
The Association Between Metabolic Syndrome and the Risk of Endometrial Cancer in Pre- and Post-Menopausal Women: A UK Biobank Study
 , ,
, , 
Abstract

1. Introduction
2. Materials and Methods
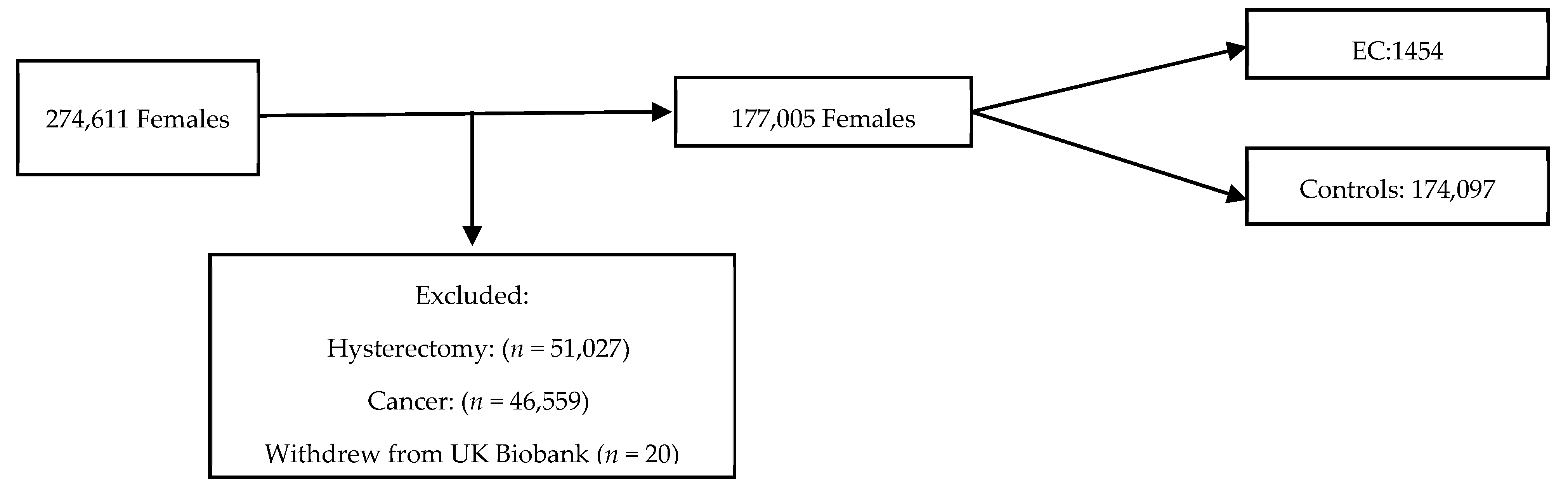
2.1. Population
2.2. Endometrial Cancer
2.3. Metabolic Syndrome Definitions
2.4. BMI Definitions
2.5. Statistical Analysis
2.6. Ethics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Wang, Y.; Zhao, R.; Wan, Q.; Wu, Y.; Zhao, L.; Wu, X. Metabolic syndrome and the risk of colorectal cancer: A systematic review and meta-analysis. Int. J. Color. Dis. 2021, 36, 2215–2225. [Google Scholar] [CrossRef]
- Karra, P.; Winn, M.; Pauleck, S.; Bulsiewicz-Jacobsen, A.; Peterson, L.; Coletta, A.; Doherty, J.; Ulrich, C.M.; Summers, S.A.; Gunter, M.; et al. Metabolic dysfunction and obesity-related cancer: Beyond obesity and metabolic syndrome. Obesity 2022, 30, 1323–1334. [Google Scholar] [CrossRef]
- Brown, K.G.M.; McBride, K.E.; Anderson, T.; Solomon, M.J. Delivering complex surgical services: Lessons learned from the evolution of a specialised pelvic exenteration centre. Aust. Health Rev. 2023, 47, 735–740. [Google Scholar] [CrossRef]
- Uterine Cancer Statistics|Cancer Research UK. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/uterine-cancer (accessed on 2 March 2024).
- Overweight and Obesity in Adults—NHS England Digital. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2021/overweight-and-obesity-in-adults (accessed on 28 April 2024).
- Hutt, S.; Mihaies, D.; Karteris, E.; Michael, A.; Payne, A.M.; Chatterjee, J. Statistical meta-analysis of risk factors for endometrial cancer and development of a risk prediction model using an artificial neural network algorithm. Cancers 2021, 13, 3689. [Google Scholar] [CrossRef]
- Consultation, W. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. 1999. Available online: http://www.staff.ncl.ac.uk/philip.home/who_dmc.htm (accessed on 22 May 2024).
