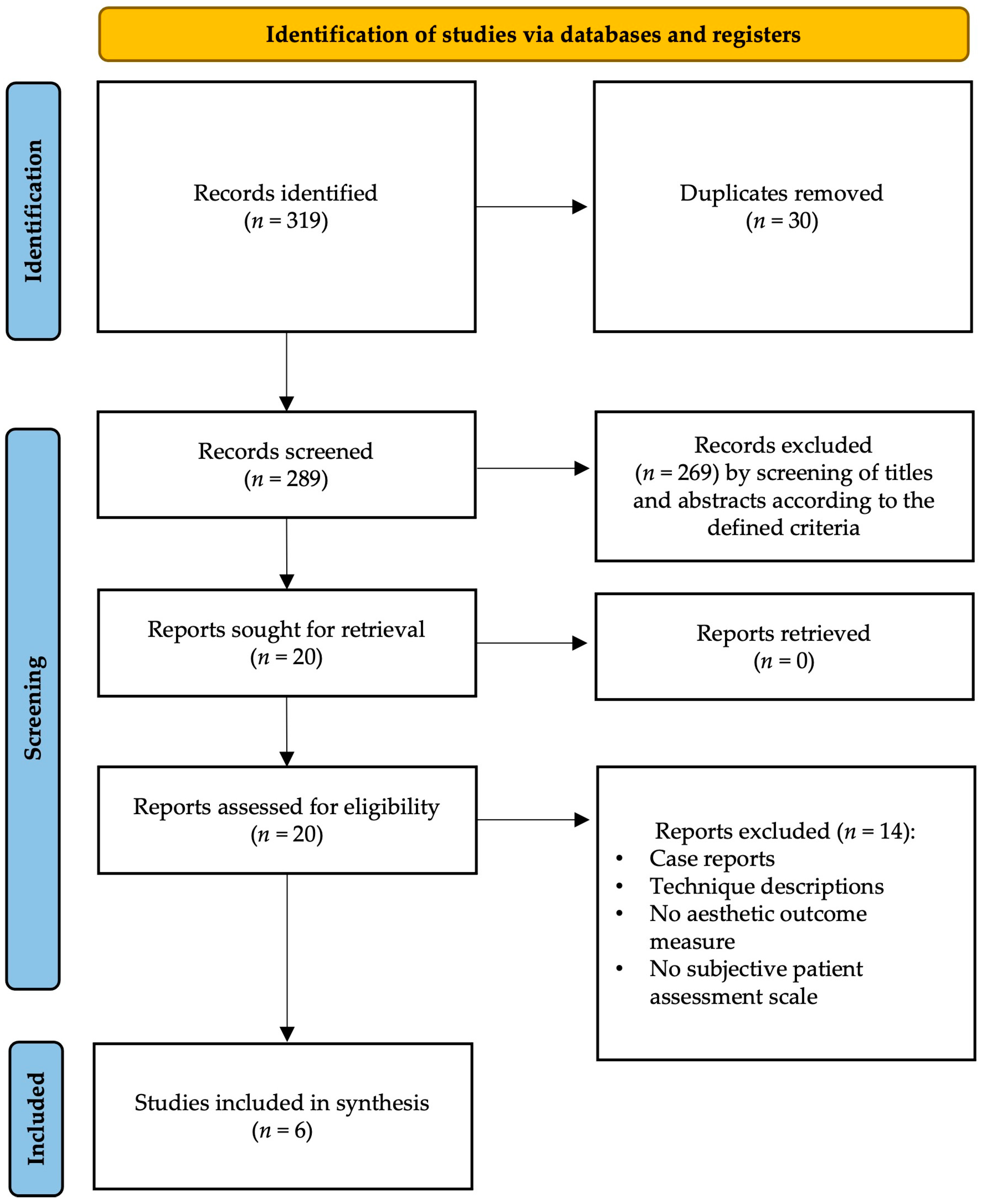
3.1. Literature Search Results
3.2. Study Details
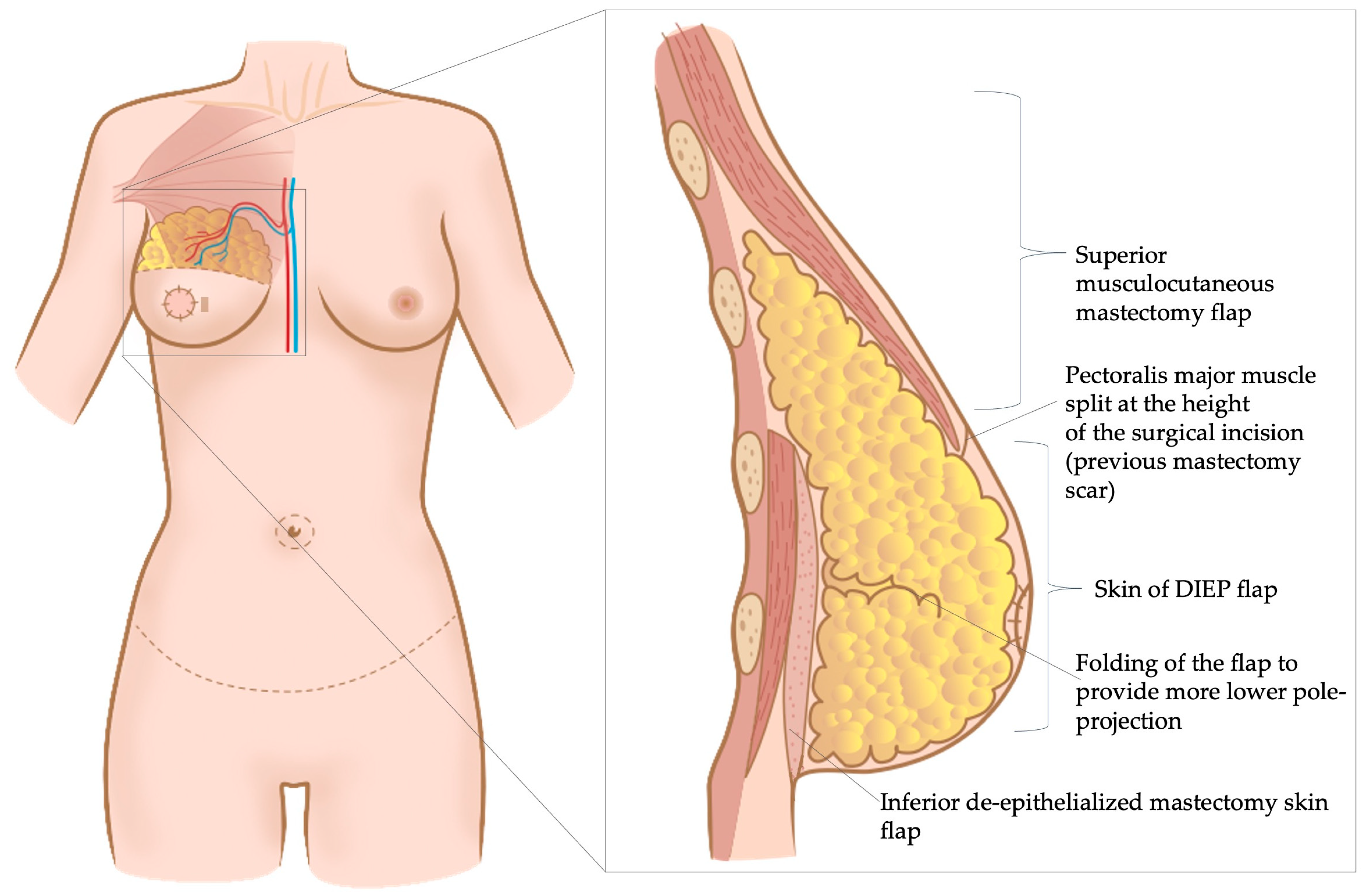
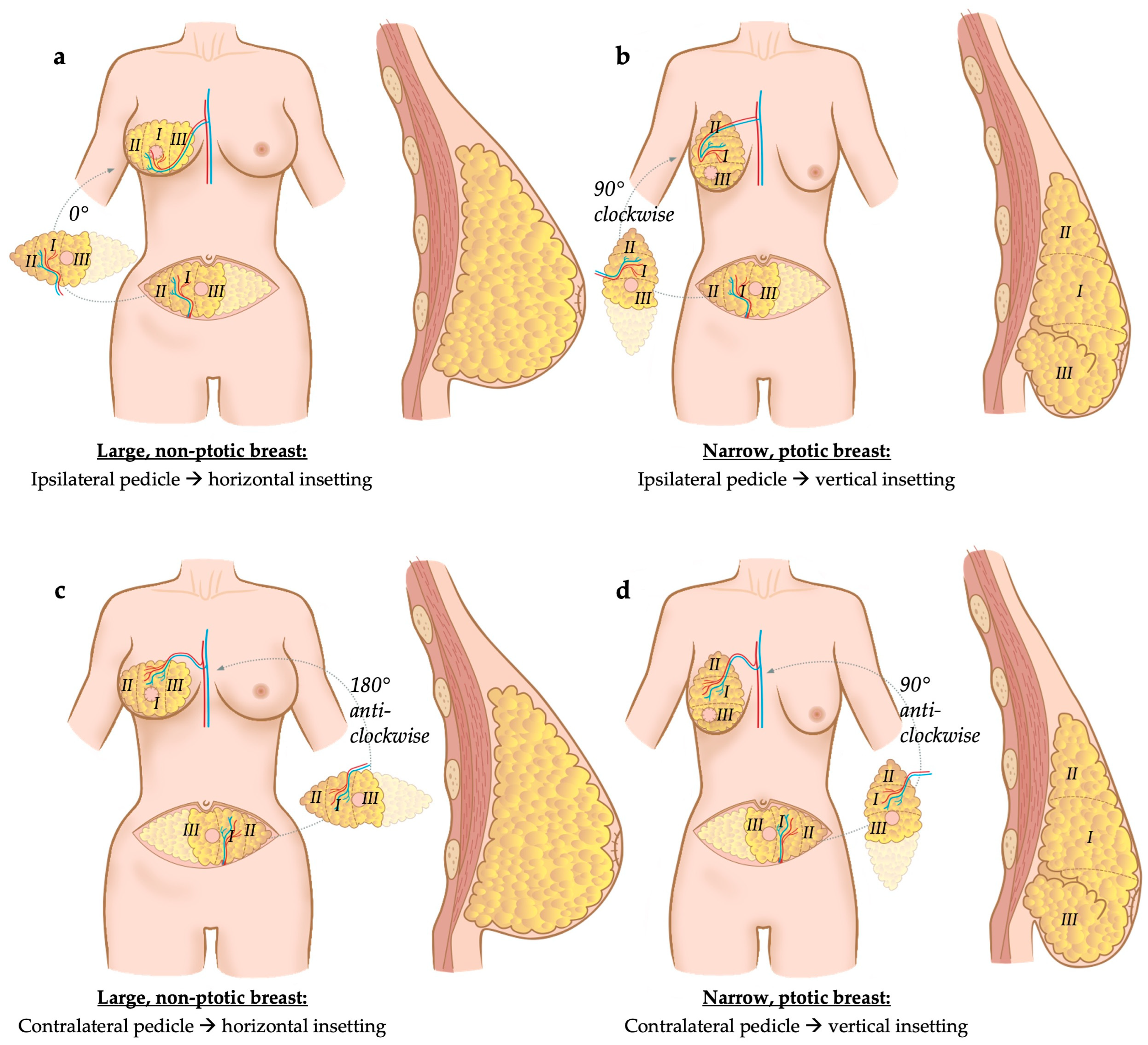
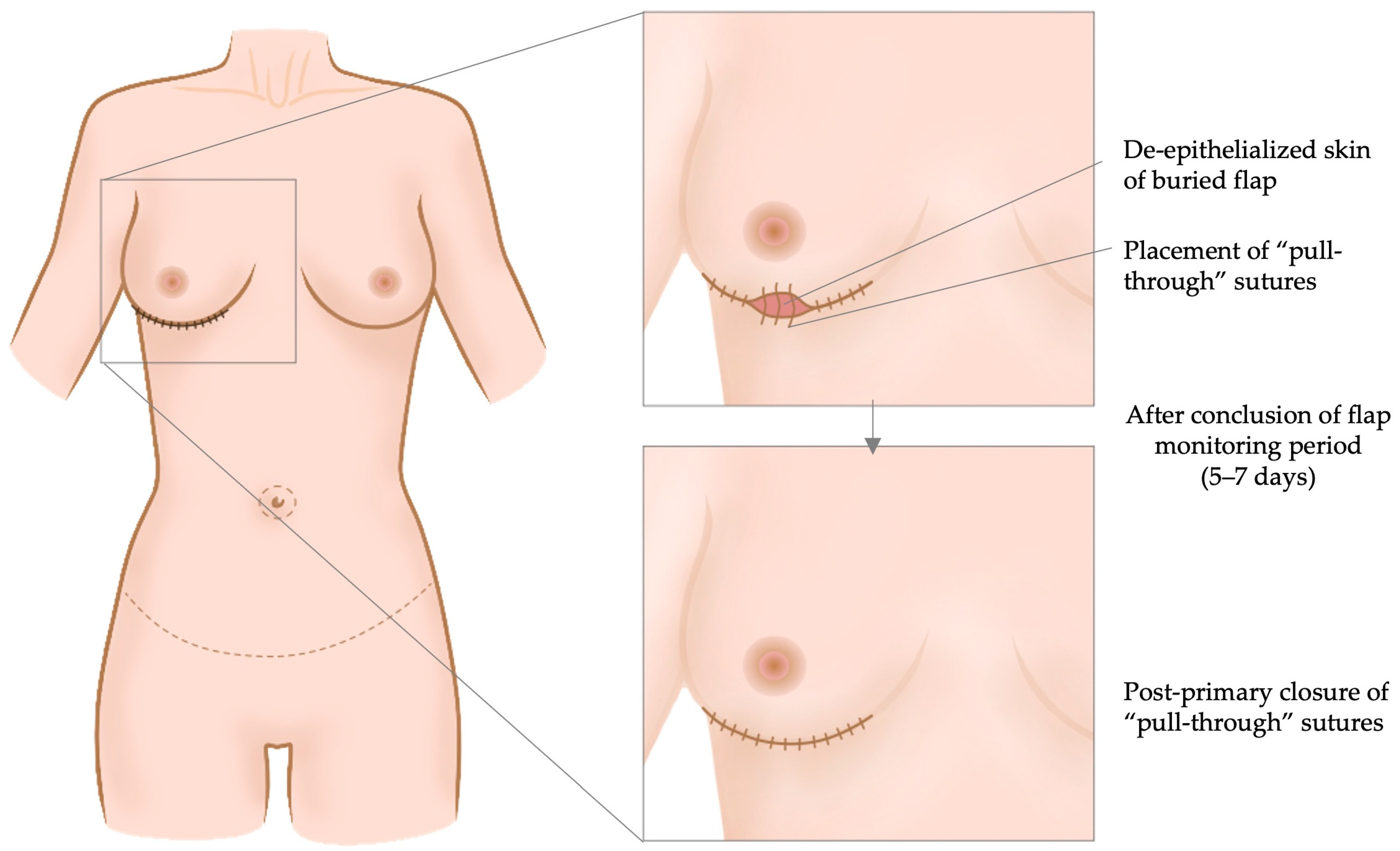
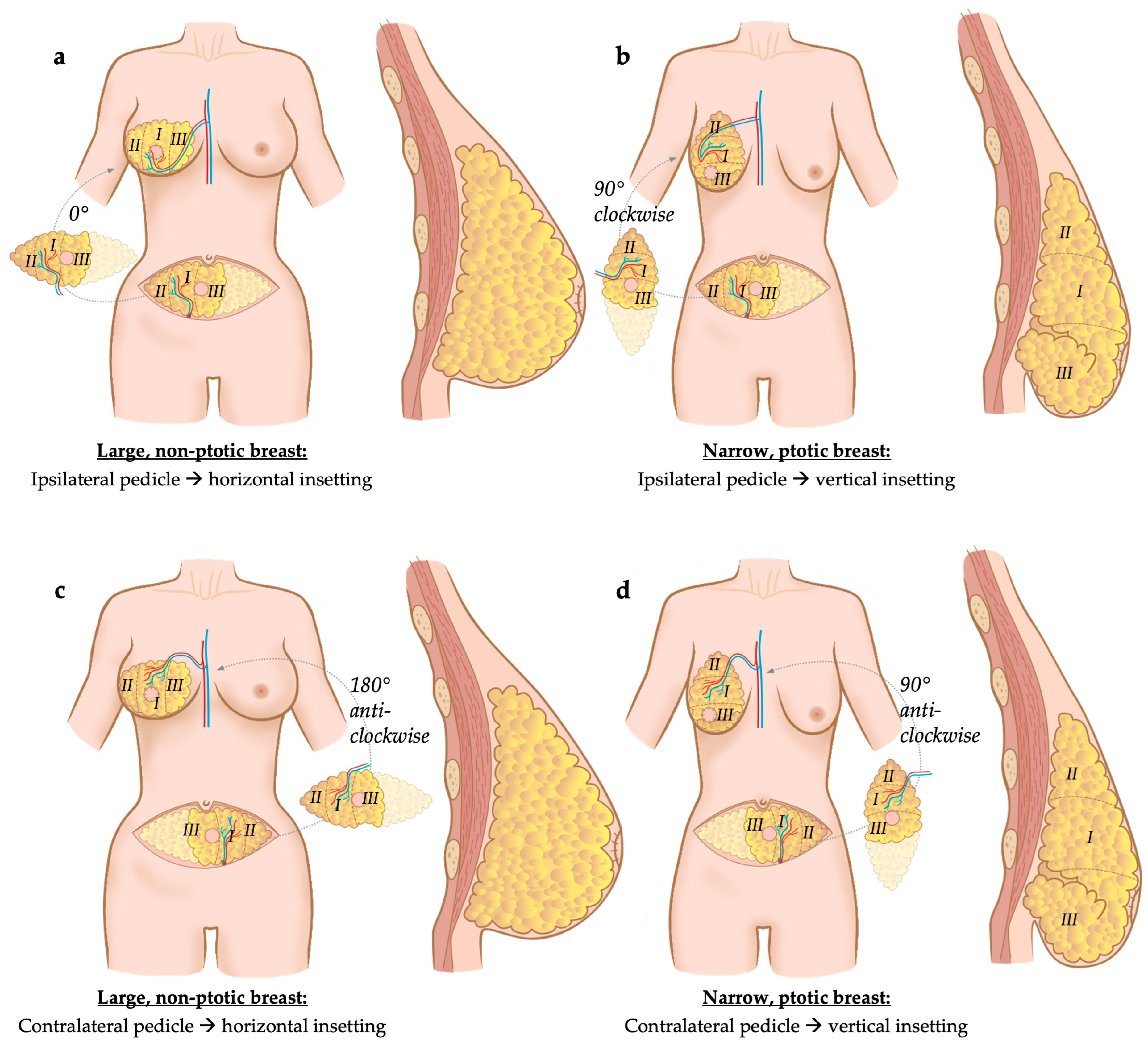
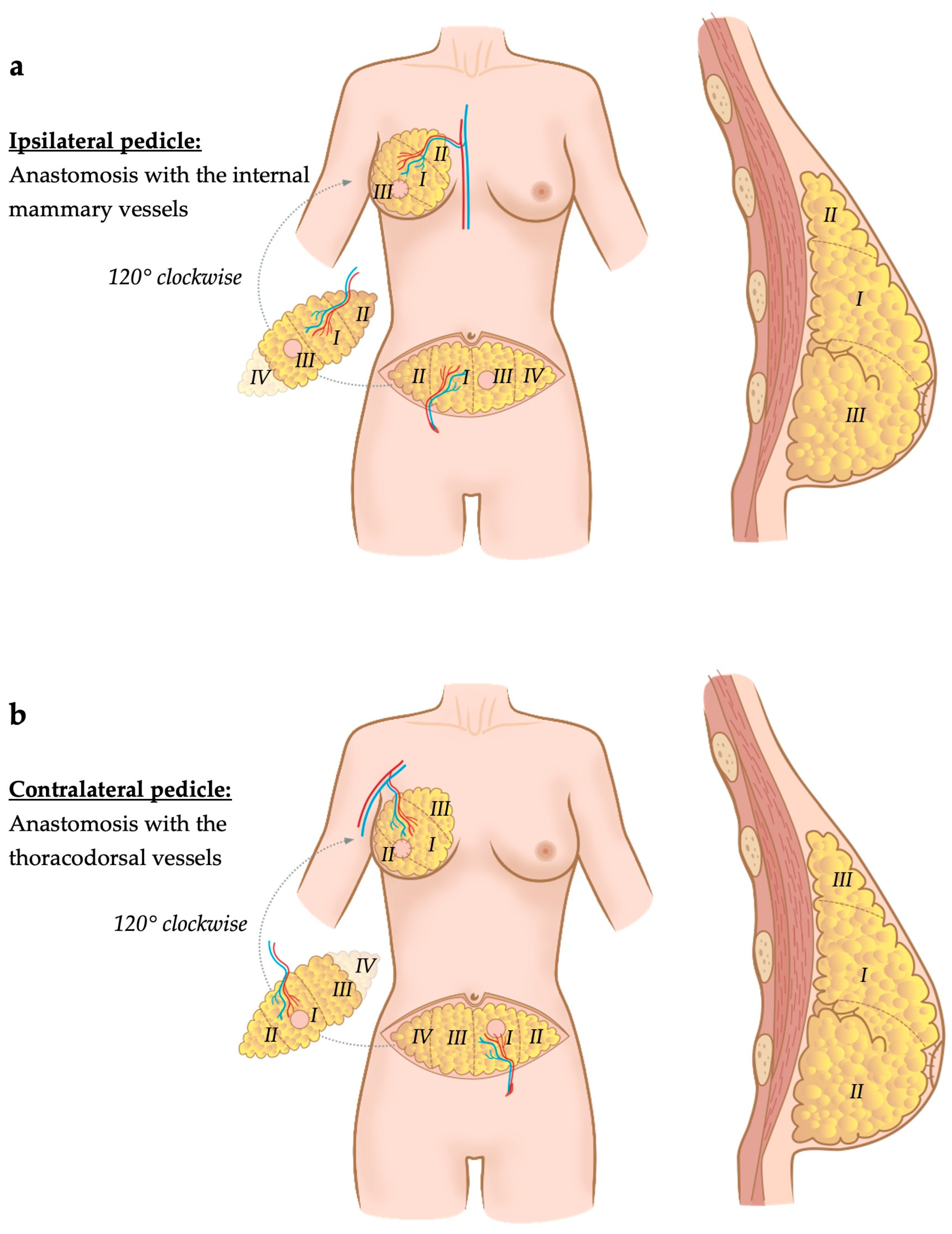
3.3. Inset and Shaping Techniques
3.4. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hassaine, Y.; Jacquet, E.; Seigneurin, A.; Delafosse, P. Evolution of breast cancer incidence in young women in a French registry from 1990 to 2018: Towards a change in screening strategy? Breast Cancer Res. 2022, 24, 87. [Google Scholar] [CrossRef]
- Foster, R.S., Jr.; Costanza, M.C. Breast self-examination practices and breast cancer survival. Cancer 1984, 53, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Kalager, M.; Haldorsen, T.; Bretthauer, M.; Hoff, G.; Thoresen, S.O.; Adami, H.O. Improved breast cancer survival following introduction of an organized mammography screening program among both screened and unscreened women: A population-based cohort study. Breast Cancer Res. 2009, 11, R44. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Garnier, H.; Colonna, M. Breast cancer epidemiology. Presse Med. 2019, 48, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Kuo, Y.F.; Shih, Y.C.T.; Giordano, S.H.; Berenson, A.B. Trends in breast cancer mortality by stage at diagnosis among young women in the United States. Cancer 2018, 124, 3500–3509. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, N.J. Care of the breast cancer survivor: Increased survival rates present a new set of challenges. Postgrad. Med. 2004, 116, 39–46. [Google Scholar] [CrossRef]
- Dragun, A.E.; Huang, B.; Tucker, T.C.; Spanos, W.J. Increasing mastectomy rates among all age groups for early stage breast cancer: A 10-year study of surgical choice. Breast J. 2012, 18, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Mamtani, A.; Morrow, M. Why Are There So Many Mastectomies in the United States? Annu. Rev. Med. 2017, 68, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Schmauss, D.; Machens, H.G.; Harder, Y. Breast Reconstruction after Mastectomy. Front. Surg. 2015, 2, 71. [Google Scholar] [CrossRef]
