
Comparative Analysis of Long-Term Outcomes in Valve-Sparing Aortic Root Reimplantation: Full Sternotomy versus Mini-Sternotomy Approach †

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. MIRAGE Registry
2.2. Surgical Technique
2.3. Definitions and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient and Surgical Characteristics
3.2. In-Hospital Course
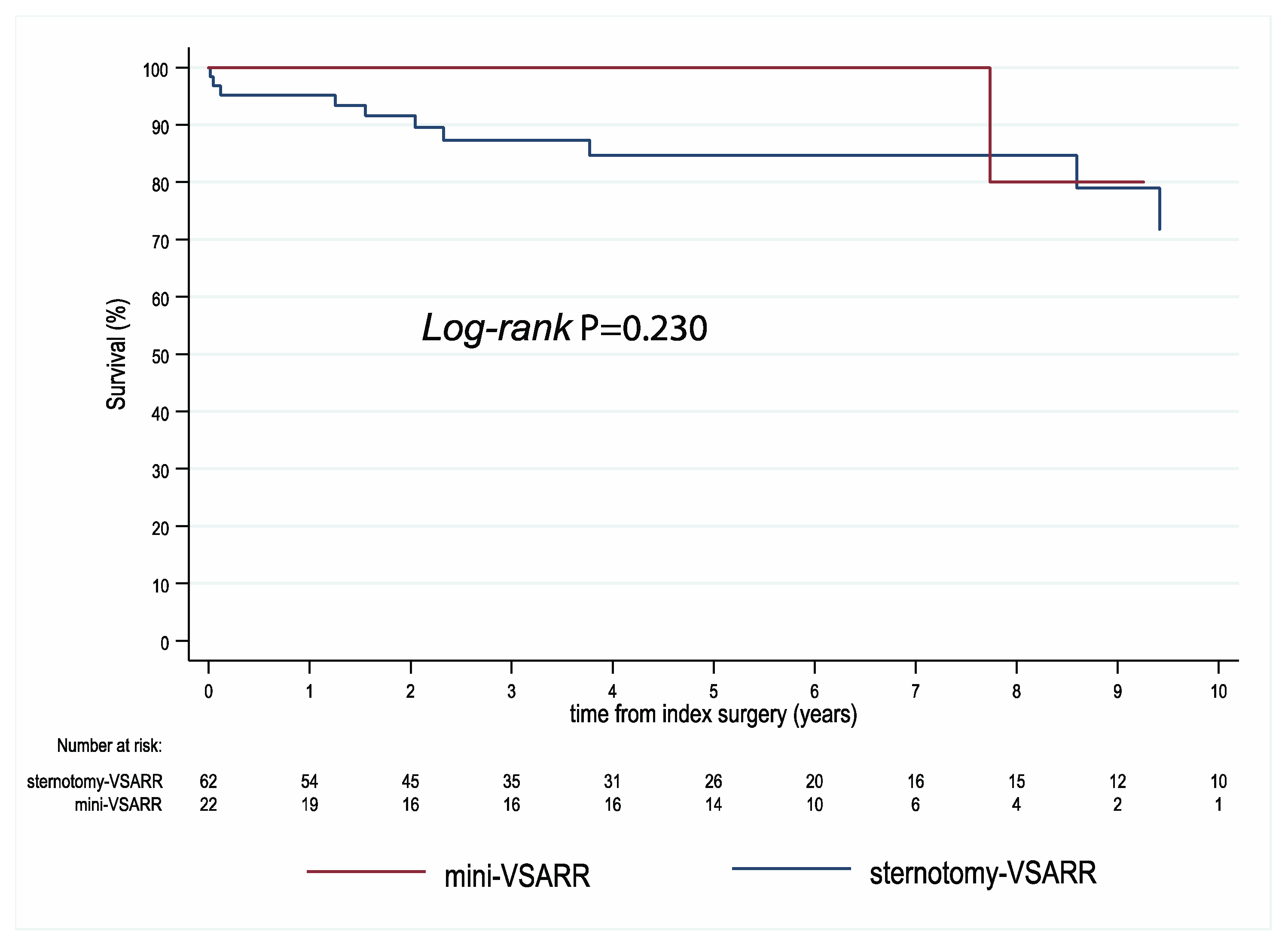
3.3. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schill, M.R.; Kachroo, P. Surgical options for aortic root aneurysm disease: Which procedure, which patient. Curr. Opin. Cardiol. 2021, 36, 683–688. [Google Scholar] [CrossRef]
- Ziganshin, B.A.; Kargin, N.; Zafar, M.A.; Elefteriades, J.A. The natural history of aortic root aneurysms. Ann. Cardiothorac. Surg. 2023, 12, 213–224. [Google Scholar] [CrossRef]
- Shrestha, M.; Boethig, D.; Krüger, H.; Kaufeld, T.; Martens, A.; Haverich, A.; Beckmann, E. Valve-sparing aortic root replacement using a straight tube graft (David I procedure). J. Thorac. Cardiovasc. Surg. 2023, 166, 1387–1397.e10. [Google Scholar] [CrossRef]
- Beckmann, E.; Kaufeld, T.; Martens, A.; Rudolph, L.; Shrestha, M.; Krueger, H.; Haverich, A.; Shrestha, M.L. Aortic valve-sparing root replacement (David-I) for acute aortic dissection type A. Ann. Cardiothorac. Surg. 2023, 12, 276–278. [Google Scholar] [CrossRef]
- Iannacone, E.M.; Lau, C., Jr.; Soletti, G.; Olaria, R.P.; Harik, L.; Dimagli, A.; Girardi, L.N. Aortic valve-sparing root replacement or Bentall? Ann. Cardiothorac. Surg. 2023, 12, 168–178. [Google Scholar] [CrossRef]
- Writing Committee Members; Isselbacher, E.M.; Preventza, O.; Hamilton Black, J., 3rd; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; et al. 2022 ACC/AHA guideline for the diagnosis and management of aortic disease: A report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J. Thorac. Cardiovasc. Surg. 2023, 166, e182–e331. [Google Scholar]
- Staromłyński, J.; Kowalewski, M.; Smoczyński, R.; Suwalski, P. Minimally invasive approach to ascending aorta and aortic root surgery. Interact. Cardiovasc. Thorac. Surg. 2021, 32, 163. [Google Scholar] [CrossRef]
- Monsefi, N.; Risteski, P.; Miskovic, A.; Moritz, A.; Zierer, A. Midterm Results of a Minimally Invasive Approach in David Procedure. Thorac. Cardiovasc. Surg. 2018, 66, 301–306. [Google Scholar] [CrossRef]
- Shrestha, M.; Krueger, H.; Umminger, J.; Koigeldiyev, N.; Beckmann, E.; Haverich, A.; Martens, A. Minimally invasive valve sparing aortic root replacement (David procedure) is safe. Ann. Cardiothorac. Surg. 2015, 4, 148–153. [Google Scholar] [PubMed]
