
Clinical Comparison of CAD/CAM vs. KLS L1® Mandible ReconGuide in Fibula Free Flap Mandible Reconstruction: A Retrospective Clinical Study

Abstract
1. Introduction
2. Material and Methods
2.1. Preoperative Planning
2.2. Operative Procedure KLS L1 Mandible ReconGuide
2.3. Operative Procedure CAD/CAM
2.4. Data Collection and Processing
2.5. Statistical Analysis
3. Results
3.1. Clinical Criteria
3.1.1. Operative Data
3.1.2. Postoperative Complications
3.1.3. Functional Rehabilitation
3.2. Geometric Criteria
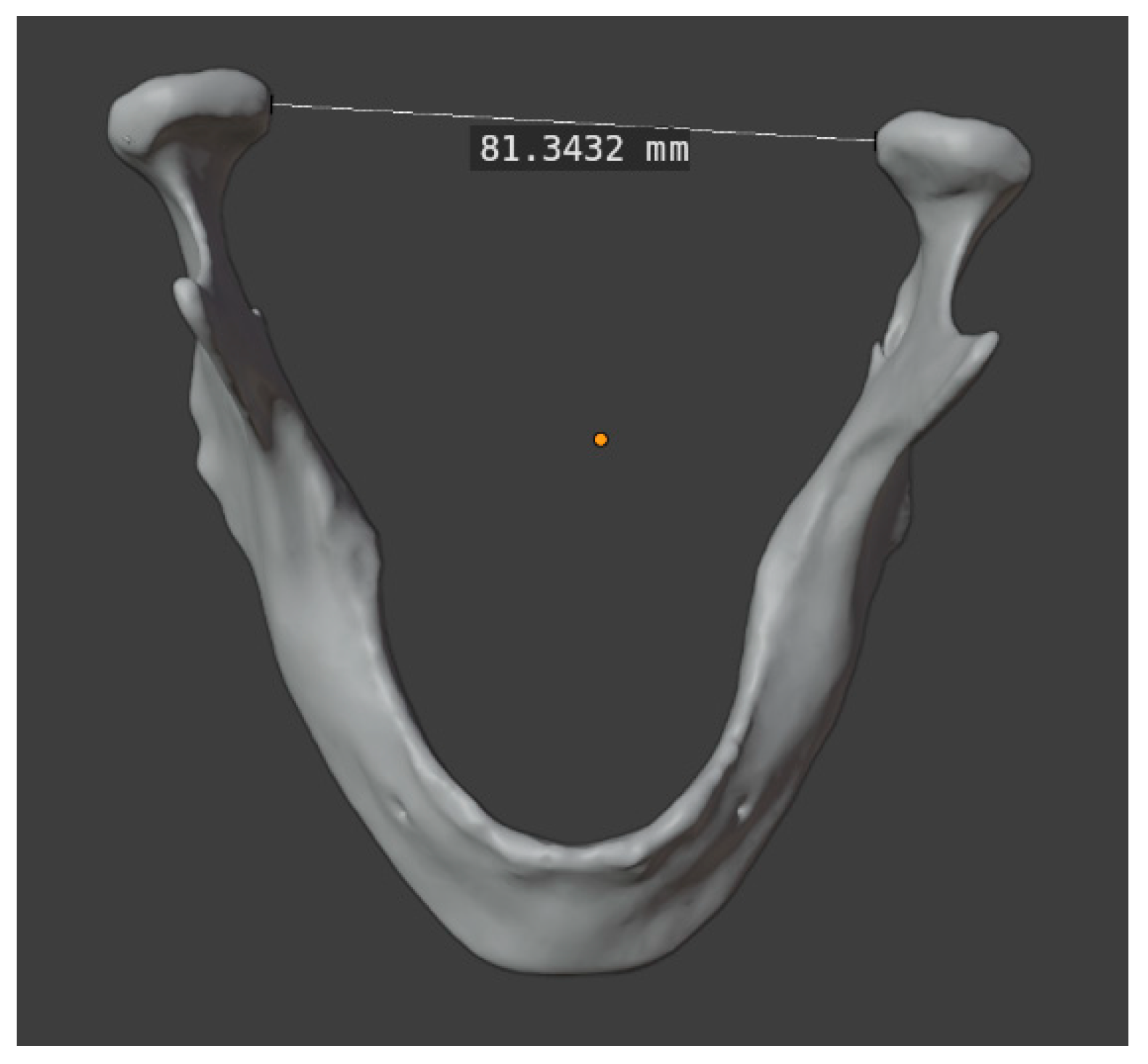
3.2.1. Intercondylar Distance
3.2.2. Gonial Angle
3.2.3. Intersegmental Distances
3.2.4. Length of Symphysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CAD/CAM | Computer-aided design/computer-aided manufacturing |
| CT | Computer tomography |
| FFF | The fibula free flap |
| IDDSI | International Dysphagia Diet Standardisation Initiative |
| IQR | Interquartile range |
| PEG | Percutaneous endoscopic gastrostomy |
| PSI | Patient-specific implant |
| SD | Standard deviation |
| STL | Standard triangle language |
References
- Hidalgo, D.A. Fibula free flap: A new method of mandible reconstruction. Plast. Reconstr. Surg. 1989, 84, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Harrison, P.; Cheng, A.; Bray, B.; Bell, R.B. Fibular Reconstruction of the Maxilla and Mandible with Immediate Implant-Supported Prosthetic Rehabilitation: Jaw in a Day. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 369–386. [Google Scholar] [CrossRef] [PubMed]
- Fatani, B.; Fatani, J.A.; Fatani, O.A. Approach for Mandibular Reconstruction Using Vascularized Free Fibula Flap: A Review of the Literature. Cureus 2022, 14, e30161. [Google Scholar] [CrossRef] [PubMed]
- Bartier, S.; Mazzaschi, O.; Benichou, L.; Sauvaget, E. Computer-assisted versus traditional technique in fibular free-flap mandibular reconstruction: A CT symmetry study. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138, 23–27. [Google Scholar] [CrossRef]
- Ince, B.; Ismayilzade, M.; Dadaci, M.; Zuhal, E. Computer-Assisted versus Conventional Freehand Mandibular Reconstruction with Fibula Free Flap: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg. 2020, 146, 686e–687e. [Google Scholar] [CrossRef]
- Ren, W.; Gao, L.; Li, S.; Chen, C.; Li, F.; Wang, Q.; Zhi, Y.; Song, J.; Dou, Z.; Xue, L.; et al. Virtual Planning and 3D printing modeling for mandibular reconstruction with fibula free flap. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e359–e366. [Google Scholar] [CrossRef]
- Copelli, C.; Cacciatore, F.; Cocis, S.; Maglitto, F.; Barbara, F.; Iocca, O.; Manfuso, A. Bone reconstruction using CAD/CAM technology in head and neck surgical oncology. A narrative review of state of the art and aesthetic-functional outcomes. Acta Otorhinolaryngol. Ital. 2024, 44, S58–S66. [Google Scholar] [CrossRef]
