Abstract
Background: Prone positioning is a standard intervention in managing patients with severe acute respiratory distress syndrome (ARDS) and is known to improve oxygenation. However, its effects on other organs, particularly the kidneys, are less well understood. This study aimed to assess the association between prone positioning and the development of acute kidney injury (AKI), specifically in overweight and obese patients. Methods: A retrospective pre–post study was conducted on a cohort of 60 critically ill ARDS patients who were placed in the prone position during hospitalization. The development of AKI was assessed using the Acute Kidney Injury Network (AKIN) criteria, with AKI measured by both creatinine levels (AKINCr) and urine output (AKINUO). Patients were divided into two groups based on body mass index (BMI): overweight/obese (BMI ≥ 25) and non-obese (BMI < 25). Data were collected before and after prone positioning. Results: In overweight/obese patients (n = 39, 57 cases), both the median AKINCr and AKINUO scores increased significantly following prone positioning (from 0 to 1, median p < 0.01, and from 0 to 2, median p < 0.01, respectively). No statistically significant changes in AKIN scores were observed in non-obese patients nor were significant differences found in either group after repositioning to supine. Conclusions: Prone positioning is associated with an increased risk of acute kidney injury in overweight and obese ARDS patients. This may be due to the kidneys’ susceptibility to intra-abdominal hypertension in these patients. Further research is needed to explore optimal proning strategies for overweight and obese populations.
1. Introduction
Acute respiratory distress syndrome (ARDS) is a clinical condition characterized by acute, diffuse inflammatory lung injury leading to respiratory failure, affecting approximately 10% of all intensive care unit (ICU) admissions [1]. Current ARDS management guidelines recommend prone positioning as a therapeutic intervention, showing a significant mortality benefit [2]. The landmark PROSEVA randomized controlled trial demonstrated that prone positioning for at least 16 h per day in patients with moderate-to-severe ARDS significantly reduced both 28-day and 90-day mortality, as well as the incidence of cardiac arrests [3]. Prone positioning improves oxygenation by reducing intrapulmonary shunting, decreasing ventilation–perfusion mismatch, and preventing ventilator-induced lung injury by distributing mechanical stress and strain more evenly throughout the lung tissue [4].
The COVID-19 pandemic has drawn further attention to this treatment approach, leading to a global increase in proning practices. COVID-19 patients with ARDS who were placed in the prone position showed significant improvements in oxygenation [5,6], with benefits comparable to those seen in non-COVID-19 ARDS patients, even in non-ICU settings [7]. Much of the benefit from prone positioning is attributed to the redistribution of the weight of the heart and abdominal organs away from the lungs, reducing atelectasis [8].
Gong et al. previously reported a positive association between body mass index (BMI) and the risk of developing ARDS [9]. The global rise in obesity prevalence, along with the increasing frequency of ICU admissions for obese patients, makes this association a critical area of ARDS research [10,11,12]. Obese patients tend to experience greater morbidity during ICU admission [12,13,14]. Outcomes in ARDS are significantly worsened when extra-pulmonary multi-organ failure develops, particularly renal failure [15]. The association between acute kidney injury (AKI) and poor outcomes is well documented [16,17]. Furthermore, patients who develop AKI during ICU admission have a significantly increased risk of long-term mortality, extending to at least two years post discharge [18]. Similar to ARDS, the incidence of AKI is substantially higher among critically ill obese patients [19,20,21,22].
Known risks associated with prone positioning include hemodynamic changes, hypoperfusion, ophthalmic injury, and compartment syndrome [23]. Several studies have explored the potential association between prone positioning and organ failure [24,25,26]; however, no definitive conclusions have been reached regarding the relationship between prone positioning and the development of renal failure.
Given the established risks of both ARDS and AKI, particularly in obese patients, we aimed to determine whether prone positioning in ARDS patients is associated with the development of AKI.
2. Materials and Methods
2.1. Study Population
This retrospective pre–post study design used each patient as their own control, comparing data before (“pre proning”) and after (“post proning”) the intervention. The intervention was defined as changing the patient’s position from supine to prone or vice versa. This study was conducted at Soroka University Medical Center (SUMC), a tertiary care academic medical center in southern Israel. The cohort included all patients with moderate-to-severe ARDS who were admitted to the ICU between January 2010 and October 2021, all of whom were under mechanical ventilation and underwent prone positioning during their hospital stay. ARDS was diagnosed based on the Berlin criteria [27]. This study was approved by the Institutional Review Board (IRB) (protocol code SCRC20017) with a waiver of informed consent.
The criteria for prone positioning followed ARDS guidelines, as established by the PROSEVA trial (p ratio < 150), but decisions regarding whether to prone a patient were made in real time at the treating physician’s discretion. Patients were excluded from the analysis if they received any diuretic drugs within six hours before or after proning or if they had renal failure requiring renal replacement therapy (RRT). This exclusion criterion applied both to patients with chronic end-stage renal disease on dialysis prior to their ARDS diagnosis and those with acute renal failure requiring new RRT. Both continuous forms of RRT (e.g., continuous veno-venous hemodiafiltration) and conventional hemodialysis were considered exclusionary forms of RRT.
2.2. Data Collection
We screened the institutional electronic medical records to identify ICU patients hospitalized during the study period with an ICD-9 diagnosis of ARDS who were placed in the prone position at least once during their hospital stay. Data were manually extracted through chart review. Collected variables included the following:
- Patient demographics: gender, age, comorbidities, and BMI.
