Abstract
Background/Objectives: Pain science education accommodating low health literacy is needed for people with chronic pain. The purpose of this study was to translate PNE4Kids, contextually adapt it into PNE4Adults, and test the feasibility of the newly developed pain science education program (PNE4Adults) for adult patients with chronic musculoskeletal pain in the municipality. Methods: A three-step approach was used to (1) translate PNE4Kids into Danish, (2) adapt to age and context (PNE4Adults), and (3) test the feasibility. (1) Translation was performed by a native Dane fluent in Dutch. (2) Two think-aloud group sessions were held, with therapists and end users. (3) Feasibility was tested amongst twenty adult patients with chronic musculoskeletal pain consecutively referred for rehabilitation in the municipality. The a priori success criteria were determined to be 70% acceptability and 70% understandability. Prior to inclusion of the first patient, the study was pre-registered on clinicaltrial.gov [NCT05140031]. Results: Translation was successfully performed. Both the therapist and end users found the program easy to grasp, the simplicity and interactive nature of the program ingenious, and the program to be well suited to an adult population. All patients (100%), across health literacy levels, found PNE4Adults comprehensible and acceptable. Conclusions: The aims were successfully met. Progression to a full trial is warranted and is underway.
1. Introduction
According to the World Health Organization (WHO), 20–33% of the world’s population lives with painful musculoskeletal (MSK) conditions [1]. As the costs due to MSK pain correspond to almost 2% of the gross domestic products of European countries [2], these pain conditions pose a challenge for healthcare systems globally [3,4]. Patients with chronic MSK pain have high use of healthcare, reduced work ability, functional limitations in their daily lives, and diminished quality of life [5,6,7]. Current care guidelines recommend that pain science education (PSE) [8]—also called, e.g., therapeutic neuroscience education [9,10], pain neuroscience education [11,12], or explain pain [13]—is a vital part of the care delivered to individuals suffering from chronic pain [13,14,15,16,17,18,19,20]. These programs aim to reconceptualize pain and enhance biopsychosocial rehabilitation [21,22].
On a patient level, PSE has been shown to reduce patients’ pain intensity, pain catastrophizing, and fear avoidance in addition to improved physical functioning, self-efficacy, and pain knowledge [23,24,25], especially in combination with other therapies [11,26]. Combining exercise and PSE shows greater short-term improvements in pain, disability, kinesiophobia, and pain catastrophizing compared to exercise alone [16]. On a societal level, PSE has been shown to reduce health expenses [25,27]. However, some of the proposed barriers include training of the therapist delivering the education [28,29,30,31], access to training materials [32], time during consultation, and patient health literacy levels [33,34]. Despite PSE’s wide recognition in the scientific literature, implementing it in a clinical context has proven difficult [30]. Physiotherapist do not feel competent in delivering this type of biopsychosocial intervention [35,36,37] and current PSE materials may be too complex [34,38]. In Denmark, where the population is generally highly educated, nearly 4 out of 10 people face difficulties accessing, understanding, appraising, and applying health information [33]. This underlines the need to consider novel ways of delivering PSE across all levels of health literacy [32].
Recently, Pas et al. (2018) developed a Dutch PSE program to teach children with chronic pain (and their parents) about the underlying biopsychosocial mechanisms of pain, called PNE4Kids [39,40]. The PNE4Kids program consists of a manual for therapists and a board game to enhance engagement and participant involvement. It provides an easy and accessible way for the patient to grasp the concept of pain and shows promise in reducing disability and pain-related fear in children [41]. This new PSE program may also hold promise for adult patients, including those with low levels of health literacy, and enhance learning due to the practical approach. As highlighted by Wittink, H. and Oosterhaven, J., 2018, using universal health literacy precautions is recommended by multiple professional organizations for all patients, regardless of education level or health literacy [42]. Before further effectiveness testing of the program, adequate adaptation and feasibility testing in the adult population is needed, as recommended in the updated Medical Research Counsel Framework [43]. The main aim of this study was to translate and adapt the existing PNE4Kids program into an adult Danish version (“PNE4Adults”) and test the feasibility of the program among adult patients suffering from chronic MSK pain and currently undergoing community-based rehabilitation.