- Hou, J.-S.; Chen, M.; Pan, C.-B.; Wang, M.; Wang, J.-G.; Zhang, B.; Tao, Q.; Wang, C.; Huang, H.-Z. Application of CAD/CAM-assisted technique with surgical treatment in reconstruction of the mandible. J. Craniomaxillofac. Surg. 2012, 40, e432–e437. [Google Scholar] [CrossRef]
- Bouchet, B.; Raoul, G.; Julieron, B.; Wojcik, T. Functional and morphologic outcomes of CAD/CAM-assisted versus conventional microvascular fibular free flap reconstruction of the mandible: A retrospective study of 25 cases. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 455–460. [Google Scholar] [CrossRef]
- Riccio, S.; Tagliabue, M.; Soncini, G.; Giugliano, G.; Bruschini, R.; Zorzi, S.; de Benedetto, L.; Chu, F.; de Berardinis, R.; Ansarin, M. An innovative tool for mandibular reconstruction in oral malignancies: A pictorial essay. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, e81–e84. [Google Scholar] [CrossRef]
- Matsuda, Y.; Jayasinghe, R.D.; Zhong, H.; Arakawa, S.; Kanno, T. Oral Health Management and Rehabilitation for Patients with Oral Cancer: A Narrative Review. Healthcare 2022, 10, 960. [Google Scholar] [CrossRef] [PubMed]
- Mahendru, S.; Jain, R.; Aggarwal, A.; Aulakh, H.S.; Jain, A.; Khazanchi, R.K.; Sarin, D. CAD-CAM vs conventional technique for mandibular reconstruction with free fibula flap: A comparison of outcomes. Surg. Oncol. 2020, 34, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Clymer, J.W.; Po-Han Chen, B.; Sadeghirad, B.; Ferko, N.C.; Cameron, C.G.; Hinoul, P. Prolonged operative duration is associated with complications: A systematic review and meta-analysis. J. Surg. Res. 2018, 229, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Ortner, F.; Eberl, M.; Otto, S.; Wang, B.; Schauberger, G.; Hofmann-Kiefer, K.; Saller, T. Patient-related and anesthesia-dependent determinants for postoperative delirium after oral and maxillofacial surgery. Results from a register-based case-control study. J. Stomatol. Oral Maxillofac. Surg. 2021, 122, 62–69. [Google Scholar] [CrossRef]
- Su, N.; Liu, Y.; Yang, X.; Luo, Z.; Shi, Z. Correlation between bony changes measured with cone beam computed tomography and clinical dysfunction index in patients with temporomandibular joint osteoarthritis. J. Craniomaxillofac. Surg. 2014, 42, 1402–1407. [Google Scholar] [CrossRef]
- Barr, M.L.; Haveles, C.S.; Rezzadeh, K.S.; Nolan, I.T.; Castro, R.; Lee, J.C.; Steinbacher, D.; Pfaff, M.J. Virtual Surgical Planning for Mandibular Reconstruction With the Fibula Free Flap: A Systematic Review and Meta-analysis. Ann. Plast. Surg. 2020, 84, 117–122. [Google Scholar] [CrossRef]