- Mortada, H.; AlNojaidi, T.F.; AlRabah, R.; Almohammadi, Y.; AlKhashan, R.; Aljaaly, H. Morbidity of the Donor Site and Complication Rates of Breast Reconstruction with Autologous Abdominal Flaps: A Systematic Review and Meta-Analysis. Breast J. 2022, 2022, 7857158. [Google Scholar] [CrossRef]
- Stillaert, F.; Lannau, B.; Van Landuyt, K.; Blondeel, P.N. The Prepectoral, Hybrid Breast Reconstruction: The Synergy of Lipofilling and Breast Implants. Plast. Reconstr. Surg. Glob. Open 2020, 8, e2966. [Google Scholar] [CrossRef]
- Rose, J.; Puckett, Y. Breast Reconstruction Free Flaps. In StatPearls; Copyright © 2023; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Chang, E.I. Latest Advancements in Autologous Breast Reconstruction. Plast. Reconstr. Surg. 2021, 147, 111e–122e. [Google Scholar] [CrossRef]
- Sapino, G.; Tay, S.K.; Maruccia, M.; Nanhekhan, L.; Watfa, W.; Mantovani, G.P.; Guillier, D.; Tedeschi, P.; Bramhall, R.; Di Summa, P.G. Abdominal-Based Microsurgical Breast Reconstruction: How to Inset the Flap to Maximize the Aesthetic Result-A Systematic Review. J. Clin. Med. 2023, 12, 6135. [Google Scholar] [CrossRef]
- Wu, S.S.; Duraes, E.F.R.; Scomacao, I.; Morisada, M.; Djohan, R.S.; Bernard, S.L.; Moreira, A.; Schwarz, G.S. Beauty Is in the Eye of the Beholder: Factors Influencing Disparity in Perceptions of Breast Reconstruction Aesthetic Outcomes. Plast. Reconstr. Surg. 2022, 150, 42e–50e. [Google Scholar] [CrossRef]
- Weick, L.; Brorson, F.; Jepsen, C.; Lidén, M.; Jensen, E.W.; Hansson, E. Giving meaning to patient reported outcomes in breast reconstruction after mastectomy—A systematic review of available scores and suggestions for further research. Breast 2022, 61, 91–97. [Google Scholar] [CrossRef]
- Silverman, S.R.; Schertz, L.A.; Yuen, H.K.; Lowman, J.D.; Bickel, C.S. Systematic review of the methodological quality and outcome measures utilized in exercise interventions for adults with spinal cord injury. Spinal Cord. 2012, 50, 718–727. [Google Scholar] [CrossRef]
- Holm, C.; Mayr, M.; Höfter, E.; Ninkovic, M. Perfusion zones of the DIEP flap revisited: A clinical study. Plast. Reconstr. Surg. 2006, 117, 37–43. [Google Scholar] [CrossRef]
