
Second Versus First Molar Extractions in Class II Division 1 Malocclusion Treatment: A Retrospective Longitudinal Outcome Study into Maxillary Canine, Premolar, and Molar Movement


 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size
2.3. Treatment
2.3.1. M1 Group (Extraction of Maxillary First Molars)
2.3.2. M2 Group (Extraction of Maxillary Second Molars)
2.4. Data Collection
2.5. Variables
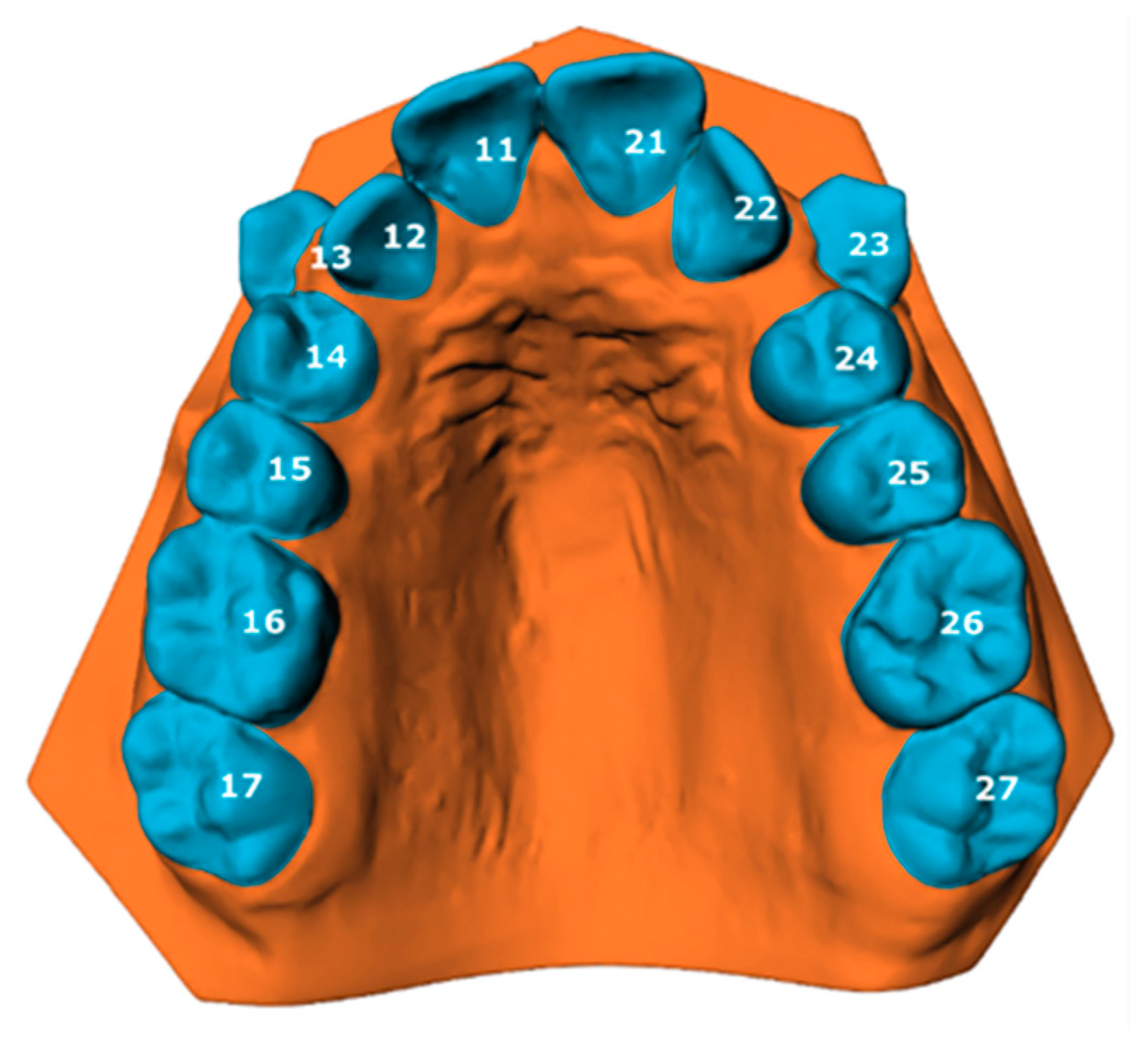
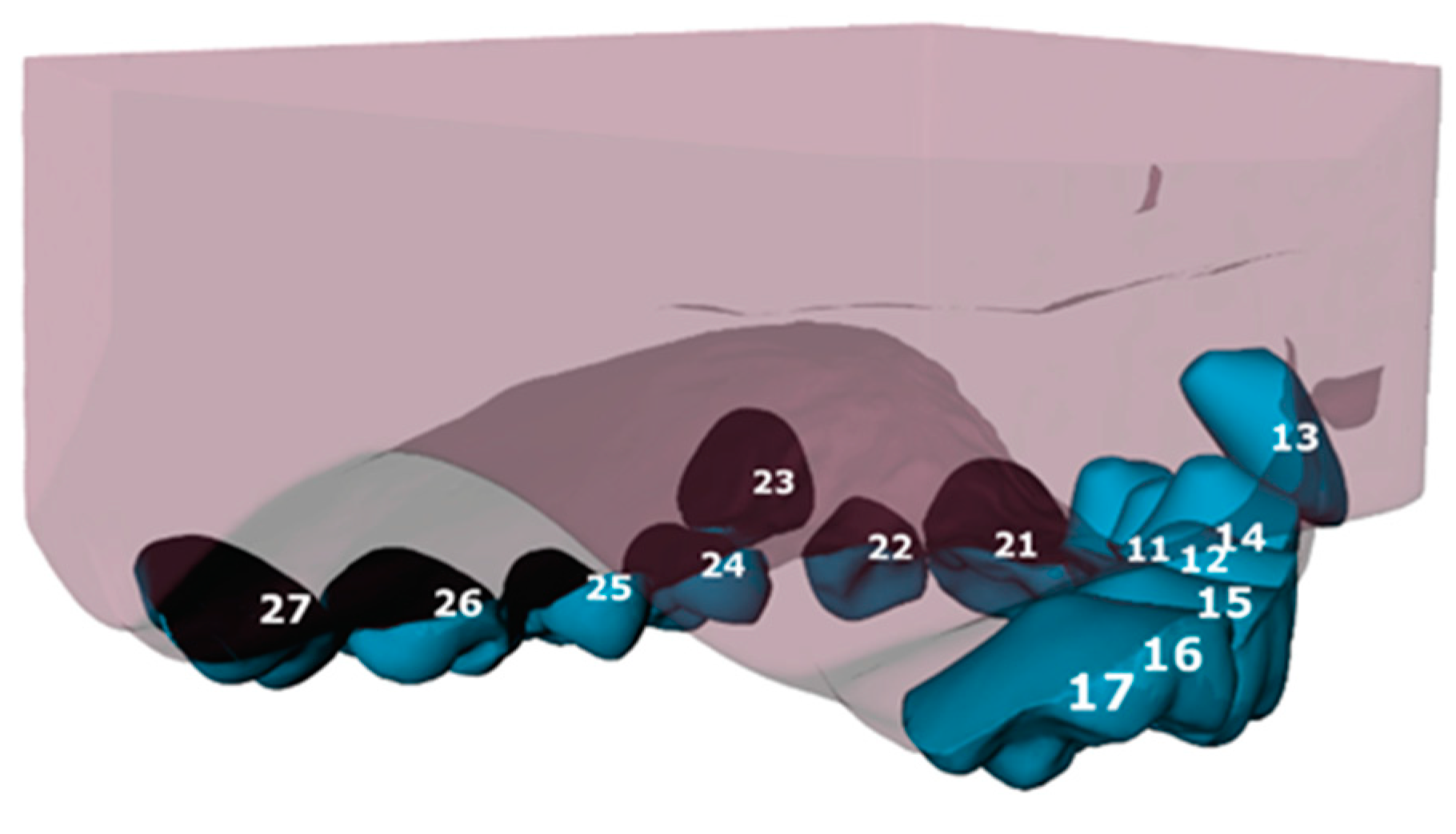
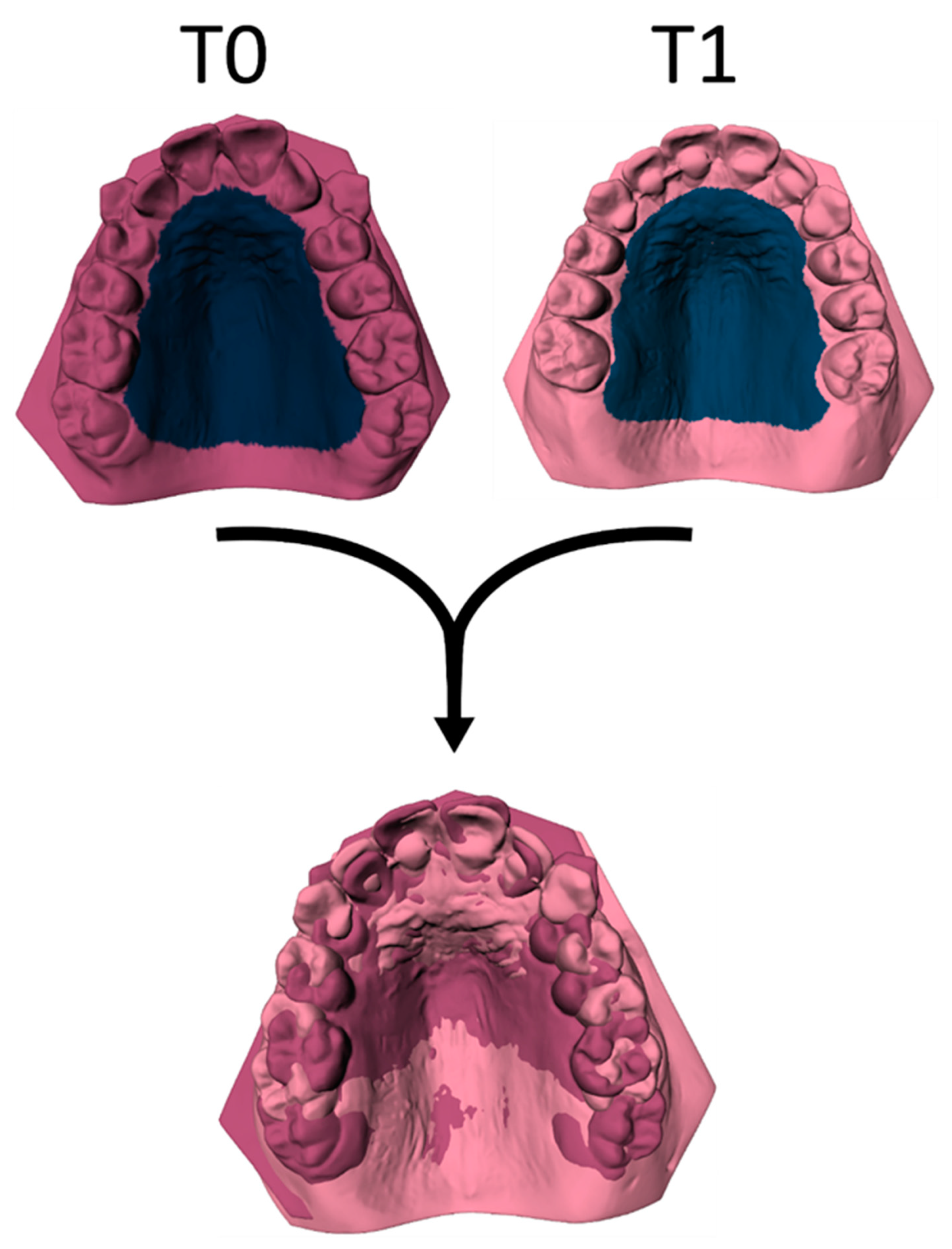
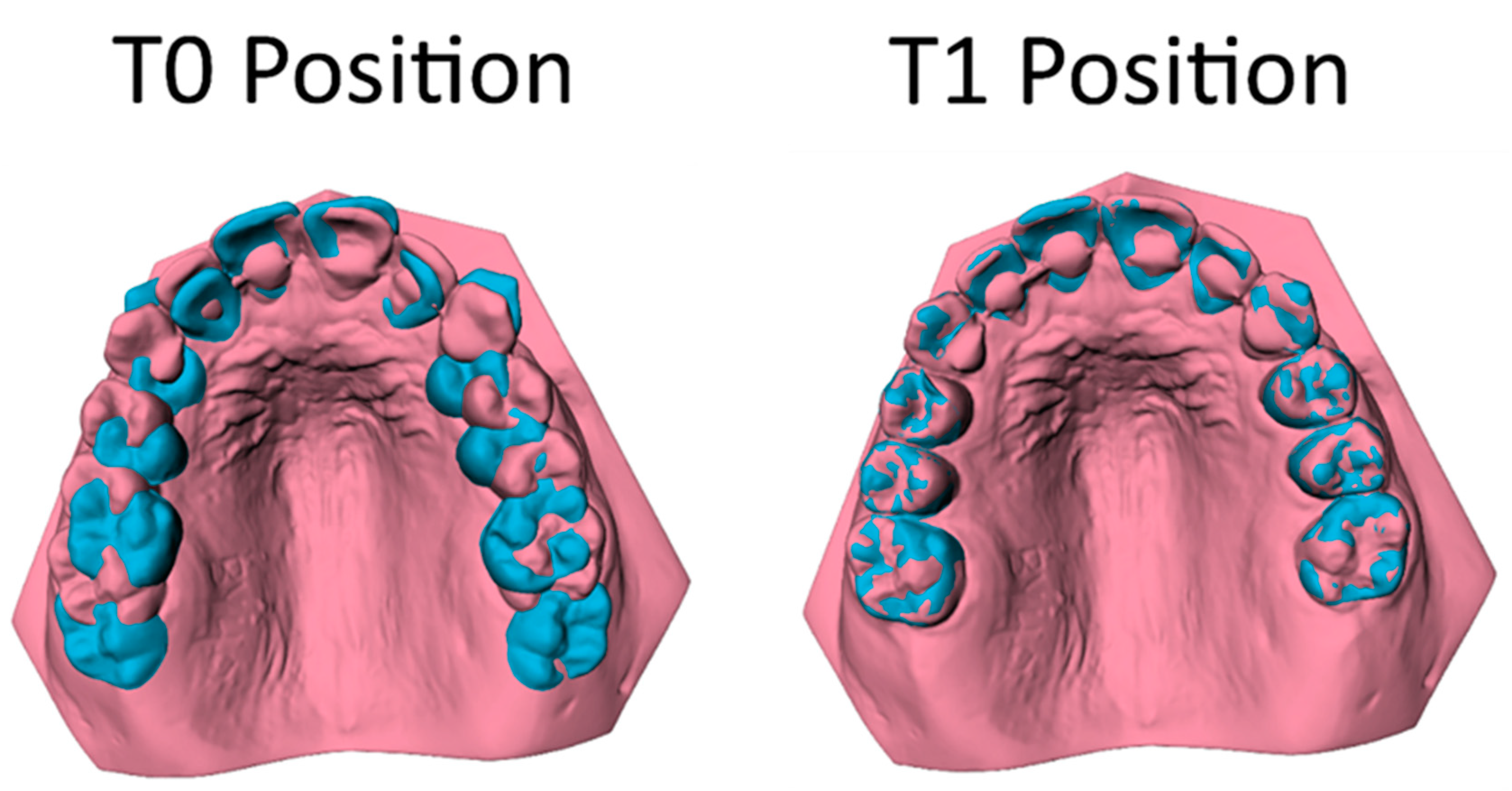
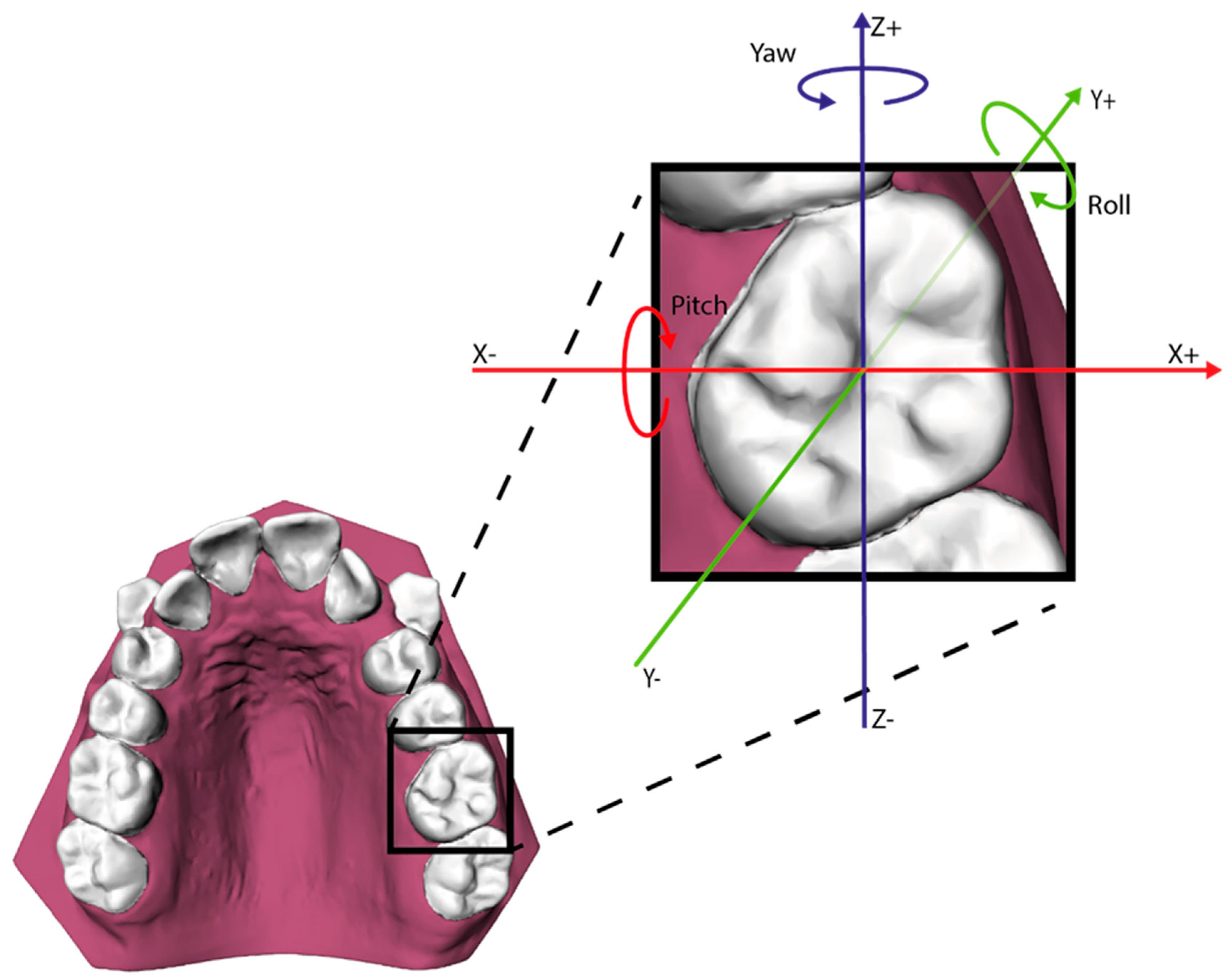
Three-Dimensional Tooth Movement
2.6. Statistical Analysis
3. Results
3.1. Sample Descriptives
3.2. Reliability of the Method
3.3. Tooth Movement
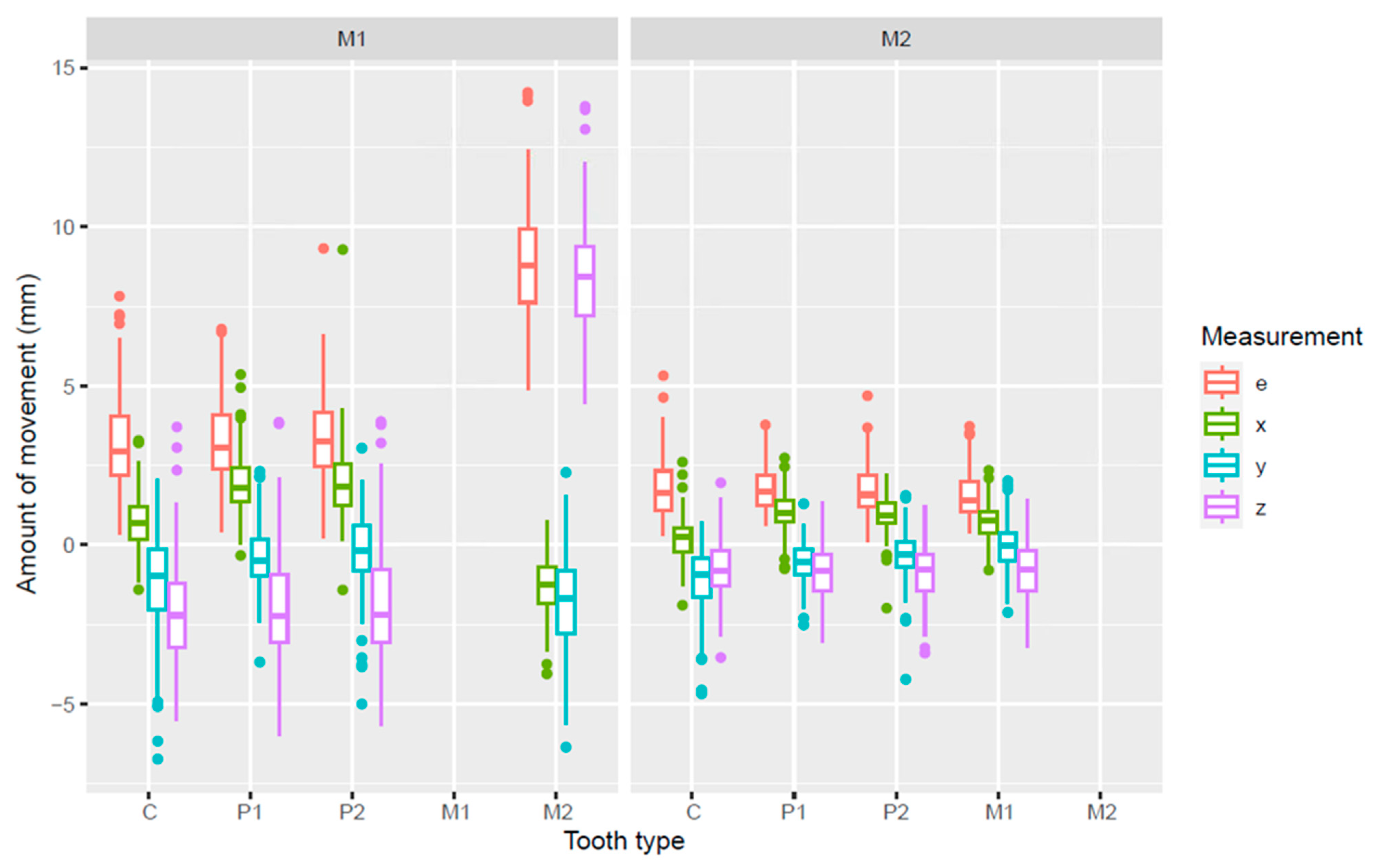