- Urken, M.L.; Weinberg, H.; Vickery, C.; Buchbinder, D.; Lawson, W.; Biller, H.F. Oromandibular Reconstruction Using Microvascular Composite Free Flaps: Report of 71 Cases and a New Classification Scheme for Bony, Soft-Tissue, and Neurologic Defects. Arch. Otolaryngol.—Head Neck Surg. 1991, 117, 733–744. [Google Scholar] [CrossRef]
- Weitz, J.; Grabenhorst, A.; Singer, H.; Niu, M.; Grill, F.D.; Kamreh, D.; Claßen, C.A.S.; Wolff, K.-D.; Ritschl, L.M. Mandibular reconstructions with free fibula flap using standardized partially adjustable cutting guides or CAD/CAM technique: A three- and two-dimensional comparison. Front. Oncol. 2023, 13, 1167071. [Google Scholar] [CrossRef]
- Weitz, J.; Wolff, K.-D.; Kesting, M.R.; Nobis, C.-P. Development of a novel resection and cutting guide for mandibular reconstruction using free fibula flap. J. Craniomaxillofac. Surg. 2018, 46, 1975–1978. [Google Scholar] [CrossRef]
- Goldman, L.W. Principles of CT: Radiation dose and image quality. J. Nucl. Med. Technol. 2007, 35, 213–225; quiz 226–228. [Google Scholar] [CrossRef]
- Chang, Y.-M.; Wei, F.-C. Fibula Jaw-in-a-Day with Minimal Computer-Aided Design and Manufacturing: Maximizing Efficiency, Cost-Effectiveness, Intraoperative Flexibility, and Quality. Plast. Reconstr. Surg. 2021, 147, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, B.; Levine, J.P.; Hirsch, D.L.; Bastidas, J.A.; Schiff, B.A.; Garfein, E.S. Importance of computer-aided design and manufacturing technology in the multidisciplinary approach to head and neck reconstruction. J. Craniofac. Surg. 2010, 21, 1277–1280. [Google Scholar] [CrossRef]
- Rempel, V.; Grandoch, A.; Safi, A.-F.; Buller, J.; Riekert, M.; Schick, V.; Nickenig, H.-J.; Zöller, J.; Kreppel, M. The prognostic implications of comorbidity and risk factors for (post)operative complications, days spent in the intensive care unit (ICU), and length of hospitalization in patients with oral squamous cell carcinoma: A prospective study. J. Craniomaxillofac. Surg. 2020, 48, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Coca-Pelaz, A.; Takes, R.P.; Hutcheson, K.; Saba, N.F.; Haigentz, M.; Bradford, C.R.; de Bree, R.; Strojan, P.; Lund, V.J.; Mendenhall, W.M.; et al. Head and Neck Cancer: A Review of the Impact of Treatment Delay on Outcome. Adv. Ther. 2018, 35, 153–160. [Google Scholar] [CrossRef]
- Petrovic, I.; Rosen, E.B.; Matros, E.; Huryn, J.M.; Shah, J.P. Oral rehabilitation of the cancer patient: A formidable challenge. J. Surg. Oncol. 2018, 117, 1729–1735. [Google Scholar] [CrossRef]