- Gravvanis, A.; Samouris, G.; Galani, E.; Tsoutsos, D. Dual plane diep flap inset: Optimizing esthetic outcome in delayed autologous breast reconstruction. Microsurgery 2015, 35, 432–440. [Google Scholar] [CrossRef]
- Gravvanis, A.; Kakagia, D.; Samouris, G.; Galani, E.; Tsoutsos, D. Tips and Outcomes of a New DIEP Flap Inset in Delayed Breast Reconstruction: The Dual-Plane Technique. J. Reconstr. Microsurg. 2016, 32, 366–370. [Google Scholar] [CrossRef]
- Razzano, S.; Marongiu, F.; Wade, R.; Figus, A. Optimizing DIEP Flap Insetting for Immediate Unilateral Breast Reconstruction: A Prospective Cohort Study of Patient-Reported Aesthetic Outcomes. Plast. Reconstr. Surg. 2019, 143, 261e–270e. [Google Scholar] [CrossRef]
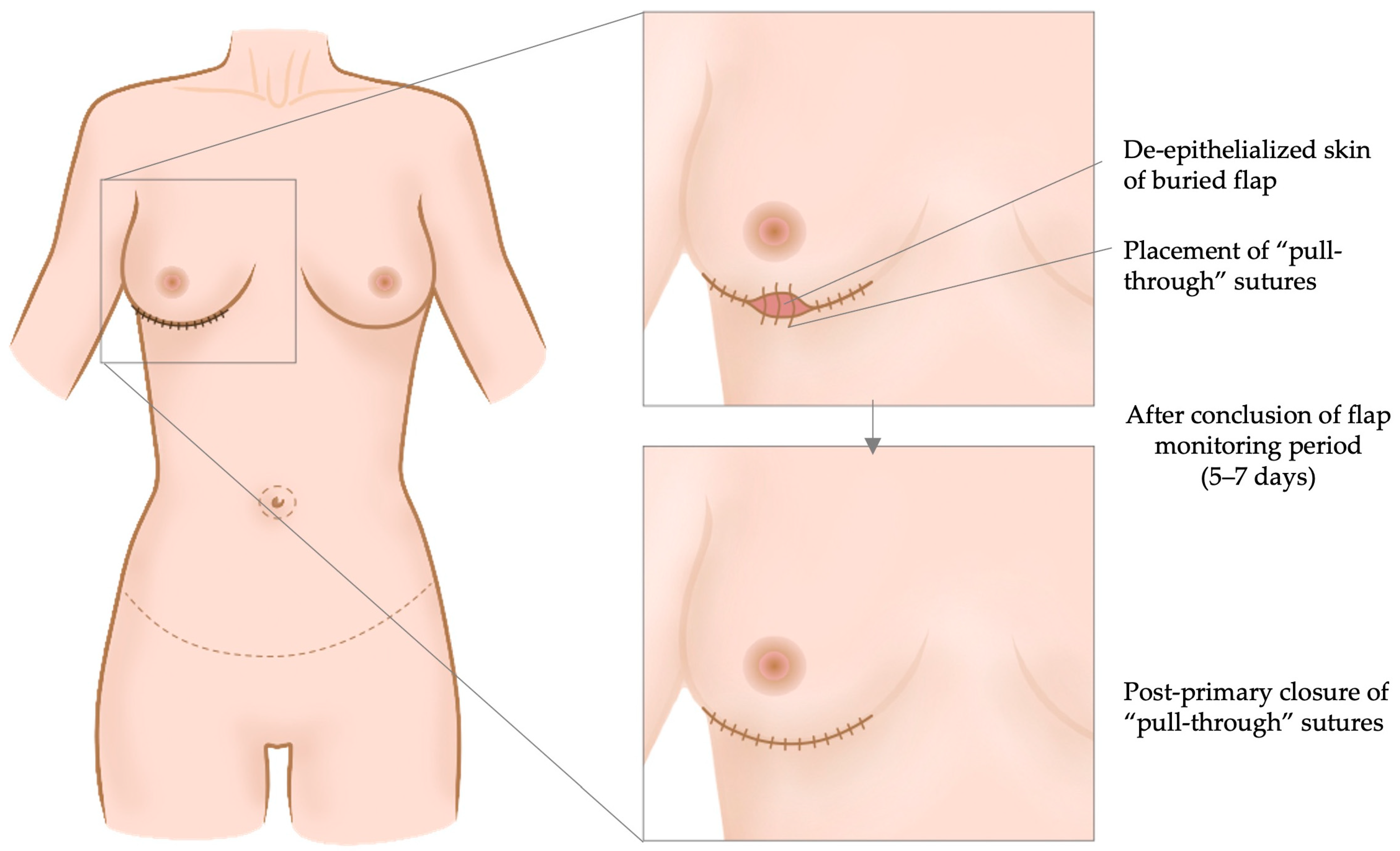
- Francis, E.C.; Dimovska, E.O.F.; Chou, H.H.; Lin, Y.L.; Cheng, M.H. Nipple-sparing mastectomy with immediate breast reconstruction with a deep inferior epigastric perforator flap without skin paddle using delayed primary retention suture. J. Surg. Oncol. 2022, 125, 1202–1210. [Google Scholar] [CrossRef]
- Long, A.S.; Ching, A.H.; Hauc, S.C.; Mozaffari, M.A.; Junn, A.H.; Rivera, J.C.; Almeida, M.N.; Alper, D.P.; Allam, O.; Alperovich, M. Flap to Mastectomy Mass: Are Higher Ratios Associated with Greater Breast Reconstruction Satisfaction? J. Reconstr. Microsurg. 2023, 39, 209–213. [Google Scholar] [CrossRef]
- Dung, P.T.V.; Sơn, T.T.; Dung, V.T.; Hậu, N.X.; Nghĩa, P.T. Techniques of inserting deep inferior epigastric perforator flap obliquely in immediate breast reconstruction after total mastectomy. JPRAS Open 2023, 36, 1–7. [Google Scholar] [CrossRef]
- Regnault, P. Breast ptosis. Definition and treatment. Clin. Plast. Surg. 1976, 3, 193–203. [Google Scholar] [CrossRef]
- Wagner, R.D.; Hamilton, K.L.; Doval, A.F.; Spiegel, A.J. How to Maximize Aesthetics in Autologous Breast Reconstruction. Aesthetic Surg. J. 2020, 40, S45–S54. [Google Scholar] [CrossRef]
- Munder, B.; Andree, C.; Witzel, C.; Fertsch, S.; Stambera, P.; Schulz, T.; Fleischer, O.; Hagouan, M.; Grüter, L.; Aufmesser, B.; et al. The DIEP Flap as Well-established Method of Choice for Autologous Breast Reconstruction with a Low Complication Rate—Retrospective Single-centre 10-Year Experience. Geburtshilfe Frauenheilkd. 2020, 80, 628–638. [Google Scholar] [CrossRef] [PubMed]