- ICU-related data: length of stay, vital signs, vasopressor requirements, concurrent medications, use of diuretics, hourly urine output, and levels of creatinine, urea, and lactate.
Measurements were recorded 24 h before and 24 h after a change in patient position, either from supine to prone or from prone back to supine. Baseline creatinine was defined as the lowest value recorded during the year prior to proning. If no previous records were available, the lowest creatinine value from the current hospitalization was used.
The severity of illness was assessed using the Sequential Organ Failure Assessment (SOFA) score [28]. In addition, pre- and post-proning blood pressure, vasopressor dose, and lactate levels were collected to account for potential hemodynamic confounders that could contribute to AKI development.
AKI severity was measured 24 h before and after intervention using the Acute Kidney Injury Network (AKIN) classification, which categorizes AKI into three stages based on changes in serum creatinine and urine output:
- Stage 1: serum creatinine increase of at least 1.5 times baseline or absolute increase of 0.3 mg/dL (AKINCr 1) or urine output < 0.5 mL/kg/h for 6–12 h (AKINUO 1).
- Stage 2: serum creatinine increase of 2.0 times baseline (AKINCr 2) or urine output < 0.5 mL/kg/h for over 12 h (AKINUO 2).
- Stage 3: serum creatinine increase of at least three times baseline, serum creatinine of 4.0 mg/dL or higher (AKINCr 3), initiation of renal replacement therapy, urine output < 0.3 mL/kg/h for 24 h, or anuria for 12 h (AKINUO 3) [29,30,31].
The estimated glomerular filtration rate (eGFR) was then calculated using the Salazar–Corcoran equation, which was developed to estimate the eGFR in obese patients by taking into account the patient’s weight and height [32,33].
2.3. Statistical Analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics, baseline laboratory values, and development of AKI before and after a change in patient position. The Wilcoxon signed-rank test was used to compare pre and post continuous variables. Logistic regression was used to assess the association between prone position and AKI development, with odds ratios and 95% confidence intervals reported. AKI development was the dependent variable in the regression model. Statistical significance was set at p < 0.05. All analyses were performed using R software.
3. Results
3.1. General Information
A total of 60 patients were admitted to the ICU at SUMC between January 2010 and October 2021 with a diagnosis of moderate-to-severe ARDS and were placed in the prone position during their hospital stay. Patients who underwent RRT within 24 h before or after proning (n = 2), and those who received diuretics within six hours of pronation (n = 2), were excluded from this study. The remaining 56 patients comprised the study population and were included in the analysis (Figure 1). The cohort was predominantly male (71%, n = 40), with a median age of 59 years and a mean BMI of 33 (range 20 to 52). Thirty-nine patients (70%) were diagnosed with COVID-19 infection. The mean baseline creatinine was 0.79 mg/dL, the median PaO2/FiO2 before proning was 64, and the pre-proning SOFA score had a median of 8 (Table 1). Detailed patient baseline comorbidities are shown in the Supplementary Materials: Table S1. Thirty-nine patients died during their ICU stay, and five additional patients died within six months of ICU discharge. The average ICU length of stay was 27.73 days.
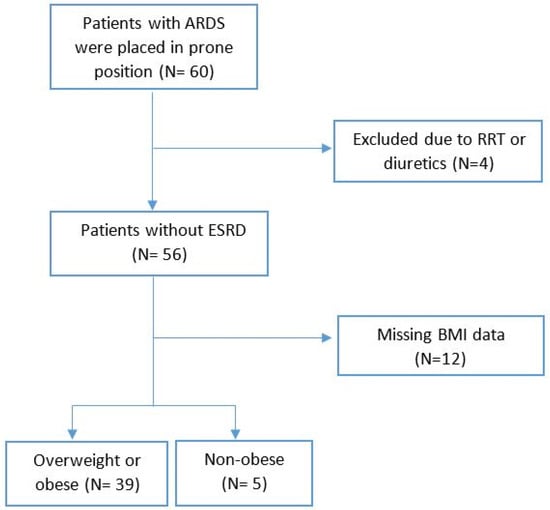
Figure 1.
Flow chart for outcome analysis. A total of 56 patients with acute respiratory distress syndrome (ARDS) who were placed in prone position were included in the first analysis, then grouped by body mass index (BMI) level. ESRD = end-stage renal disease; RRT = renal replacement therapy.

Table 1.
Baseline patient characteristics.
In the cohort of 56 patients, there were 86 distinct supine-to-prone positioning episodes (“proning”) conducted as part of ARDS management. A total of 34% of the cohort (n = 19) required multiple periods in the prone position during their hospital stay. Of the 86 proning episodes, only 59 corresponding supination maneuvers (i.e., returning the patient from prone to supine) were included in the data analysis. Patients were excluded from the supination analysis due to the need for RRT, concurrent diuretic administration, or death while in the prone position, accounting for the discrepancy in the number of proning and supination episodes available for analysis.
The duration of time that patients remained in the prone position varied based on the discretion of the treating physician, with a mean duration of 65 h and 14 min and a median duration of 48 h and 30 min. This extended time in the prone position was attributed to the gradual integration of the PROSEVA trial recommendations, as well as the high proportion of COVID-19 patients in the cohort. The large number of ventilated patients during the COVID-19 pandemic, restrictions on healthcare worker exposure to infected patients, and the low caregiver-to-patient ratio made frequent position changes difficult, preventing adherence to the 16 h goal for supination, as recommended by the PROSEVA study.