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Available online: https://pubmed.ncbi.nlm.nih.gov/12485966/ (accessed on 28 November 2024).
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar] [PubMed]
- Canchola, A.J.; Chang, E.T.; Bernstein, L.; Largent, J.A.; Reynolds, P.; Deapen, D.; Ursin, G.; Horn-Ross, P.L. Body size and the risk of endometrial cancer by hormone therapy use in postmenopausal women in the California Teachers Study cohort. Cancer Causes Control. 2010, 21, 1407–1416. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ju, W.; Kim, H.J.; Hankinson, S.E.; De Vivo, I.; Cho, E. Prospective study of body fat distribution and the risk of endometrial cancer. Cancer Epidemiol. 2015, 39, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.; Cust, A.; Lahmann, P.H.; Steindorf, K.; Boutron-Ruault, M.-C.; Clavel-Chapelon, F.; Mesrine, S.; Linseisen, J.; Rohrmann, S.; Boeing, H.; et al. Anthropometric factors and risk of endometrial cancer: The European prospective investigation into cancer and nutrition. Cancer Causes Control. 2007, 18, 399–413. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Farris, M.; McNeil, J.; Friedenreich, C. Obesity and Endometrial Cancer. Recent Results Cancer Res. 2016, 208, 107–136. [Google Scholar] [PubMed]
- Cote, M.L.; Alhajj, T.; Ruterbusch, J.J.; Bernstein, L.; Brinton, L.A.; Blot, W.J.; Chen, C.; Gass, M.; Gaussoin, S.; Henderson, B.; et al. Risk factors for endometrial cancer in black and white women: A pooled analysis from the epidemiology of endometrial cancer consortium (E2C2). Cancer Causes Control. 2015, 26, 287–296. [Google Scholar] [CrossRef]
- MacKintosh, M.L.; Derbyshire, A.E.; McVey, R.J.; Bolton, J.; Nickkho-Amiry, M.; Higgins, C.L.; Kamieniorz, M.; Pemberton, P.W.; Kirmani, B.H.; Ahmed, B.; et al. The impact of obesity and bariatric surgery on circulating and tissue biomarkers of endometrial cancer risk. Int. J. Cancer 2019, 144, 641–650. [Google Scholar] [CrossRef]
- Cust, A.E.; Allen, N.E.; Rinaldi, S.; Dossus, L.; Friedenreich, C.; Olsen, A.; Tjønneland, A.; Overvad, K.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; et al. Serum levels of C-peptide, IGFBP-1 and IGFBP-2 and endometrial cancer risk; Results from the European prospective investigation into cancer and nutrition. Int. J. Cancer 2007, 120, 2656–2664. [Google Scholar] [CrossRef]
- Lukanova, A.; Zeleniuch-Jacquotte, A.; Lundin, E.; Micheli, A.; Arslan, A.A.; Rinaldi, S.; Muti, P.; Lenner, P.; Koenig, K.L.; Biessy, C.; et al. Prediagnostic levels of C-peptide, IGF-I, IGFBP -1, -2 and -3 and risk of endometrial cancer. Int. J. Cancer. 2004, 108, 262–268. [Google Scholar] [CrossRef]
- Wang, Y.; Hua, S.; Tian, W.; Zhang, L.; Zhao, J.; Zhang, H.; Zhang, W.; Xue, F. Mitogenic and anti-apoptotic effects of insulin in endometrial cancer are phosphatidylinositol 3-kinase/Akt dependent. Gynecol. Oncol. 2012, 125, 734–741. [Google Scholar] [CrossRef]
- Nagamani, M.; Stuart, C.A. Specific binding and growth-promoting activity of insulin in endometrial cancer cells in culture. Am. J. Obstet. Gynecol. 1998, 179, 6–12. [Google Scholar] [CrossRef]
- Lukanova, A.; Lundin, E.; Micheli, A.; Arslan, A.; Ferrari, P.; Rinaldi, S.; Krogh, V.; Lenner, P.; Shore, R.E.; Biessy, C.; et al. Circulating levels of sex steroid hormones and risk of endometrial cancer in postmenopausal women. Int. J. Cancer 2004, 108, 425–432. [Google Scholar] [CrossRef]