- Ritschl, L.M.; Singer, H.; Clasen, F.-C.; Haller, B.; Fichter, A.M.; Deppe, H.; Wolff, K.-D.; Weitz, J. Oral rehabilitation and associated quality of life following mandibular reconstruction with free fibula flap: A cross-sectional study. Front. Oncol. 2024, 14, 1371405. [Google Scholar] [CrossRef]
- Latifi, F.; Tabrizi, R.; Kordkheili, M.H.; Shahbazi, S.; Fernandes, G.V.O. The Influence of Implant Number on Stress Distribution in the Anterior Region of Mandible Reconstructed with Fibula Bone Graft: A Finite Element Analysis. J. Maxillofac. Oral Surg. 2024, 23, 1–8. [Google Scholar] [CrossRef]
- Latifi, F.; Tabrizi, R.; Hosseinikordkheili, M. How does the Number of Implants Affect Stress Distribution in Fibula Graft at the Posterior of the Mandible? A Finite Element Analysis. J. Maxillofac. Oral Surg. 2023, 22, 304–312. [Google Scholar] [CrossRef]
- Ohkoshi, A.; Sato, N.; Kurosawa, K.; Miyashita, H.; Ishii, R.; Nakanome, A.; Ogawa, T.; Tachi, M.; Takahashi, T.; Katori, Y. Impact of CAD/CAM mandibular reconstruction on chewing and swallowing function after surgery for locally advanced oral cancer: A retrospective study of 50 cases. Auris Nasus Larynx 2021, 48, 1007–1012. [Google Scholar] [CrossRef]
- Mao, X.-Y.; Fu, X.; Niu, F.; Chen, Y.; Jin, Q.; Qiao, J.; Gui, L. Computer-assisted mandibular curved osteotomy: An automatic method to design the new aesthetic gonion and osteotomy line. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 2622–2628. [Google Scholar] [CrossRef]
- Valletta, R.; Rongo, R.; Pango Madariaga, A.C.; Baiano, R.; Spagnuolo, G.; D’Antò, V. Relationship between the Condylion-Gonion-Menton Angle and Dentoalveolar Heights. Int. J. Environ. Res. Public Health 2020, 17, 3309. [Google Scholar] [CrossRef] [PubMed]
- Larrazabal-Moron, C.; Sanchis-Gimeno, J.A. Gonial angle growth patterns according to age and gender. Ann. Anat. 2018, 215, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, C.N.; Ozturk, C.; Bozkurt, M.; Uygur, H.S.; Papay, F.A.; Zins, J.E. Dentition, bone loss, and the aging of the mandible. Aesthet. Surg. J. 2013, 33, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Lemes, C.R.; Tozzi, C.F.; Gribel, S.; Gribel, B.F.; Venezian, G.C.; do Carmo Menezes, C.; Custodio, W. Mandibular ramus height and condyle distance asymmetries in individuals with different facial growth patterns: A cone-beam computed tomography study. Surg. Radiol. Anat. 2021, 43, 267–274. [Google Scholar] [CrossRef]
- Lazić, B.; Tepavcević, B.; Keros, J.; Komar, D.; Stanicić, T.; Azinović, Z. Intercondylar distances of the human temporomandibular joints. Coll. Antropol. 2006, 30, 37–41. [Google Scholar] [PubMed]
- Hackney, F.L.; van Sickels, J.E.; Nummikoski, P.V. Condylar displacement and temporomandibular joint dysfunction following bilateral sagittal split osteotomy and rigid fixation. J. Oral Maxillofac. Surg. 1989, 47, 223–227. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KLS L1® Mandible ReconGuide (G1) | CAD/CAM (G2) | p-Value | |