2. Materials and Methods
2.1. Design
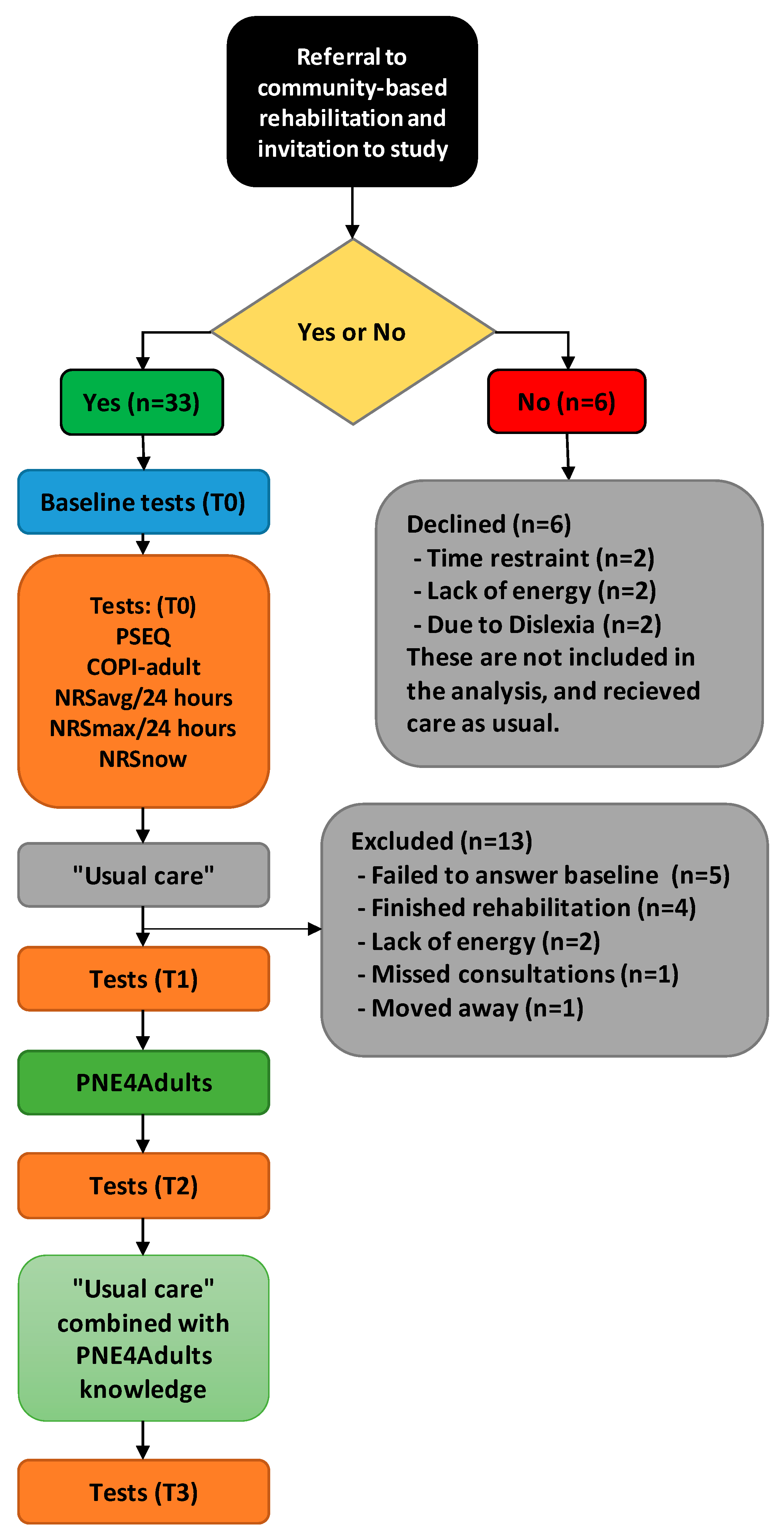
We used a three-step approach to conduct translation, adaptation, and testing of feasibility. Step 1: translation of the PNE4Kids manual into Danish; step 2: contextual adaptation to an adult version, including two consecutive “think-aloud sessions”, one with physiotherapists and occupational therapists, and one with adult, chronic pain patients; and step 3: feasibility testing in a cross-over inspired design (Figure 1) after completion of the first two steps.