- Friberg, E.; Mantzoros, C.S.; Wolk, A. Diabetes and risk of endometrial cancer: A population-based prospective cohort study. Cancer Epidemiol. Biomark. Prev. 2007, 16, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Clement, N.S.; Oliver, T.R.W.; Shiwani, H.; Sanner, J.R.F.; Mulvaney, C.A.; Atiomo, W. Metformin for endometrial hyperplasia. Cochrane Database Syst Rev. 2017, 2017, CD012214. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Robledo, K.P.; Gebski, V.; Armes, J.E.; Alizart, M.; Cummings, M.; Chen, C.; Leung, Y.; Sykes, P.; McNally, O.; et al. Complete pathological response following levonorgestrel intrauterine device in clinically stage 1 endometrial adenocarcinoma: Results of a randomized clinical trial. Gynecol. Oncol. 2021, 161, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.B.; Lathigara, D.; Kaushal, D. Systematic Review and Meta-Analysis of the Impact of Bariatric Surgery on Future Cancer Risk. Int. J. Mol. Sci. 2023, 24, 6192. [Google Scholar] [CrossRef]
- Zhang, X.; Rhoades, J.; Caan, B.J.; E Cohn, D.; Salani, R.; Noria, S.; A Suarez, A.; Paskett, E.D.; Felix, A.S. Intentional weight loss, weight cycling, and endometrial cancer risk: A systematic review and meta-analysis. Int. J. Gynecol. Cancer 2019, 29, 1361–1371. [Google Scholar] [CrossRef]
- Wang, L.; Xu, R.; Kaelber, D.C.; Berger, N.A. Glucagon-Like Peptide 1 Receptor Agonists and 13 Obesity-Associated Cancers in Patients with Type 2 Diabetes. JAMA Netw. Open 2024, 7, e2421305. [Google Scholar] [CrossRef]
- Rodolakis, A.; Scambia, G.; Planchamp, F.; Acien, M.; Sardo, A.D.S.; Farrugia, M.; Grynberg, M.; Pakiž, M.; Pavlakis, K.; Vermeulen, N.; et al. ESGO/ESHRE/ESGE Guidelines for the fertility-sparing treatment of patients with endometrial carcinoma. Facts Views Vis. Obgyn 2023, 15, 3. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Definition | |
|---|---|
| WHO (1999) [14] | Insulin resistance is defined as type 2 diabetes mellitus (DM) or impaired fasting glucose (IFG) (>100 mg/dL) or impaired glucose tolerance (IGT), plus two of the following: Abdominal obesity (waist-to-hip ratio > 0.9 in men or >0.85 in women, or BMI > 30 kg/m2. Triglycerides 150 mg/dL or greater, and/or high-density lipoprotein (HDL)-cholesterol < 40 mg/dL in men and <50 mg/dL in women. Blood pressure (BP) 140/90 mmHg or greater. Microalbuminuria (urinary albumin secretion rate 20 μg/min or greater, or albumin-to-creatinine ratio 30 mg/g or greater). |
| IDF (2005) [1] | Central obesity (defined as waist circumference but can be assumed if BMI > 30 kg/m2) with ethnicity-specific values *, plus two of the following: Triglycerides 150 mg/dL or greater. HDL-cholesterol < 40 mg/dL in men and <50 mg/dL in women. BP 130/85 mmHg or greater. Fasting glucose 100 mg/dL or greater. |
| NCEP:ATPIII (2001) [12] | Any three or more of the following: Waist circumference > 102 cm in men, >88 cm in women. Triglycerides 150 mg/dL or greater. HDL-cholesterol < 40 mg/dL in men and <50 mg/dL in women. BP 130/85 mmHg or greater. Fasting glucose 100 mg/dL or greater. |