|---|---|---|---|
| Duration of surgery (min) | 12.28 [10.50, 13.49] | 11.87 [10.70, 16.10] | 0.607 |
| Hospitalization (d) | 23.50 [19.25, 32.00] | 39.00 [24.00, 42.50] | 0.226 |
| Postoperative delirium | 4 (22.2%) | 2 (28.6%) | 1 |
| Thrombosis | 0 | 0 | n.a. |
| Reintervention | 8 (44.4%) | 2 (28.6%) | 0.785 |
| Plate exposition | 4 (22.2%) | 2 (28.6%) | 1 |
| Wound dehiscence | 7 (38.9%) | 4 (57.1%) | 0.706 |
| Infection (local) | 3 (16.7%) | 2 (28.6%) | 0.911 |
| Infection (systemic) | 2 (11.1%) | 2 (28.6%) | 0.644 |
| KLS L1® Mandible ReconGuide (G1) | CAD/CAM (G2) | p-Value | |
|---|---|---|---|
| Intercondylar distance (preop) | 83.99 [81.10, 86.93] | 84.25 [82.68, 87.36] | 0.672 |
| Intercondylar distance (postop) | 85.50 [81.57, 88.04] | 85.03 [79.43, 93.91] | 1.000 |
| Intercondylar distance (difference) | −0.33 [−2.15, 1.57] | −0.78 [−3.54, 2.55] | 0.952 |
| Gonial angle (preop) | 121.50 [119.25, 129.75] | 125.00 [118, 127.50] | 0.716 |
| Gonial angle (postop) | 127.00 [118.00, 133.00] | 123.00 [119, 132] | 0.832 |
| Gonial angle (difference) | −2.00 [−10.25, 2.50] | −3.00 [−6.50, 4.00] | 0.879 |
| Length of symphysis (preop) | 30.93 [28.75, 35.37] | 30.86 [28.19, 33.43] | 0.641 |
| Length of symphysis (postop) | 30.41 [28.95, 32.55] | 34.78 [32.75, 35.90] | 0.046 |
| Length of symphysis (difference) | −0.40 [−2.25, 2.77] | −1.59 [−7.11, 0.38] | 0.205 |
| Intersegmental distance | 0 | 0 | n.a. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denk, L.; Sigwart, A.-M.; Kolk, A.; Walch, B. Clinical Comparison of CAD/CAM vs. KLS L1® Mandible ReconGuide in Fibula Free Flap Mandible Reconstruction: A Retrospective Clinical Study. J. Clin. Med. 2025, 14, 736. https://doi.org/10.3390/jcm14030736
Denk L, Sigwart A-M, Kolk A, Walch B. Clinical Comparison of CAD/CAM vs. KLS L1® Mandible ReconGuide in Fibula Free Flap Mandible Reconstruction: A Retrospective Clinical Study. Journal of Clinical Medicine. 2025; 14(3):736. https://doi.org/10.3390/jcm14030736
Chicago/Turabian StyleDenk, Lena, Anna-Maria Sigwart, Andreas Kolk, and Benjamin Walch. 2025. "Clinical Comparison of CAD/CAM vs. KLS L1® Mandible ReconGuide in Fibula Free Flap Mandible Reconstruction: A Retrospective Clinical Study" Journal of Clinical Medicine 14, no. 3: 736. https://doi.org/10.3390/jcm14030736
APA StyleDenk, L., Sigwart, A.-M., Kolk, A., & Walch, B. (2025). Clinical Comparison of CAD/CAM vs. KLS L1® Mandible ReconGuide in Fibula Free Flap Mandible Reconstruction: A Retrospective Clinical Study. Journal of Clinical Medicine, 14(3), 736. https://doi.org/10.3390/jcm14030736