Table S2 in the Supplementary Materials presents the laboratory results collected before and after both proning and supination maneuvers, with the most abnormal level measured within 24 h after the change in position reported. The mean lactate level increased significantly after proning, rising from 2.17 mmol/L to 3.24 mmol/L (p < 0.01). A similar significant increase was observed following supination, with lactate levels increasing from a mean of 1.78 mmol/L to 2.64 mmol/L (p < 0.01). There were no significant changes in the mean arterial pressure (MAP) or vasopressor requirements within 24 h after either pronation or supination. Additionally, the SOFA score did not show any significant changes (Supplementary materials: Table S3).
After pronation maneuvers, the mean creatinine level increased significantly from 0.98 mg/dL to 1.26 mg/dL within 24 h of proning (p < 0.01). A similar significant trend was seen in serum urea, which increased from a mean of 73 mg/dL to 86 mg/dL within 24 h of proning (p < 0.01). Following supination, no significant change in creatinine was observed (1.09 mg/dL to 1.1 mg/dL, p = 0.11). However, serum urea levels did rise significantly after supination, increasing from a mean of 79 mg/dL to 86 mg/dL (Supplementary Materials: Table S4).
3.2. AKIN Criteria
As mentioned in the Methods, AKIN scores were calculated for all patients based on creatinine (AKINCr) and also on urine output (AKINUO) [29,30,31]. In the overall cohort, the mean AKINCr exhibited a significant increase from 0.53 before transitioning to the prone position to 0.93 after proning. However, given the ordinal nature of the AKIN score, the median AKINCr was also assessed, and no disparities were found, with AKIN 0 (i.e., no AKI) observed both before and after the proning maneuver (measured as worst recorded AKI 24 h post maneuver change, Table 2, p < 0.01). Conversely, a different trend emerged in AKINUO within the overall cohort, with a significant increase from AKIN 0 pre prone to AKIN 1 post prone (Table 3, p < 0.01). When patients were placed in a supine position, no statistically significant differences were detected in the AKIN scores, whether based on creatinine or urine output (Table 2 and Table 3).
Table 2.
Univariate analysis of AKIN criteria based on creatinine (mg/dL), stratified by BMI.
Table 3.
Univariate analysis of AKIN criteria based on urine output (mL/h), stratified by BMI.
3.3. Obesity Subgroup Analysis
Pre-planned subgroup analyses were conducted on the basis of weight and age, focusing exclusively on pronation. Patients were divided according to BMI into the overweight/obese (BMI ≥ 25) and non-obese (BMI < 25) cohorts (Supplementary Materials: Table S5). Within these subgroups, the overweight or obese group included most of the patients, 57 proning events in thirty-nine patients, while the non-obese group included 11 proning events in five patients (Table 2 and Table 3). Eighteen proning events were missing data regarding patient height or weight and so were not included in the pre-planned subgroup analysis. A separate pre-specified subgroup analysis by age was also performed, separating patients into those below 60 years old and above or equal to 60 to see if the results were stratified by age (Supplementary Materials: Tables S6 and S7).
In the subgroup of overweight or obese patients (n = 39 patients, 57 instances of proning), the median AKINCr exhibited a notable increase from AKIN 0 pre prone to AKIN 1 post prone (see Table 2, p < 0.01). However, no statistically significant differences were observed in AKINCr before and after proning for non-obese patients or for the entire cohort when transitioning from prone to supine (Table 2). A similar trend was observed for the AKINUO score. Among obese patients, urine output decreased post proning, and the median AKINUO increased from AKIN 0 to AKIN 2 following proning (median, p < 0.01), while no significant changes were noted in the AKINUO score for non-obese patients (Table 3). The transition from prone to supine did not yield statistically significant alterations in either the AKINCr or AKINUO scores (Table 2 and Table 3).
Additionally, in the obese population, a near-significant reduction in the eGFR was observed following prone positioning, with a mean decrease from 139 to 129 (p = 0.07) (Supplementary Materials: Table S8).
3.4. Age Subgroup Analysis
A separate pre-planned subgroup analysis by age revealed notable differences. When assessing AKINCr, a notable increase in mean AKINCr was evident, rising from 0.46 to 0.85 in patients under 60 years of age and from 0.63 to 1.03 in patients aged 60 or older. Intriguingly, the median AKINCr remained consistently at 0 both before and after the prone position in both age groups. In contrast, the mean AKINUO showed an elevation in both patients under 60 and those over 60 years old (increasing from 0.62 to 0.96 and from 0.74 to 1.58, respectively). However, the median AKINUO significantly ascended from AKIN 0 to AKIN 2 after proning among patients aged 60 or older (median, p < 0.01), whereas among younger patients, AKINUO remained at 0 both before and after transitioning to proning. After returning patients to a supine position, there were no changes in either the median AKINCr or AKINUO in either age group (Supplementary Materials: Tables S6 and S7).
3.5. Multivariable Logistic Regression
A multivariable logistic regression analysis was conducted to predict the occurrence of AKI (as defined by AKIN worsening) after prone positioning, as well as to adjust variables found to be statistically significant in the univariate analysis. The regression model included the patients’ age, lactate level, and position change. The prone position was found to be significantly associated with AKI development (odds ratio 2.38; 95% confidence interval, 1.05–5.36; p = 0.037). Patient age was also associated with AKI (odds ratio 1.04 for each year of life; 95% confidence interval, 11.02–1.07; p < 0.01), while lactate levels did not reach statistical significance (odds ratio 1.25; 95% confidence interval, 0.92–1.71; p = 0.2) (Table 4). A multivariate logistic regression stratified by COVID-19 infection was also conducted, and no significant differences were revealed in post-proning AKI by separating patients into COVID-19 vs. non-COVID-19 ARDS (Supplementary Materials: Table S9).