| Consensus (2009) [13] | Any three of the following: Elevated waist circumference (according to population and country-specific definitions). Triglycerides 150 mg/dL or greater. HDL-cholesterol < 40 mg/dL in men and <50 mg/dL in women. BP 130/85 mmHg or greater. Fasting glucose 100 mg/dL or greater. |
| Control n = 174,097 | EC n = 1454 | p-Value (Mann-U) | |
|---|---|---|---|
| Follow-up (years) median (IQR) | 11.9 (11.2–12.6) | 6.2 (3.6–9.1) | <0.001 |
| Ethnicity n (%) | |||
| White | 162,146 (92.4) | 1354 (93.1) | <0.001 |
| Mixed | 1371 (0.8) | 7 (0.5) | <0.001 |
| Asian/Asian British | 3516 (2.0) | 36 (2.4) | <0.001 |
| Black/Black British | 3274 (2.1) | 17 (1.2) | <0.001 |
| East Asian | 788 (0.4) | 4 (0.3) | <0.001 |
| Other | 1909 (1.1) | 22 (1.5) | <0.001 |
| NA—Not answered n (%) | 1093 (0.6) | 14 (1.0) | <0.001 |
| Index of deprivation (England) median (IQR) | 12.9 (7.4–23.3) | 14.0 (8.0–23.6) | <0.001 |
| Age at recruitment median (IQR) | 55.0 (48.0–62.0) | 60.0 (54.0–64.0) | <0.0001 |
| Height (cm) mean (SD) | 162.6 (6.4) | 162.0 (6.2) | 0.0002 |
| Height missing n (%) | 754 (0.4) | 6 (0.4) | NS |
| Weight (kg) median (IQR) | 68.5 (61.2–77.9) | 76.7 (67.1–90.9) | <0.0001 |
| Weight missing n (%) | 892 (0.5) | 7 (0.5) | NS |
| Waist circumference (cm) median (IQR) | 82 (75–91) | 91 (81–102) | <0.0001 |
| Waist circumference missing n (%) | 719 (0.4) | 4 (0.3) | |
| BMI (kg/m2) median (IQR) | 25.8 (23.2–29.4) | 29.4 (25.4–34.9) | <0.0001 |
| BMI missing n (%) | 2395 (1.4) | 8 (0.6) | <0.0001 |
| Age at menarche median (IQR) | 13.0 (12.0–13.0) | 13.0 (12.0–14.0) | <0.0001 |
| Pre-menopausal, n (%) | 55,260 (33.6) | 251 (18.1) | <0.0001 |
| Post-menopause, n (%) | 109,120 (66.4) | 1134 (81.9) | <0.0001 |
| Menopause missing n (%) | 9717 (5.6) | 69 (4.8) | <0.0001 |
| Age at menopause median (IQR) | 51.0 (48.0–53.0) | 52.0 (50.0–55.0) | <0.0001 |
| Nulliparous n (%) | 35,745 (20.5) | 365 (25.1) | <0.0001 |
| Oral contraceptive pill (OCP) used n (%) | 142, 452 (81.9) | 1023 (70.4) | <0.0001 |
| OCP never used n (%) | 31,163 (17.9) | 427 (29.7) | <0.0001 |
| OCP data missing | 392 (0.2) | 4 (0.3) | NS |
| Hormone replacement therapy (HRT) used n (%) | 50,556 (29.0) | 525 (36.1) | <0.0001 |
| HRT never used n (%) | 123,149 (70.7) | 925 (63.6) | <0.0001 |
| HRT data missing | 392 (0.2) | 4 (0.3) | |
| Never smoked n (%) | 106,094 (60.9) | 967 (66.5) | <0.0001 |
| Ex-smoker n (%) | 52,105 (29.9) | 410 (28.2) | <0.0001 |
| Current smoker n (%) | 14,929 (8.6) | 68 (4.7) | <0.0001 |
| Smoking status missing n (%) | 969 (0.6) | 9 (0.6) | NS |
| Diabetes mellitus (DM)—any n (%) | 5650 (3.3) | 117 (8.1) | <0.0001 |
| Diabetes status missing | 861 (0.5) | 13 (0.9) | <0.0001 |
| Taking cholesterol lowering medication n (%) | 17,795 (10.3) | 268 (18.7) | <0.0001 |
| Anti-hypertensives n (%) | 15,295 (8.9) | 217 (15.1) | <0.0001 |
| Polycystic ovarian syndrome n (%) | 263 (0.2) | 4 (0.3) | <0.001 |
| Controls n = 174,097 | EC n = 1454 | p-Value (Mann-U) | |
|---|---|---|---|
| BMI ≥ 30 kg/m2 (%) | 38,235 (22.0) | 663 (45.6) | <0.001 |
| Waist Circumference ≥ 80 cm (%) | 54,148 (31.1) | 810 (55.7) | <0.001 |
| Waist-to-Hip ratio ≥ 0.85 (%) | 49,993 (28.7) | 609 (41.9) | <0.001 |
| Arterial BP ≥ 130/85 mmHg (%) | 47,600 (27.3) | 522 (35.9) | <0.001 |
| HbA1c ≥ 48 mmol/mol (%) | 3706 (2.1) | 75 (5.2) | <0.001 |