3.4. Three-Dimensional Measurements Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Proffit, W.R.; Fields, H.W., Jr.; Larson, B. Contemporary Orthodontics, 6th ed.; Elsevier: Philadelphia, PA, USA, 2018; pp. 140–202. [Google Scholar]
- Thiruvenkatachari, B.; Harrison, J.E.; Worthington, H.V.; O’Brien, K. Early Orthodontic Treatment for Class II Malocclusion Reduces the Chance of Incisal Trauma: Results of a Cochrane Systematic Review. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Evrard, A.; Tepedino, M.; Cattaneo, P.M.; Cornelis, M.A. Which factors influence orthodontists in their decision to extract? A questionnaire survey. J. Clin. Exp. Dent. 2019, 11, e432–e438. [Google Scholar] [CrossRef]
- Alsaggaf, D.H.; Afify, A.R.; Zawawi, K.H.; Alsulaimani, F.F. Factors influencing the orthodontic treatment plan in Class II malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 829–837.e1. [Google Scholar] [CrossRef] [PubMed]
- Trevisi, H.; Trevisi Zanelato, R. State-of-the-Art Orthodontics, Self-Ligation Appliances, Miniscrews and Second Molar Extractions; Elsevier: Philadelphia, PA, USA, 2018; pp. 156–223. [Google Scholar]
- Konstantonis, D.; Vasileiou, D.; Papageorgiou, S.N.; Eliades, T. Soft Tissue Changes Following Extraction vs. Nonextraction Orthodontic Fixed Appliance Treatment: A Systematic Review and Meta-analysis. Eur. J. Oral. Sci. 2018, 126, 167–179. [Google Scholar] [CrossRef]
- Raposo, R.; Peleteiro, B.; Paço, M.; Pinho, T. Orthodontic camouflage versus orthodontic-orthognathic surgical treatment in Class II malocclusion: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2018, 47, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Janson, M.; Nakamura, A.; de Freitas, M.R.; Henriques, J.F.; Pinzan, A. Influence of cephalometric characteristics on the occlusal success rate of Class II malocclusions treated with 2- and 4-premolar extraction protocols. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 861–868. [Google Scholar] [CrossRef]
- Atik, E.; Akarsu-Guven, B.; Kocadereli, I. Soft tissue effects of three different Class II/1-camouflage treatment strategies. J. Orofac. Orthop. 2017, 78, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Mendes, L.M.; Junqueira, C.H.; Garib, D.G. Soft-tissue changes in Class II malocclusion patients treated with extractions: A systematic review. Eur. J. Orthod. 2016, 38, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.W.; Kuijpers-Jagtman, A.M.; Bronkhorst, E.M.; Livas, C.; Ren, Y.; Kuijpers, M.A.R.; Katsaros, C. Class II Division 1 Malocclusion Treatment with Extraction of Maxillary First Molars: Evaluation of Treatment and Post-treatment Changes by the PAR Index. Orthod. Craniofac. Res. 2021, 24, 102–110. [Google Scholar] [CrossRef]
- Jacobs, C.; Jacobs-Müller, C.; Luley, C.; Erbe, C.; Wehrbein, H. Orthodontic space closure after first molar extraction without skeletal anchorage. J. Orofac. Orthop. 2011, 72, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.W.; Goeke, J.; Bronkhorst, E.M.; Pancherz, H.; Ruf, S.; Katsaros, C. Overjet Correction and Space Closure Mechanisms for Class II Treatment by Extracting the Maxillary First Molars. J. Orofac. Orthop. 2011, 72, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.W.; Serafin, M.; Fastuca, R.; Kuijpers-Jagtman, A.M.; Caprioglio, A. Skeletal, dental and soft tissue cephalometric changes after orthodontic treatment of dental Class II malocclusion with maxillary first molar or first premolar extractions. J. Clin. Med. 2022, 11, 3170. [Google Scholar] [CrossRef]
- Waters, D.; Harris, E.F. Cephalometric Comparison of Maxillary Second Molar Extraction and Nonextraction Treatments in Patients with Class II Malocclusions. Am. J. Orthod. Dentofac. Orthop. 2001, 120, 608–677. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Wong, R.W.-K.; Ikegami, T.; Hägg, U. Maxillary Second Molar Extractions in Orthodontic Treatment. World J. Orthod. 2008, 9, 52–61. [Google Scholar] [PubMed]
- De Freitas, M.R.; De Lima, D.V.; De Freitas, K.M.S.; Janson, G.; Henriques, J.F.C. Strategic Maxillary Second-Molar Extraction in Class II Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 878–886. [Google Scholar] [CrossRef]
- Basdra, E.K.; Stellzig, A.; Komposch, G. Extraction of Maxillary Second Molars in the Treatment of Class II Malocclusion. Angle Orthod. 1996, 66, 287–292. Available online: https://www.umcg.nl/-/afdeling/orthodontie (accessed on 13 December 2023).