Table 4.
Multivariate logistic regression model for predicting AKI occurrence after prone position.
3.6. Time to AKI Post Prone
In the overall cohort, the average urine output per hour was lowest at 6 h following pronation (mean of 59 mL/h, p-value < 0.01 when compared to the mean urine output during the 6 hours before pronation), with subsequent gradual improvement (Figure 2). In the overall cohort, 42% (n = 36) of the cases who underwent a proning intervention event demonstrated AKI (as defined by worsening in AKIN criteria, creatinine or UO, by at least one point after prone position) within 24 h of being placed in the prone position. Among the cases where AKI was observed post proning, 55.5% (n = 20 out of 36) had a mean urine output of less than 0.5 milliliters per kilogram per hour during the 24 h post pronation. In 33.33% of these cases (n = 12), AKI was still present prior to the patient’s return to the supine position, emphasizing that the post-proning AKI is often not transient. A comparison of the AKIN score measured after proning and directly before returning the patients to the supine position showed a slight decrease in the mean AKINUO score but no change in the median AKINUO score (Table 5). No significant change was observed in the AKINCr (Supplementary Materials: Table S10).
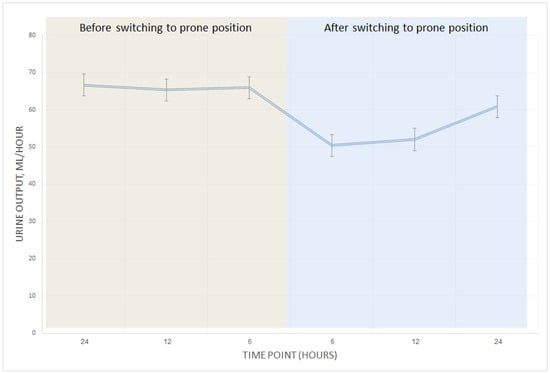
Figure 2.
Average urine output in patients with overweight or obesity before and after prone position. Mean urine output per hour measured 24 h before and after prone position. The lowest urine output among overweight or obese patients was measured six hours post prone position (p < 0.01), then improved gradually. No significant change was observed among non-obese patients; thus, the chart only includes overweight or obese patients.
Table 5.
Univariate analysis of AKIN scores based on urine output (mL/h) at different time points in patients with AKI after prone positioning.
4. Discussion
Our main findings suggest that prone positioning in overweight or obese patients (BMI ≥ 25) treated for ARDS significantly increases the risk of developing AKI, as defined by the AKIN criteria [29]. This effect was observed exclusively in this population, while no similar impact was noted among non-obese patients, regardless of whether AKI was assessed via creatinine levels or urine output. Notably, returning patients to the supine position did not significantly affect AKI occurrence or renal function across any groups, with the exception of a minor rise in urea levels.
We observed that AKI incidence peaked six hours post prone maneuver, with gradual improvement in urine output thereafter. However, a high proportion of patients (55.55%) experienced AKI that persisted for up to 24 h following the prone intervention. Upon repositioning into the supine position, 33.33% of patients still displayed signs of AKI, accompanied by only a slight reduction in their AKINUO scores. These findings suggest that while renal function may begin to recover within hours, prone positioning might exert lasting effects on kidney function in some patients.
Not only did the incidence of AKI worsen following prone positioning among obese patients, but a near-significant reduction in the eGFR (p = 0.07) was also noted exclusively in this group, contrasting with non-obese prone patients where no such trend was observed. Nevertheless, clinicians often rely on AKI and creatinine rise as key markers, with the literature emphasizing creatinine worsening as a significant risk factor for mortality among ICU patients [16].
Patient age was also identified as a significant risk factor for the development of AKI, with a higher risk observed in patients aged 60 years or older. Our findings align with previous studies [34,35], which have shown that elderly patients with AKI face a greater risk of complications [36,37]. However, in multivariate analysis, we found that the prone position maneuver exerted a stronger influence on AKI development compared to age (odds ratio: 2.38 vs. 1.04 per year of life, respectively). Other variables, such as MAP, lactate levels, and SOFA scores, did not show significant changes in either univariate or multivariate analyses.
Prior to the current study, only a few investigations evaluated the negative impact of the prone position on renal function [25,26]. To date, no definitive conclusion has been drawn on whether prone positioning significantly increases the risk of AKI or whether returning to the supine position can effectively reverse renal impairment. Additionally, the relationship between BMI, AKI, and prone positioning has not been previously explored. Weig et al. examined the effects of abdominal obesity on organ function in patients with H1N1-associated ARDS undergoing prolonged cumulative prone positioning [26]. That study reported a higher incidence of renal failure in abdominally obese patients compared to non-abdominally obese ones (83% vs. 35%; p < 0.01), although abdominal obesity was defined by a sagittal abdominal diameter of ≥26 cm, without consideration of BMI.
Our findings reveal that prone positioning is a safe intervention for non-obese patients, with no significant impact on renal function. However, in overweight or obese patients, kidney failure can be expected within hours of prone positioning, potentially persisting for an extended period. Thus, careful preparation and monitoring are essential when managing these patients. In this context, our results support Weig et al.’s recommendation of exercising caution with prone positioning in obese patients [26].