- Grünherz, L.; Keijzer, W.; Uyulmaz, S.; Fertsch, S.; Imhof, L.; Käser, S.; Farhadi, J.; Lindenblatt, N. Donor site aesthetics and morbidity after DIEP flap breast reconstruction-A retrospective multicenter study. Breast J. 2020, 26, 1980–1986. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, A.C.; Çizmeci, O.; Aydin, H.; Emekli, U.; Özden, B.C.; Ulug, B.T. Comparison of the early and late postoperative results in cases with pedicled transverse rectus abdominis musculocutaneous flap breast reconstruction: Twenty-year follow-up. Turk. J. Plast. Surg. 2020, 28, 98–103. [Google Scholar]
- Fayman, M.S.; Potgieter, E.; Becker, P.J. The pedicle tram flap: A focus on improved aesthetic outcome. Aesthetic Plast. Surg. 2006, 30, 301–308. [Google Scholar] [CrossRef]
- Pompei, B.; Farhadi, J. Diep Flap Volume Augmentation: Literature Review and “Calzone” Flap Shaping Technique. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1933–1939. [Google Scholar] [CrossRef]
- Odobescu, A.; Goodwin, I.; Berbiche, D.; BouMerhi, J.; Harris, P.G.; Danino, M.A. High Fidelity Microsurgical Simulation: The Thiel Model and Evaluation Instrument. Plast. Surg. 2019, 27, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Koolen, P.G.; Lee, B.T.; Lin, S.J.; Erhard, H.A.; Greenspun, D.T. Bipedicle-conjoined perforator flaps in breast reconstruction. J. Surg. Res. 2015, 197, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Seth, A.K.; Koolen, P.G.L.; Sultan, S.M.; Lee, B.T.; Erhard, H.A.; Greenspun, D.T. Unilateral Autologous Breast Reconstruction with Bi-pedicled, Conjoined Deep Inferior Epigastric Perforator Flaps. J. Reconstr. Microsurg. 2019, 35, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.G.; Rozen, W.M.; Chow, W.T.; Chowdhry, M.; Fitzgerald O’Connor, E.; Sharma, H.; Griffiths, M.; Ramakrishnan, V.V. Stacked and bipedicled abdominal free flaps for breast reconstruction: Considerations for shaping. Gland. Surg. 2016, 5, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Hamdi, M.; Al Harami, S.; Chahine, F.; Giunta, G.; De Baerdemaeker, R.; Zeltzer, A. The “Hug Flap”: Surgical Technique to Enhance the Aesthetic Breast Projection in Autologous Breast Reconstruction. Aesthetic Surg. J. 2021, 41, NP1462–NP1470. [Google Scholar] [CrossRef] [PubMed]