- Paddenberg, E.; Braun, M.C.; Proff, P.; Lippold, C.; Kirschneck, C. Comparative Treatment Outcomes after Bilateral Extractions of Maxillary Second Molars or First Premolars in Patients with Class II Malocclusion: A Retrospective Study. Head Face Med. 2023, 19, 5. [Google Scholar] [CrossRef] [PubMed]
- Batista, K.B.S.L.; Thiruvenkatachari, B.; Harrison, J.E.; O’Brien, K. Orthodontic Treatment for Prominent Upper Front Teeth (Class II Malocclusion) in Children and Adolescents. Cochrane Database Syst. Rev. 2018, 3, CD003452. [Google Scholar] [CrossRef]
- Maspero, C.; Galbiati, G.; Giannini, L.; Guenza, G.; Farronato, M. Class II Division 1 Malocclusions: Comparisons between One- and Two-Step Treatment. Eur. J. Paediatr. Dent. 2018, 19, 295–299. [Google Scholar] [CrossRef]
- Ganzer, N.; Feldmann, I.; Liv, P.; Bondemark, L. A novel method for superimposition and measurements on maxillary digital 3D models-studies on validity and reliability. Eur. J. Orthod. 2018, 40, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Koh, K.M.; Choi, S.H.; Kim, J.H.; Cha, J.Y. Validation of three-dimensional digital model superimpositions based on palatal structures in patients with maximum anterior tooth retraction following premolar extraction. Korean J. Orthod. 2022, 52, 258–267. [Google Scholar] [CrossRef]
- Zhang, L.; Guo, R.; Xu, B.; Wang, Y.; Li, W. Three-dimensional evaluation of maxillary tooth movement in extraction patients with three different miniscrew anchorage systems: A randomized controlled trial. Progr. Orthod. 2022, 23, 46. [Google Scholar] [CrossRef]
- Schmitz, J.; Keilig, L.; Daratsianos, N.; Bourauel, C. Superimposition of dental models to determine orthodontic tooth movements: Comparison of different superimposition methods in vitro and in vivo. J. Orofac. Orthop. 2024; ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Haque, S.; Sandler, J.; Cobourne, M.T.; Bassett, P.; DiBiase, A.T. A retrospective study comparing the loss of anchorage following the extraction of maxillary first or second premolars during orthodontic treatment with fixed appliances in adolescent patients. J. Orthod. 2017, 44, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.W.; Kuijpers-Jagtman, A.M.; Katsaros, C. A treatment method for Class II Division 1 patients with extraction of permanent maxillary first molars. World J. Orthod. 2009, 10, 41–48. [Google Scholar]
- Pancherz, H. The Mechanism of Class II Correction in Herbst Appliance Treatment. A Cephalometric Investigation. Am. J. Orthod. 1982, 82, 104–113. [Google Scholar] [CrossRef]
- Hamza, B.; Papageorgiou, S.N.; Patcas, R.; Schätzle, M. Spontaneous space closure after extraction of permanent first molars in children and adolescents: A systematic review and meta-analysis. Eur. J. Orthod. 2024, 46, cjae054. [Google Scholar] [CrossRef]
- Kılınç, D.D.; Sayar, G. Various Contemporary Intraoral Anchorage Mechanics Supported with Temporary Anchorage Devices. Turk. J. Orthod. 2016, 29, 109–113. [Google Scholar] [CrossRef]
- Schroeder, M.A.; Schroeder, D.K.; Santos, D.J.S.; Leser, M.M. Molar extractions in orthodontics. Dent. Press. J. Orthod. 2011, 16, 130–157. [Google Scholar] [CrossRef]
- Bayome, M.; Park, J.H.; Bay, C.; Kook, Y.A. Distalization of maxillary molars using temporary skeletal anchorage devices: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2021, 24 (Suppl. S1), 103–112. [Google Scholar] [CrossRef] [PubMed]
- Staley, R.N.; Stuntz, W.R.; Peterson, L.C. A Comparison of Arch Widths in Adults with Normal Occlusion and Adults with Class II, Division 1 Malocclusion. Am. J. Orthod. 1985, 88, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Abbing, A.; Koretsi, V.; Eliades, T.; Papageorgiou, S.N. Duration of orthodontic treatment with fixed appliances in adolescents and adults: A systematic review with meta-analysis. Progr. Orthod. 2020, 21, 37. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Groups | |||||
|---|---|---|---|---|---|---|
| M1 Extraction (n = 98) | M2 Extraction (n = 64) | |||||
| Mean | SD | Range | Mean | SD | Range | |
| Age T0 (years) | 13.20 | 1.46 | 10.50–17.20 | 13.20 | 1.36 | 10.30–16.30 |