The precise pathophysiology connecting prone positioning to renal failure remains incompletely understood. One proposed mechanism is the induction of intra-abdominal hypertension (IAH) by the prone position [24,38], which has been associated with impaired renal function due to elevated renal vein pressure, reduced arterial perfusion, and decreased glomerular filtration rate [39,40,41,42,43,44]. This effect is particularly significant in obese patients, who are more susceptible to IAH and its renal implications [40,45,46]. Additionally, increased renal parenchymal pressure in the prone position may lead to renal ischemia, further contributing to AKI [44]. Obesity exacerbates this risk, as it is associated with glomerular hypertrophy, which heightens the kidneys’ vulnerability to ischemic injury [22].
Urologic surgeries, particularly percutaneous nephrolithotomy (PCNL) performed in the prone position, have been associated with an increased risk of AKI [47,48,49,50,51]. This risk is attributed to factors such as hemodynamic changes, increased intra-abdominal pressure, and compartment syndrome during prolonged procedures [47,52]. To mitigate these risks, careful patient positioning, vigilant intraoperative monitoring, and minimizing operative time are essential strategies. Additionally, maintaining adequate hydration and ensuring proper padding can help reduce the incidence of AKI in patients undergoing urologic surgeries in the prone position [47,48].
Prone positioning is known to offer significant respiratory benefits [4,53,54,55,56], improving outcomes in patients with severe ARDS [57,58,59]. These patients often have the most critical form of ARDS (PaO2/FiO2 ratio < 100) and have exhausted all other treatment options. Therefore, avoiding prone positioning in critically ill patients to prevent AKI may not always be feasible. Nevertheless, AKI has been linked to poor outcomes and increased mortality, particularly in critically ill populations [16,18,60,61,62]. It remains important to understand the underlying causes of AKI and to explore preventative strategies.
Our findings raise the question of whether specific proning techniques might reduce the risk of AKI, particularly in obese patients. While only a few studies have addressed this issue [24,63], no prospective trial has systematically evaluated the impact of tailored proning techniques on renal outcomes. There is a pressing need for prospective studies that focus on optimizing prone positioning for obese patients to prevent renal deterioration without compromising the respiratory benefits of this intervention.
Given that AKI is a significant independent risk factor for mortality in ICU patients [18], and considering the increased risk of AKI associated with prone positioning in obese patients, a comprehensive prospective investigation is warranted. This need is even more urgent in the post-COVID-19 era, where obese patients experienced higher mortality rates during the pandemic. The increased susceptibility of obese individuals to future respiratory pandemics, combined with the higher mortality risk, is further complicated by the more frequent use of prone positioning in ICUs post COVID-19 compared to pre-pandemic levels. These factors suggest that the mortality risk could be amplified in future respiratory pandemics, underscoring the necessity of further research and preventative measures.
This study has several limitations. First, being a retrospective single-center study inherently restricts our sample size and the ability to establish causality. Second, because prone positioning is a validated treatment for hypoxemic ARDS patients, conducting a standard case–control study with a control group of similarly severe hypoxemic patients who did not receive prone positioning was not feasible. Consequently, we utilized a suboptimal pre–post study design, complicating the differentiation between the effects of prone positioning on kidney function and the patients’ overall clinical deterioration. While we collected data on potential confounders such as the MAP, SOFA score, and lactate levels pre and post proning, no significant changes were observed in these parameters, indicating that AKI may be more closely associated with the prone position itself than with systemic clinical decline. However, the complete elimination of inherent biases is unattainable.
Third, we did not directly measure intra-abdominal pressure or abdominal obesity, relying instead on BMI as a proxy for obesity, which limits our ability to definitively establish causality between these factors and AKI. Additionally, data were collected within 24 h of the position change, focusing on the immediate effects of prone positioning on kidney injury. Therefore, the longer-term impacts of prone positioning remain unclear. Another limitation is that the mean time in the prone position exceeded the recommended 16 h, as per the PROSEVA study. This was due to two factors: the slow implementation of the 16 h proning regimen and the increased patient load during the COVID-19 pandemic, which restricted treatment options and prolonged proning times. The question of whether shorter proning durations could reduce the incidence of prone-related AKI remains open.
5. Conclusions
In conclusion, our study highlights a significant association between prone positioning and the development of AKI in overweight or obese patients with ARDS. This may be due to the increased vulnerability of the kidneys to IAH. While prone positioning is an established intervention that offers substantial respiratory benefits in ARDS management, our findings indicate that it may pose an increased risk of renal impairment, particularly in this patient population. Given the higher morbidity associated with AKI and its potential long-term consequences, careful monitoring and consideration of alternative strategies may be warranted when implementing prone positioning in obese patients. Future research should focus on optimizing proning techniques and exploring preventive measures to mitigate renal risks without compromising respiratory outcomes, especially in the context of the ongoing challenges posed by increasing obesity rates and the lingering effects of the COVID-19 pandemic on ICU practices.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/jcm14020631/s1: Table S1: Baseline patient comorbidities; Table S2: Univariate analysis of lab results during ICU admission: before and after prone and supine position; Table S3: Univariate analysis of patients’ SOFA scores during ICU admission, stratified by BMI; Table S4: Univariate analysis of patients’ urea and creatinine during ICU admission: before and after prone and supine position; Table S5: Analysis of patient BMI; Table S6: Univariate analysis of AKIN criteria based on creatinine (mg/dL), stratified by age; Table S7: Univariate analysis of AKIN criteria based on urine output (mL/h), stratified by age; Table S8: Univariate analysis of eGFR before and after prone position, stratified by BMI; Table S9: Multivariate logistic regression model for predicting AKI occurrence, stratified by COVID-19 infection; and Table S10: Univariate analysis of AKIN scores based on creatinine (mg/dL) at different time points in patients with AKI after prone positioning.