- Sef, D.; Bahrami, T.; Raja, S.G.; Klokocovnik, T. Current trends in minimally invasive valve-sparing aortic root replacement—Best available evidence. J. Card. Surg. 2022, 37, 1684–1690. [Google Scholar] [CrossRef] [PubMed]
- Staromłyński, J.; Kowalewski, M.; Sarnowski, W.; Smoczyński, R.; Witkowska, A.; Bartczak, M.; Drobiński, D.; Wierzba, W.; Suwalski, P. Midterm results of less invasive approach to ascending aorta and aortic root surgery. J. Thorac. Dis. 2020, 12, 6446–6457. [Google Scholar] [CrossRef]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardiothorac. Surg. 2012, 41, 734–744, discussion 744–745. [Google Scholar] [CrossRef]
- Kowalewski, M.; Pasierski, M.; Makhoul, M.; Comanici, M.; Dąbrowski, E.J.; Matteucci, M.; Litwinowicz, R.; Kowalówka, A.; Wańha, W.; Jiritano, F.; et al. Topical vancomycin for sternal wound infection prophylaxis. A systematic review and updated meta-analysis of over 40,000 cardiac surgery patients. Surgery 2023, 174, 1102–1112. [Google Scholar] [CrossRef]
- Kowalewski, M.; Pawliszak, W.; Zaborowska, K.; Navarese, E.P.; Szwed, K.A.; Kowalkowska, M.E.; Kowalewski, J.; Borkowska, A.; Anisimowicz, L. Gentamicin-collagen sponge reduces the risk of sternal wound infections after heart surgery: Meta-analysis. J. Thorac. Cardiovasc. Surg. 2015, 149, 1631–1640.e1–e6. [Google Scholar] [CrossRef]
- Petäjä, L.; Vaara, S.; Liuhanen, S.; Suojaranta-Ylinen, R.; Mildh, L.; Nisula, S.; Korhonen, A.-M.; Kaukonen, K.-M.; Salmenperä, M.; Pettilä, V. Acute Kidney Injury After Cardiac Surgery by Complete KDIGO Criteria Predicts Increased Mortality. J. Cardiothorac. Vasc. Anesth. 2017, 31, 827–836. [Google Scholar] [CrossRef] [PubMed]
- Lebehn, M.; Vahl, T.; Kampaktsis, P.; Hahn, R.T. Contemporary Evaluation and Clinical Treatment Options for Aortic Regurgitation. J. Cardiovasc. Dev. Dis. 2023, 10, 364. [Google Scholar] [CrossRef]
- Sievers, H.-H.; Schmidtke, C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J. Thorac. Cardiovasc. Surg. 2007, 133, 1226–1233. [Google Scholar] [CrossRef]
- Pasierski, M.; Batko, J.; Kuźma, Ł.; Wańha, W.; Jasiński, M.; Widenka, K.; Deja, M.; Bartuś, K.; Hirnle, T.; Wojakowski, W.; et al. Surgical ablation, left atrial appendage occlusion or both? Nationwide registry analysis of cardiac surgery patients with underlying atrial fibrillation. Eur. J. Cardio-Thoracic Surg. 2024, 65, ezae014. [Google Scholar] [CrossRef]