- Jeong, W.S.; Han, W.; Eom, J.S. Comparison of Aesthetic Outcomes Between Vertical and Horizontal Flap Insets in Breast Reconstruction with the TRAM or DIEP Flaps. Aesthetic Plast. Surg. 2017, 41, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Laporta, R.; Longo, B.; Sorotos, M.; Pagnoni, M.; Santanelli Di Pompeo, F. One-stage DIEP flap breast reconstruction: Algorithm for immediate contralateral symmetrization. Microsurgery 2016, 36, 7–19. [Google Scholar] [CrossRef]
- El Khatib, A.; Bou-Merhi, J.; Awaida, C.; Bernier, C.; Gagnon, A.; Retchkiman, M.; Odobescu, A.; Danino, M.A. Immediate fine-tuning of DIEP flaps using the Wise pattern mastectomy: Description of the technique and a retrospective analysis of complication rates. Ann. Chir. Plast. Esthet. 2022, 67, 189–195. [Google Scholar] [CrossRef]
- Wang, T.; He, J.; Xu, H.; Ma, S.; Dong, J. Achieving Symmetry in Unilateral DIEP Flap Breast Reconstruction: An Analysis of 126 Cases over 3 Years. Aesthetic Plast. Surg. 2015, 39, 63–68. [Google Scholar] [CrossRef]
- Tomita, K.; Yano, K.; Hata, Y.; Nishibayashi, A.; Hosokawa, K. DIEP Flap Breast Reconstruction Using 3-dimensional Surface Imaging and a Printed Mold. Plast. Reconstr. Surg. Glob. Open 2015, 3, e316. [Google Scholar] [CrossRef]
- Tomita, K.; Yano, K.; Taminato, M.; Nomori, M.; Hosokawa, K. DIEP Flap Breast Reconstruction in Patients with Breast Ptosis: 2-Stage Reconstruction Using 3-Dimensional Surface Imaging and a Printed Mold. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1511. [Google Scholar] [CrossRef] [PubMed]
- Tregaskiss, A.; Vermaak, P.V.; Boulton, R.; Morris, R.J. The template technique for breast mound planning when using abdominal flaps for breast reconstruction. Breast 2012, 21, 686–689. [Google Scholar] [CrossRef] [PubMed]