Author Contributions
Conceptualization, E.E., D.B. and L.F.; methodology, E.E., D.B. and L.F.; formal analysis, I.H.; investigation, E.E., I.H. and L.F.; resources, L.F.; data curation, E.E., D.B., A.A. and A.S.B.; writing—original draft preparation, E.E. and L.F.; writing—review and editing, E.E., R.G., J.T. and L.F.; visualization, I.H. and E.E.; supervision, L.F.; project administration, D.B. and L.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee of Soroka University Medical Center (SUMC) (protocol code SCRC20017 on 21 December 2020).
Informed Consent Statement
Patient consent was waived by the Institutional Ethics Committee due to the retrospective study design.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. JAMA 2018, 319, 698. [Google Scholar] [CrossRef] [PubMed]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Taccone, P.; Carlesso, E.; Marini, J.J. Prone Position in Acute Respiratory Distress Syndrome. Rationale, Indications, and Limits. Am. J. Respir. Crit. Care Med. 2013, 188, 1286–1293. [Google Scholar] [CrossRef] [PubMed]
- Coppo, A.; Bellani, G.; Winterton, D.; Di Pierro, M.; Soria, A.; Faverio, P.; Cairo, M.; Mori, S.; Messinesi, G.; Contro, E.; et al. Feasibility and physiological effects of prone positioning in non-intubated patients with acute respiratory failure due to COVID-19 (PRON-COVID): A prospective cohort study. Lancet Respir. Med. 2020, 8, 765–774. [Google Scholar] [CrossRef]
- Parker, E.M.; Bittner, E.A.; Berra, L.; Pino, R.M. Efficiency of Prolonged Prone Positioning for Mechanically Ventilated Patients Infected with COVID-19. J. Clin. Med. 2021, 10, 2969. [Google Scholar] [CrossRef]
- Weiss, T.T.; Cerda, F.; Scott, J.B.; Kaur, R.; Sungurlu, S.; Mirza, S.H.; Alolaiwat, A.A.; Augustynovich, A.E.; Li, J. Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID-19: A retrospective observational cohort study. Br. J. Anaesth. 2021, 126, 48–55. [Google Scholar] [CrossRef]
- Henderson, W.R.; Griesdale, D.E.; Dominelli, P.; Ronco, J.J. Does prone positioning improve oxygenation and reduce mortality in patients with acute respiratory distress syndrome? Can. Respir. J. 2014, 21, 213–215. [Google Scholar] [CrossRef]
- Gong, M.N.; Bajwa, E.K.; Thompson, B.T.; Christiani, D.C. Body mass index is associated with the development of acute respiratory distress syndrome. Thorax 2010, 65, 44–50. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef]
- Flegal, K.M.; Kruszon-Moran, D.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA 2016, 315, 2284–2291. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, K.; Lewandowski, M. Intensive care in the obese. Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Madl, C.; Filipescu, D.; Moreno, R.; Groeneveld, J.; Artigas, A.; Reinhart, K.; Vincent, J.-L. Obesity is associated with increased morbidity but not mortality in critically ill patients. Intensive Care Med. 2008, 34, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Akinnusi, M.E.; Pineda, L.A.; El Solh, A.A. Effect of obesity on intensive care morbidity and mortality: A meta-analysis. Crit. Care Med. 2008, 36, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; Gjerde, S.; Guttormsen, A.B.; Haugen, O.; Høivik, T.; Onarheim, H.; Aardal, S. Outcome after acute respiratory failure is more dependent on dysfunction in other vital organs than on the severity of the respiratory failure. Crit. Care 2003, 7, R72–R77. [Google Scholar] [CrossRef]
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Rewa, O.; Bagshaw, S.M. Acute kidney injury—Epidemiology, outcomes and economics. Nat. Rev. Nephrol. 2014, 10, 193–207. [Google Scholar] [CrossRef]
- Fuchs, L.; Lee, J.; Novack, V.; Baumfeld, Y.; Scott, D.; Celi, L.; Mandelbaum, T.; Howell, M.; Talmor, D. Severity of Acute Kidney Injury and Two-Year Outcomes in Critically Ill Patients. Chest 2013, 144, 866–875. [Google Scholar] [CrossRef]
- Soto, G.J.; Frank, A.J.; Christiani, D.C.; Gong, M.N. Body mass index and acute kidney injury in the acute respiratory distress syndrome. Crit. Care Med. 2012, 40, 2601–2608. [Google Scholar] [CrossRef]
- Druml, W.; Metnitz, B.; Schaden, E.; Bauer, P.; Metnitz, P.G.H. Impact of body mass on incidence and prognosis of acute kidney injury requiring renal replacement therapy. Intensive Care Med. 2010, 36, 1221–1228. [Google Scholar] [CrossRef]
- Billings, F.T.; Pretorius, M.; Schildcrout, J.S.; Mercaldo, N.D.; Byrne, J.G.; Ikizler, T.A.; Brown, N.J. Obesity and oxidative stress predict AKI after cardiac surgery. J. Am. Soc. Nephrol. 2012, 23, 1221–1228. [Google Scholar] [CrossRef] [PubMed]