- Steyerberg, E.W. Clinical Prediction Models. A Practical Approach to Development, Validation, and Updating; Springer: New York, NY, USA, 2009. [Google Scholar]
- Dieberg, G.; Smart, N.A.; King, N. Minimally invasive cardiac surgery: A systematic review and meta-analysis. Int. J. Cardiol. 2016, 223, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, M.; Kaufeld, T.; Shrestha, P.; Martens, A.; Rustum, S.; Rudolph, L.; Krüger, H.; Arar, M.; Haverich, A.; Beckmann, E. Valve-sparing David procedure via minimally invasive access does not compromise outcome. Front. Cardiovasc. Med. 2022, 9, 966126. [Google Scholar] [CrossRef] [PubMed]
- Mikus, E.; Micari, A.; Calvi, S.; Salomone, M.; Panzavolta, M.; Paris, M.; Del Giglio, M. Mini-Bentall: An Interesting Approach for Selected Patients. Innovations 2017, 12, 41–45. [Google Scholar] [PubMed]
- Deschka, H.; Erler, S.; Machner, M.; El-Ayoubi, L.; Alken, A.; Wimmer-Greinecker, G. Surgery of the ascending aorta, root remodelling and aortic arch surgery with circulatory arrest through partial upper sternotomy: Results of 50 consecutive cases. Eur. J. Cardio-Thoracic Surg. 2013, 43, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Pyo, W.K.; Ok, Y.J.; Kim, H.J.; Kim, J.B. Mini-access open arch repair. J. Thorac. Dis. 2021, 13, 2233–2241. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stoliński, J.; Plicner, D.; Grudzień, G.; Kruszec, P.; Fijorek, K.; Musiał, R.; Andres, J. Computed Tomography Helps to Plan Minimally Invasive Aortic Valve Replacement Operations. Ann. Thorac. Surg. 2016, 101, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.A., Jr.; Wood, K.L.; Melvin, A.L.; Lebow, B.F.; Knight, P.A. Video assisted right mini-thoracotomy for aortic root replacement. J. Vis. Surg. 2018, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Tsaroev, B.; Sharifulin, R.; Karadzha, A.; Pivkin, A.; Afanasyev, A.; Zalesov, A.; Mustaev, M.; Bogachev-Prokophiev, A. The David procedure through a right anterior minithoracotomy. Multimedia Man. Cardio-Thoracic Surg. 2023, 2023. [Google Scholar]
- Jawarkar, M.; Manek, P.; Wadhawa, V.; Doshi, C. Mini-Bentall Surgery: The Right Thoracotomy Approach. J. Chest Surg. 2021, 54, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Sromicki, J.; Van Hemelrijck, M.; Schmiady, M.O.; Greutmann, M.; Tempesta, F.B.; Mestres, C.-A.; Vogt, P.R.; Carrel, T.P.; Holubec, T. Twenty-five year experience with aortic valve-sparing root replacement in a single teaching center. Front. Cardiovasc. Med. 2023, 10, 1104149. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, E.; Martens, A.; Krüger, H.; Korte, W.; Kaufeld, T.; Stettinger, A.; Haverich, A.; Shrestha, M.L. Aortic valve-sparing root replacement in patients with bicuspid aortic valve: Long-term outcome with the David I procedure over 20 years. Eur. J. Cardio-Thoracic Surg. 2021, 58, 86–93. [Google Scholar] [CrossRef]
- Gocoł, R.; Bis, J.; Malinowski, M.; Ciosek, J.; Hudziak, D.; Morkisz, Ł.; Jasiński, M.; Deja, M.A. Comparison of bicuspid and tricuspid aortic valve repair. Eur. J. Cardio-Thoracic Surg. 2020, 59, 1183–1190. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients | PS-Matched Patients | |||||
|---|---|---|---|---|---|---|---|
| Sternotomy-VSARR (62) | Mini-VSARR (22) | Pvalue | Sternotomy-VSARR (17) | Mini-VSARR (17) | Pvalue | ||
| Age, years (median (IQR)) | 39 (28, 52) | 64 (49, 65) | <0.001 | 63 (52, 68) | 53 (48, 64) | 0.143 | |
| Male gender | 55 (88.7) | 20 (90.9) | 1.000 | 15 (88.2) | 16 (94.1) | 1.000 | |
| Diabetes | 2 (3.2) | 2 (9.1) | 0.280 | 2 (11.8) | 1 (5.9) | 0.209 | |
| Smoking | 26 (41.9) | 9 (40.9) | 1.000 | 8 (47.1) | 7 (41.2) | 1.000 | |
| Hypertension | 39 (62.9) | 18 (81.8) | 0.119 | 16 (94.1) | 14 (82.4) | 0.601 | |
| CVD | 2 (3.2) | 1 (4.5) | 1.000 | 1 (5.9) | 0 (0.0) | 1.000 | |
| Hyperlipidemia | 16 (25.8) | 7 (31.8) | 0.589 | 5 (29.4) | 3 (17.6) | 0.280 | |
| BMI (median (IQR)) | 25.1 (23.3, 27.8) | 27.8 (25.9, 30.7) | 0.008 | 26.5 (24.6, 30.4) | 27.1 (24.7, 29.3) | 0.953 | |
| Pulmonary hypertension 1 | 3 (4.8) | 0 (0.0) | 0.563 | 0 (0.0) | 0 (0.0) | NA | |
| Renal impairment | 10 (16.1) | 6 (27.3) | 0.343 | 7 (41.2) | 5 (29.4) | 0.721 | |
| NYHA | |||||||
| I | 36 (58.1) | 9 (40.9) | 0.215 | 9 (52.9) | 6 (35.3) | 0.491 | |
| II | 21 (33.9) | 8 (36.4) | 1.000 | 6 (35.3) | 6 (35.3) | 1.000 | |
| III | 5 (8.1) | 5 (22.7) | 0.118 | 2 (11.8) | 5 (29.4) | 0.398 | |
| LVEF (%)(median (IQR)) 1 | 55 (51, 60) | 59 (50, 60) | 0.588 | 55 (53, 61) | 59 (50, 60) | 0.968 | |
| Previous MI | 1 (1.6) | 0 (0.0) | 1.000 | 1 (5.9) | 0 (0.0) | 1.000 | |
| Previous PCI | 0 (0.0) | 1 (4.5) | 0.262 | 0 (0.0) | 1 (5.9) | 0.354 | |
| Aortic disease | |||||||
| AV stenosis | 2 (3.2) | 0 (0.0) | 1.000 | 1 (5.9) | 0 (0.0) | 0.354 | |
| AV insufficiency | 52 (83.9) | 22 (100.0) | 0.057 | 14 (82.4) | 17 (100.0) | 0.227 | |
| Bicuspid aortic valve | 27 (43.5) | 1 (4.5) | 0.001 | 3 (17.6) | 1 (5.9) | 0.601 | |
| Sternotomy-VSARR (17) | Mini-VSARR (17) | Pvalue | |
|---|---|---|---|