| Fasting Glucose ≥ 100 mg/dL (%) | 20,391 (11.7) | 242 (16.6) | <0.001 |
| Triglycerides ≥ 150 mg/dL (%) | 46,977 (27.0) | 598 (41.1) | <0.001 |
| HDL Cholesterol ≤ 50 mg/dL (%) | 57,654 (33.1) | 614 (42.2) | <0.001 |
| MetS (WHO 1998) (%) | 9051 (5.2) | 160 (11.0) | <0.001 |
| MetS (NCEP:ATPIII 2001) (%) | 28,916 (16.6) | 500 (34.4) | <0.001 |
| MetS IDF (2005) (%) | 36,711 (21.1) | 552 (38.0) | <0.001 |
| Consensus MetS (2009) (%) | 37,972 (21.8) | 569 (39.1) | <0.001 |
| HR | 95.0% CI for HR | p | SE | |
|---|---|---|---|---|
| WHO (1998) [14] | 1.928 | 1.633–2.276 | <0.001 | 0.085 |
| IDF (2005) [1] | 2.080 | 1.869–2.314 | <0.001 | 0.054 |
| NCEP:ATPIII (2001) [12] | 2.385 | 2.138–2.659 | <0.001 | 0.056 |
| Consensus (2009) [13] | 2.091 | 1.880–2.325 | <0.001 | 0.054 |
| Pre-Menopausal N = 249 | Post Menopausal N = 1201 | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95.0% CI for HR | p | SE | HR | 95.0% CI for HR | p | SE | |
| Age at menarche | 0.928 | 0.857–1.004 | 0.064 | 0.041 | 0.912 | 0.879–0.945 | <0.001 | 0.018 |
| Nulliparity | 1.779 | 1.374–2.304 | <0.001 | 0.234 | 1.233 | 1.068–1.423 | 0.004 | 0.090 |
| Ever used contraception | 0.757 | 0.549–1.045 | 0.091 | 0.164 | 0.760 | 0.667–0.866 | <0.001 | 0.066 |
| Ever used HRT | 0.866 | 0.673–1.115 | 0.266 | 0.129 | 1.006 | 0.894–1.132 | 0.922 | 0.060 |
| Smoking | 1.594 | 1.198–2.122 | 0.001 | 0.146 | 0.752 | 0.671–0.843 | <0.001 | 0.058 |
| Waist circumference > 80 cm | 1.104 | 0.820–1.486 | 0.513 | 0.152 | 2.165 | 1.910–2.454 | <0.001 | 0.064 |
| Triglycerides > 150 mg/dL | 1.534 | 1.182–1.991 | 0.001 | 0.133 | 1.228 | 1.089–1.386 | <0.001 | 0.062 |
| HDL < 50 mg/dL | 1.199 | 0.909–1.581 | 0.200 | 0.141 | 1.188 | 1.054–1.339 | 0.005 | 0.061 |
| BP > 130/85 mmHg | 1.016 | 0.664–1.552 | 0.943 | 0.217 | 1.109 | 0.985–1.250 | 0.087 | 0.061 |
| Glucose > 100 mg/dL | 0.928 | 0.415–2.076 | 0.856 | 0.411 | 1.021 | 0.870–1.198 | 0.803 | 0.082 |
| HbA1c > 48 mmol/mol | 1.511 | 1.078–2.119 | 0.017 | 0.172 | 1.288 | 0.986–1.682 | 0.063 | 0.136 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karkia, R.; Maccarthy, G.; Payne, A.; Karteris, E.; Pazoki, R.; Chatterjee, J. The Association Between Metabolic Syndrome and the Risk of Endometrial Cancer in Pre- and Post-Menopausal Women: A UK Biobank Study. J. Clin. Med. 2025, 14, 751. https://doi.org/10.3390/jcm14030751
Karkia R, Maccarthy G, Payne A, Karteris E, Pazoki R, Chatterjee J. The Association Between Metabolic Syndrome and the Risk of Endometrial Cancer in Pre- and Post-Menopausal Women: A UK Biobank Study. Journal of Clinical Medicine. 2025; 14(3):751. https://doi.org/10.3390/jcm14030751
Chicago/Turabian StyleKarkia, Rebecca, Gideon Maccarthy, Annette Payne, Emmanouil Karteris, Raha Pazoki, and Jayanta Chatterjee. 2025. "The Association Between Metabolic Syndrome and the Risk of Endometrial Cancer in Pre- and Post-Menopausal Women: A UK Biobank Study" Journal of Clinical Medicine 14, no. 3: 751. https://doi.org/10.3390/jcm14030751
APA StyleKarkia, R., Maccarthy, G., Payne, A., Karteris, E., Pazoki, R., & Chatterjee, J. (2025). The Association Between Metabolic Syndrome and the Risk of Endometrial Cancer in Pre- and Post-Menopausal Women: A UK Biobank Study. Journal of Clinical Medicine, 14(3), 751. https://doi.org/10.3390/jcm14030751