- Danziger, J.M.; Chen, K.P.; Lee, J.; Feng, M.; Mark, R.G.; Celi, L.A.; Mukamal, K.J. Obesity, Acute Kidney Injury, and Mortality in Critical Illness. Crit. Care Med. 2016, 44, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Edgcombe, H.; Carter, K.; Yarrow, S. Anaesthesia in the prone position. Br. J. Anaesth. 2008, 100, 165–183. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, A.W.; Pelosi, P.; De Waele, J.J.; Malbrain, M.L.; Ball, C.G.; Meade, M.O.; Stelfox, H.T.; Laupland, K.B. Clinical review: Intra-abdominal hypertension: Does it influence the physiology of prone ventilation? Crit. Care 2010, 14, 232. [Google Scholar] [CrossRef]
- Hering, R.; Wrigge, H.; Vorwerk, R.; Brensing, K.A.; Schröder, S.; Zinserling, J.; Hoeft, A.; Spiegel, T.V.; Putensen, C. The Effects of Prone Positioning on Intraabdominal Pressure and Cardiovascular and Renal Function in Patients with Acute Lung Injury. Anesth. Analg. 2001, 92, 1226–1231. [Google Scholar] [CrossRef]
- Weig, T.; Janitza, S.; Zoller, M.; Dolch, M.E.; Miller, J.; Frey, L.; Kneidinger, N.; Johnson, T.; Schubert, M.I.; Irlbeck, M. Influence of abdominal obesity on multiorgan dysfunction and mortality in acute respiratory distress syndrome patients treated with prone positioning. J. Crit. Care 2014, 29, 557–561. [Google Scholar] [CrossRef]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Cruz, D.N.; Ricci, Z.; Ronco, C. Clinical review: RIFLE and AKIN—Time for reappraisal. Crit. Care 2009, 13, 211. [Google Scholar] [CrossRef]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed]
- Salazar, D.E.; Corcoran, G.B. Predicting creatinine clearance and renal drug clearance in obese patients from estimated fat-free body mass. Am. J. Med. 1988, 84, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.; Capotondo, M.M.; Quaintenne, M.; Musso-Enz, G.M.; Aroca-Martinez, G.; Musso, C.G. Obesity and glomerular filtration rate. Int. Urol. Nephrol. 2024, 56, 1663–1668. [Google Scholar] [CrossRef]
- Chang-Panesso, M. Acute kidney injury and aging. Pediatr. Nephrol. 2021, 36, 2997–3006. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G. Acute Kidney Injury in Elderly Persons. Am. J. Kidney Dis. 2010, 56, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Tsai, H.B.; Wu, C.Y.; Lin, Y.-F.; Hsu, N.-C.; Chen, J.-S.; Hung, K.-Y. The severity of initial acute kidney injury at admission of geriatric patients significantly correlates with subsequent in-hospital complications. Sci. Rep. 2015, 5, 13925. [Google Scholar] [CrossRef]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute Kidney Injury Increases Risk of ESRD among Elderly. J. Am. Soc. Nephrol. 2009, 20, 223–228. [Google Scholar] [CrossRef]
- Jin, S.-J.; Park, Y.-S.; Kim, S.-H.; Kim, D.; Shim, W.-H.; Jang, D.-M.; Shaffrey, C.I.; Naik, B.I. Effect of Prone Positional Apparatus on the Occurrence of Acute Kidney Injury after Spine Surgery. World Neurosurg. 2019, 128, e597–e602. [Google Scholar] [CrossRef]
- De Waele, J.J.; De Laet, I.; Kirkpatrick, A.W.; Hoste, E. Intra-abdominal Hypertension and Abdominal Compartment Syndrome. Am. J. Kidney Dis. 2011, 57, 159–169. [Google Scholar] [CrossRef]
- Shashaty, M.G.S.; Stapleton, R.D. Physiological and Management Implications of Obesity in Critical Illness. Ann. Am. Thorac. Soc. 2014, 11, 1286–1297. [Google Scholar] [CrossRef]
- Dalfino, L.; Tullo, L.; Donadio, I.; Malcangi, V.; Brienza, N. Intra-abdominal hypertension and acute renal failure in critically ill patients. Intensive Care Med. 2008, 34, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Biancofiore, G.; Bindi, M.L.; Romanelli, A.; Boldrini, A.; Consani, G.; Bisà, M.; Filipponi, F.; Vagelli, A.; Mosca, F. Intra-abdominal pressure monitoring in liver transplant recipients: A prospective study. Intensive Care Med. 2003, 29, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Doty, J.M.; Saggi, B.H.; Sugerman, H.J.; Blocher, C.R.; Pin, R.; Fakhry, I.; Gehr, T.W.B.; Sica, D.A. Effect of increased renal venous pressure on renal function. J. Trauma Acute Care Surg. 1999, 47, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Sun, H.; Sun, Z.; Yang, X.; Zhou, S.; Wei, J. Intra-abdominal hypertension and increased acute kidney injury risk: A systematic review and meta-analysis. J. Int. Med. Res. 2021, 49, 03000605211016627. [Google Scholar] [CrossRef] [PubMed]
- Holodinsky, J.K.; Roberts, D.J.; Ball, C.G.; Blaser, A.R.; Starkopf, J.; A Zygun, D.; Stelfox, H.T.; Malbrain, M.L.; Jaeschke, R.C.; Kirkpatrick, A.W. Risk factors for intra-abdominal hypertension and abdominal compartment syndrome among adult intensive care unit patients: A systematic review and meta-analysis. Crit. Care 2013, 17, R249. [Google Scholar] [CrossRef]