- Raposio, E.; Belgrano, V.; Santi, P.; Chiorri, C. Which is the Ideal Breast Size?: Some Social Clues for Plastic Surgeons. Ann. Plast. Surg. 2016, 76, 340–345. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Article (Year, Author) | Study Design | Patients (n) | Inset/Shaping | Questionnaire (PROM) | Time-Point of Evaluation | Presence of Control Group | Outcome |
|---|---|---|---|---|---|---|---|
| 2015, Gravvanis et al. [19] | prospective, comparative | 50 | group A (n = 25): flap inset using prepectoral single plane; group B (n = 25): flap inset using dual plane (pre- and subpectoral) | Likert scale | not specified | Yes (prepectoral, single plane) | patient self-evaluation, aesthetic outcome evaluated by 30 evaluators (7 questions based on postoperative photographs and VAS (0–100 mm)) |
| 2016, Gravvanis et al. [20] | prospective | 42 | dual plane inset | Likert scale | 2 and 24 months | none | patient self-evaluation |
| 2019, Razzano et al. [21] | prospective | 70 | inset upon the author’s algorithm depending on patients’ morphology, contra- or ipsilateral breast, uni- or bipedicled flap, shape and volume of the contralateral breast | BREAST-Q | 12 months | None | patient self-evaluation), aesthetic outcome evaluated by three independent assessors |
| 2022, Francis et al. [22] | prospective, comparative | 24 | post-primary retention suture after burying the DIEP flap instead of using a skin paddle | BREAST-Q | 9 months | yes (monitoring skin paddle) | patient self-evaluation, Manchester scar scale (the lower the score, the better the cosmetic outcome) completed by seven plastic surgeons/fellows |
| 2023, Long et al. [23] | retrospective | 45 | higher flap-to-mastectomy mass ratio | BREAST-Q | 21 months | none | patient self-evaluation |
| 2023, Dung et al. [24] | retrospective | 40 | oblique inset, flap volume 10% > mastectomy volume (water displacement) | BREAST-Q | 6 months | none | patient self-evaluation |
| Article (Year, Author) | Mastectomy laterality and Type (n) | Radiation Therapy | Contralateral Mastopexy/Reduction Mammoplasty (n) | Immediate vs. Delayed Reconstruction | Aesthetic Outcome Score |
|---|---|---|---|---|---|