| Age T1 (years) | 15.70 | 1.58 | 12.40–19.80 | 14.70 | 1.45 | 11.30–18.10 |
| Treatment duration (years) | 2.51 | 0.55 | 1.36–4.49 | 1.53 | 0.37 | 0.82–2.64 |
| DME | PCC | Mean Diff (mm) | 95% CI (mm) | p | ||
|---|---|---|---|---|---|---|
| Inter | e | 0.44 | 0.96 | −0.13 | −0.21; −0.05 | 0.002 |
| x | 0.21 | 0.98 | 0.04 | 0.00; 0.08 | 0.049 | |
| y | 0.33 | 0.94 | 0.12 | 0.06; 0.18 | <0.001 | |
| z | 0.69 | 0.94 | 0.13 | 0.01; 0.26 | 0.038 | |
| Intra | e | 0.08 | 1.00 | −0.02 | −0.04; −0.00 | 0.019 |
| x | 0.05 | 1.00 | 0.00 | −0.01; 0.01 | 0.637 | |
| y | 0.13 | 0.99 | 0.01 | −0.01; 0.04 | 0.246 | |
| z | 0.06 | 1.00 | 0.01 | −0.00; 0.02 | 0.181 | |
| M1 Extraction Group | M2 Extraction Group | ||||||
|---|---|---|---|---|---|---|---|
| Tooth Type | Axis | Mean (mm) | SD (mm) | [Min; Max] (mm) | Mean (mm) | SD (mm) | [Min; Max] (mm) |
| C | e | 3.17 | 1.42 | 0.35; 7.82 | 1.82 | 1.03 | 0.27; 5.32 |
| x | 0.73 | 0.88 | −1.41; 3.28 | 0.19 | 0.70 | −1.90; 2.60 | |
| y | −1.26 | 1.60 | −6.72; 2.07 | −1.13 | 1.08 | −4.68; 0.72 | |
| z | −2.09 | 1.52 | −5.51; 3.71 | −0.75 | 0.91 | −3.54; 1.95 | |
| P1 | e | 3.25 | 1.22 | 0.41; 6.78 | 1.76 | 0.70 | 0.61; 3.77 |
| x | 1.89 | 0.86 | −0.33; 5.36 | 1.01 | 0.63 | −0.75; 2.73 | |
| y | −0.41 | 0.98 | −3.68; 2.31 | −0.56 | 0.62 | −2.51; 1.29 | |
| z | −2.01 | 1.61 | −5.99; 3.86 | −0.83 | 0.90 | −3.07; 1.37 | |
| P2 | e | 3.33 | 1.28 | 0.20; 9.32 | 1.75 | 0.75 | 0.11; 4.69 |
| x | 1.91 | 1.05 | −1.42; 9.28 | 0.94 | 0.62 | −1.99; 2.21 | |
| y | −0.16 | 1.20 | −5.00; 3.04 | −0.37 | 0.80 | −4.23; 1.55 | |
| z | −1.95 | 1.66 | −5.69; 3.88 | −0.83 | 0.95 | −3.40; 1.26 | |
| M1 | e | - | - | - | 1.59 | 0.75 | 0.38; 3.73 |
| x | - | - | - | 0.72 | 0.61 | −0.79; 2.34 | |
| y | - | - | - | −0.03 | 0.74 | −2.12; 2.01 | |
| z | - | - | - | −0.83 | 0.98 | −3.24; 1.44 | |
| M2 | e | 8.85 | 1.93 | 4.89; 14.22 | - | - | - |
| x | −1.30 | 0.91 | −4.05; 0.75 | - | - | - | |
| y | −1.77 | 1.51 | −6.35; 2.28 | - | - | - | |
| z | 8.40 | 1.66 | 4.45; 13.78 | - | - | - | |
| Tooth Type | Axis | Estimate (mm) | 95% CI (mm) | p |
|---|---|---|---|---|
| C | e | −1.30 | −1.66; −0.93 | <0.001 |
| x | −0.54 | −0.74; −0.33 | <0.001 | |
| y | 0.11 | −0.29; 0.51 | 0.587 | |
| z | 1.24 | 0.86; 1.61 | <0.001 | |
| P1 | e | −1.48 | −1.74; −1.21 | <0.001 |
| x | −0.87 | −1.08; −0.67 | <0.001 | |
| y | −0.15 | −0.36; 0.07 | 0.196 | |
| z | 1.14 | 0.77; 1.52 | <0.001 | |
| P2 | e | −1.58 | −1.87; −1.30 | <0.001 |
| x | −0.93 | −1.18; −0.57 | <0.001 | |
| y | −0.20 | −0.50; 0.10 | 0.201 | |
| z | 1.11 | 0.70; 1.51 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oostenbrink, A.H.A.; Bronkhorst, E.M.; Booij, J.W.; Dieters, A.J.A.; Ren, Y.; Kuijpers-Jagtman, A.M.; Bruggink, R. Second Versus First Molar Extractions in Class II Division 1 Malocclusion Treatment: A Retrospective Longitudinal Outcome Study into Maxillary Canine, Premolar, and Molar Movement. J. Clin. Med. 2025, 14, 225. https://doi.org/10.3390/jcm14010225
Oostenbrink AHA, Bronkhorst EM, Booij JW, Dieters AJA, Ren Y, Kuijpers-Jagtman AM, Bruggink R. Second Versus First Molar Extractions in Class II Division 1 Malocclusion Treatment: A Retrospective Longitudinal Outcome Study into Maxillary Canine, Premolar, and Molar Movement. Journal of Clinical Medicine. 2025; 14(1):225. https://doi.org/10.3390/jcm14010225
Chicago/Turabian StyleOostenbrink, Akkelien H. A., Ewald M. Bronkhorst, Johan W. Booij, Arjan J. A. Dieters, Yijin Ren, Anne Marie Kuijpers-Jagtman, and Robin Bruggink. 2025. "Second Versus First Molar Extractions in Class II Division 1 Malocclusion Treatment: A Retrospective Longitudinal Outcome Study into Maxillary Canine, Premolar, and Molar Movement" Journal of Clinical Medicine 14, no. 1: 225. https://doi.org/10.3390/jcm14010225
APA StyleOostenbrink, A. H. A., Bronkhorst, E. M., Booij, J. W., Dieters, A. J. A., Ren, Y., Kuijpers-Jagtman, A. M., & Bruggink, R. (2025). Second Versus First Molar Extractions in Class II Division 1 Malocclusion Treatment: A Retrospective Longitudinal Outcome Study into Maxillary Canine, Premolar, and Molar Movement. Journal of Clinical Medicine, 14(1), 225. https://doi.org/10.3390/jcm14010225