| CPB time (median (IQR)) | 166 (157, 177) | 226 (220, 239) | <0.001 |
| Aortic cross clamp (median (IQR)) | 140 (136, 147) | 160 (158, 171) | <0.001 |
| In-hospital mortality | 0 (0.0) | 0 (0.0) | NA |
| Cardiac tamponade and/or rethoracotomy for bleeding | 3 (17.6) | 2 (11.8) | 1.000 |
| Postoperative drainage (mL) (median (IQR)) | 845 (588, 1393) | 740 (485, 1020) | 0.651 |
| Periprocedural MI | 0 (0.0) | 1 (5.9) | 1.000 |
| Respiratory failure | 0 (0.0) | 1 (5.9) | 1.000 |
| Neurologic complications | 0 (0.0) | 0 (0.0) | NA |
| Multiorgan failure | 0 (0.0) | 1 (5.9) | 1.000 |
| Acute kidney failure and/or dialysis | 0 (0.0) | 1 (5.9) | 1.000 |
| Sternal wound infection | 0 (0.0) | 1 (5.9) | 1.000 |
| ECMO | 0 (0.0) | 1 (5.9) | 1.000 |
| IABP | 0 (0.0) | 0 (0.0) | NA |
| HLoS (median (IQR)) | 9.50 (8.00, 11.00) | 6.52 (4.92, 9.35) | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staromłyński, J.; Kowalówka, A.; Gocoł, R.; Hudziak, D.; Żurawska, M.; Nowak, W.; Pasierski, M.; Sarnowski, W.; Smoczyński, R.; Bartczak, M.; et al. Comparative Analysis of Long-Term Outcomes in Valve-Sparing Aortic Root Reimplantation: Full Sternotomy versus Mini-Sternotomy Approach. J. Clin. Med. 2024, 13, 2692. https://doi.org/10.3390/jcm13092692
Staromłyński J, Kowalówka A, Gocoł R, Hudziak D, Żurawska M, Nowak W, Pasierski M, Sarnowski W, Smoczyński R, Bartczak M, et al. Comparative Analysis of Long-Term Outcomes in Valve-Sparing Aortic Root Reimplantation: Full Sternotomy versus Mini-Sternotomy Approach. Journal of Clinical Medicine. 2024; 13(9):2692. https://doi.org/10.3390/jcm13092692
Chicago/Turabian StyleStaromłyński, Jakub, Adam Kowalówka, Radosław Gocoł, Damian Hudziak, Małgorzata Żurawska, Wojciech Nowak, Michał Pasierski, Wojciech Sarnowski, Radosław Smoczyński, Maciej Bartczak, and et al. 2024. "Comparative Analysis of Long-Term Outcomes in Valve-Sparing Aortic Root Reimplantation: Full Sternotomy versus Mini-Sternotomy Approach" Journal of Clinical Medicine 13, no. 9: 2692. https://doi.org/10.3390/jcm13092692
APA StyleStaromłyński, J., Kowalówka, A., Gocoł, R., Hudziak, D., Żurawska, M., Nowak, W., Pasierski, M., Sarnowski, W., Smoczyński, R., Bartczak, M., Brączkowski, J., Sadecka, S., Drobiński, D., Deja, M., Szymański, P., Suwalski, P., & Kowalewski, M. (2024). Comparative Analysis of Long-Term Outcomes in Valve-Sparing Aortic Root Reimplantation: Full Sternotomy versus Mini-Sternotomy Approach. Journal of Clinical Medicine, 13(9), 2692. https://doi.org/10.3390/jcm13092692