| 2015, Gravvanis et al. [19] | Unilateral, radical modified (50/50) | 50/50, adjuvant | Intervention group (dual plane, 17/25) Control group (pre-pectoral, 18/25) | Delayed | Likert scale completed by 17/25 patients in the prepectoral plane group and 16/25 patients in the dual plane group: significant difference in favor of the dual plane group in the questions about “satisfaction without brasserie”, “ptosis of breast with time” and “fullness of the upper pole” VAS evaluated by 30 external observers: significant difference in favor of dual plane in the questions about “overall breast appearance”, “superior scar”, “superior mastectomy skin”, “natural transition”, “outline of the breast”; 26/30 evaluators preferred dual plane group |
| 2016, Gravvanis et al. [20] | Unilateral, radical modified (42/42) | 42/42, adjuvant | 26/42 | Delayed | Likert scale completed by 42/42 patients: no significant difference between 2-month and 2-year follow-up, especially high scores in the questions about “satisfaction with brasserie”, “satisfaction without brasserie”, and “fullness of the upper pole” at the 2-year follow-up |
| 2019, Razzano et al. [21] | Unilateral, both skin-sparing (64/70) and non-skin-sparing (6/70) | Not reported | 29/70 | Immediate | BREAST-Q: 82/100 points in the questions about “overall satisfaction”, 81/100 points in the questions about “satisfaction with breasts”, the highest scores achieved in the questions about “satisfaction with the surgeon, medical staff and office staff”, lowest scores achieved in the questions about “sexual well-being”. Photos from 51/70 patients evaluated by three independent evaluators (surgeon, nurse, secretary): generally favorable outcome (mostly “good” or “very good”, agreement on breast projection, shape and volume, but disagreement in evaluation of breast symmetry and ptosis |
| 2022, Francis et al. [22] | Nipple-sparing mastectomy (12/12) | 1/12 patients in the control group and 5/12 patients in the intervention group with adjuvant chemotherapy or radiotherapy | Not reported | 12/12 immediate reconstructions with monitoring skin paddle, 3/12 patients in the intervention group with delayed reconstruction | BREAST-Q: tend to be more satisfied in the intervention group (68/100 vs. 62/100 points in the questions about “satisfaction with breasts”) statistically significant difference only in the domain of “satisfaction with their surgeon” Manchester scar scale: Statistically significant difference in the domains “scar distortion”, “visual analogue scale” and “overall scar scale” favoring the intervention group |