- Smit, M.; Werner, M.J.M.; Lansink-Hartgring, A.O.; Dieperink, W.; Zijlstra, J.G.; van Meurs, M. How central obesity influences intra-abdominal pressure: A prospective, observational study in cardiothoracic surgical patients. Ann. Intensive Care 2016, 6, 99. [Google Scholar] [CrossRef]
- Akhavan, A.; Gainsburg, D.M.; Stock, J.A. Complications Associated with Patient Positioning in Urologic Surgery. Urology 2010, 76, 1309–1316. [Google Scholar] [CrossRef]
- Boyer, N.; Eldridge, J.; Prowle, J.R.; Forni, L.G. Postoperative Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2022, 17, 1535. [Google Scholar] [CrossRef]
- Bozorgmehri, S.; Gilbert, S.; Cook, R.L.; Beyth, R.; Ozrazgat-Baslanti, T.; Bihorac, A.; Canales, M. PD13-09 Acute Kidney Injury After Urologic Surgeries. J. Urol. 2018, 199, e302. [Google Scholar] [CrossRef]
- Caddeo, G.; Williams, S.T.; McIntyre, C.W.; Selby, N.M. Acute Kidney Injury in Urology Patients: Incidence, Causes and Outcomes. Nephro-Urol. Mon. 2013, 5, 955–961. [Google Scholar] [CrossRef]
- Schmid, M.; Dalela, D.; Tahbaz, R.; Langetepe, J.; Randazzo, M.; Dahlem, R.; Fisch, M.; Trinh, Q.-D.; Chun, F.K. Novel biomarkers of acute kidney injury: Evaluation and evidence in urologic surgery. World J. Nephrol. 2015, 4, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Gal, J.; Hyman, J.; Gainsburg, D.M. Positioning for Urological Procedures. In Anesthesia for Urologic Surgery; Gainsburg, D.M., Bryson, E.O., Frost, E.A.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 243–269. [Google Scholar] [CrossRef]
- Abroug, F.; Ouanes-Besbes, L.; Elatrous, S.; Brochard, L. The effect of prone positioning in acute respiratory distress syndrome or acute lung injury: A meta-analysis. Areas of uncertainty and recommendations for research. Intensive Care Med. 2008, 34, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Charron, C.; Repesse, X.; Bouferrache, K.; Bodson, L.; Castro, S.; Page, B.; Jardin, F.; Vieillard-Baron, A. PaCO2 and alveolar dead space are more relevant than PaO2/FiO2 ratio in monitoring the respiratory response to prone position in ARDS patients: A physiological study. Crit. Care 2011, 15, R175. [Google Scholar] [CrossRef] [PubMed]
- Langer, T.; Brioni, M.; Guzzardella, A.; Carlesso, E.; Cabrini, L.; Castelli, G.; Dalla Corte, F.; De Robertis, E.; Favarato, M.; Forastieri, A.; et al. Prone position in intubated, mechanically ventilated patients with COVID-19: A multi-centric study of more than 1000 patients. Crit. Care 2021, 25, 128. [Google Scholar] [CrossRef]
- Blanch, L.; Mancebo, J.; Perez, M.; Martinez, M.; Mas, A.; Betbese, A.J.; Joseph, D.; Ballús, J.; Lucangelo, U.; Bak, E. Short-term effects of prone position in critically ill patients with acute respiratory distress syndrome. Intensive Care Med. 1997, 23, 1033–1039. [Google Scholar] [CrossRef]
- Mathews, K.S.; Soh, H.; Shaefi, S.; Wang, W.; Bose, S.; Coca, S.; Gupta, S.; Hayek, S.S.; Srivastava, A.; Brenner, S.K.; et al. Prone Positioning and Survival in Mechanically Ventilated Patients with Coronavirus Disease 2019—Related Respiratory Failure. Crit. Care Med. 2021. Publish Ahead of Print. [Google Scholar] [CrossRef]
- Sud, S.; Friedrich, J.O.; Taccone, P.; Polli, F.; Adhikari, N.K.J.; Latini, R.; Pesenti, A.; Guérin, C.; Mancebo, J.; Curley, M.A.Q.; et al. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: Systematic review and meta-analysis. Intensive Care Med. 2010, 36, 585–599. [Google Scholar] [CrossRef]
- Gattinoni, L.; Busana, M.; Giosa, L.; Macrì, M.M.; Quintel, M. Prone Positioning in Acute Respiratory Distress Syndrome. Semin. Respir. Crit. Care Med. 2019, 40, 94–100. [Google Scholar] [CrossRef]
- Abebe, A.; Kumela, K.; Belay, M.; Kebede, B.; Wobie, Y. Mortality and predictors of acute kidney injury in adults: A hospital-based prospective observational study. Sci. Rep. 2021, 11, 15672. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Waikar, S.S.; Liu, K.D.; Chertow, G.M. Diagnosis, Epidemiology and Outcomes of Acute Kidney Injury. Clin. J. Am. Soc. Nephrol. 2008, 3, 844–861. [Google Scholar] [CrossRef]
- Chiumello, D.; Cressoni, M.; Racagni, M.; Landi, L.; Bassi, G.L.; Polli, F.; Carlesso, E.; Gattinoni, L. Effects of thoraco-pelvic supports during prone position in patients with acute lung injury/acute respiratory distress syndrome: A physiological study. Crit. Care 2006, 10, R87. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).