| 2023, Long et al. [23] | 25/45 bilateral, 20/45 unilateral, 5/45 nipple-sparing, 40/45 type not reported | 18/45 adjuvant | Not reported | Not reported | BREAST-Q: average score of 65/100 points in the domain “satisfaction with the breasts”, significantly higher score in patients with increased flap mass compared to the mastectomy mass (average difference in mass ~26.3%) |
| 2023, Dung et al. [24] | Laterality not reported, radical modified mastectomy | Not reported | Not reported | Immediate | BREAST-Q: average score of 62/100 points in the questions about “satisfaction with the breasts” |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zucal, I.; De Pellegrin, L.; Parodi, C.; Harder, Y.; Schweizer, R. The Influence of Inset and Shaping of Abdominal-Based Free Flap Breast Reconstruction on Patient-Reported Aesthetic Outcome Scores—A Systematic Review. J. Clin. Med. 2024, 13, 2395. https://doi.org/10.3390/jcm13082395
Zucal I, De Pellegrin L, Parodi C, Harder Y, Schweizer R. The Influence of Inset and Shaping of Abdominal-Based Free Flap Breast Reconstruction on Patient-Reported Aesthetic Outcome Scores—A Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2395. https://doi.org/10.3390/jcm13082395
Chicago/Turabian StyleZucal, Isabel, Laura De Pellegrin, Corrado Parodi, Yves Harder, and Riccardo Schweizer. 2024. "The Influence of Inset and Shaping of Abdominal-Based Free Flap Breast Reconstruction on Patient-Reported Aesthetic Outcome Scores—A Systematic Review" Journal of Clinical Medicine 13, no. 8: 2395. https://doi.org/10.3390/jcm13082395
APA StyleZucal, I., De Pellegrin, L., Parodi, C., Harder, Y., & Schweizer, R. (2024). The Influence of Inset and Shaping of Abdominal-Based Free Flap Breast Reconstruction on Patient-Reported Aesthetic Outcome Scores—A Systematic Review. Journal of Clinical Medicine, 13(8), 2395. https://doi.org/10.3390/jcm13082395