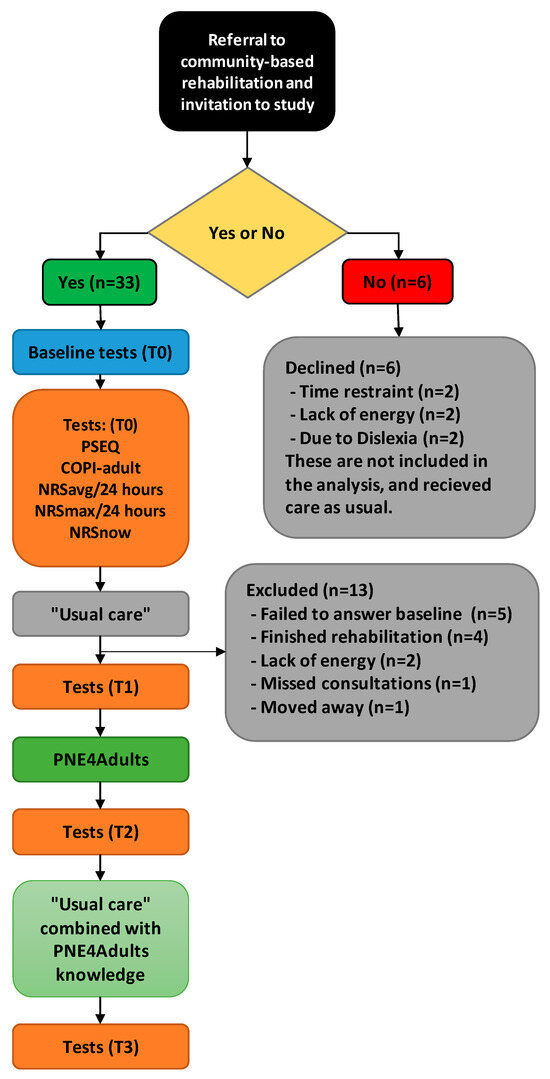
Figure 1.
Flowchart of inclusion. ‘T0’: Timepoint 0, before first consultation, ‘T1’: Timepoint 1, after “usual care” before PNE4Adults, ‘T2’: Timepoint 2, after PNE4Adults, ‘T3’: Timepoint 3, after additional “usual care” combined with knowledge from PNE4Adults. ‘PSEQ’: Pain Self Efficacy Questionnaire, ‘COPI-Adult’: Concept Of Pain Inventory for adults, ‘NRS’: Numeric Rating Scale, ‘NRSavg’: The average pain in the last 24 h, ‘NRSmax’: The maximum pain in the last 24 h, ‘NRSnow’: The current pain, “Usual care”: routinely care received in the municipality, ‘PNE4Adults’: Pain science education.
2.2. Setting and Context
This study was conducted at a high-volume community-based rehabilitation center in Denmark. Each year, approximately 1000 patients with MSK pain are referred for rehabilitation. Both the patients and the therapists involved in the study were from the rehabilitation center.
2.3. Methods
2.3.1. Step 1: Translation of the PNE4Kids Program from Dutch into Danish
The original Dutch version of the PNE4Kids program was translated into Danish by a native Danish-speaking physiotherapist with no prior knowledge of pain science or the PNE4Kids program. The translator was fluent in Dutch. In an online meeting between the first author and the original authors of PNE4Kids, the new Danish version was then discussed and triangulated with the published English version for comparison of meaning. Since it was a translation of a manual of 11 pages to guide PSE rather than a questionnaire, we did not use a dual panel or forward–backward translation during this process. While psychometric testing is essential for tools like questionnaires, it is not applicable to the PNE4Adults program, which is a structured manual-based intervention. Its validity is supported by its theoretical foundation and alignment with established frameworks. The “PNE” part of the program’s name was retained for easy recognition.
2.3.2. Step 2: Contextual Adaptation of PNE4Kids into PNE4Adults
We conducted a think-aloud session to adapt the PNE4Kids program into a version applicable for adult patients. We invited a group of Danish physiotherapists and occupational therapists, all healthcare professionals from the community center rehabilitation facility, with a self-reported good understanding of contemporary pain science and who had all undergone a pain science course of 48 h. See Appendix A, Table A1 for the characteristics of the participants. Prior to the think-aloud group session, the manual was forwarded to the participants to be read in advance. The think-aloud session was held in person and lasted for 1.5 h. Each part of the manual was discussed thoroughly during the session and any thoughts, uncertainties, and opinions were voiced and considered amongst the group. The session was audio-recorded and transcribed. Any suggestions for changes were talked through until consensus was reached. If consensus was not reached, the suggestion was noted and discussed within an end user group (see next section). This involved both changes with regards to the Danish adaptation but also changes related to the altered age group (i.e., the transition from children to adult patients).
After the initial think-aloud session, we used an external end user group of Danish adult patients with chronic pain to test the manual and the board game [39]. See Appendix A, Table A2 for their characteristics. The health literacy status for Panel 2 can be seen in Appendix A, Table A3, and it includes patients with low degrees of health literacy, measured with the Health Literacy Questionnaire [44]. These patients had previously attended an extensive PSE program of 10 weeks, which included pain neurophysiology and learning about the biopsychosocial aspects of pain and possibilities of self-management. The end user group did not view the manual but underwent PNE4Adults as an educational session. The group members were encouraged to voice any thoughts, questions, uncertainties, and ideas about PNE4Adults. The discussion was once again facilitated through open-end questions and was audio-recorded and subsequently transcribed.
2.3.3. Step 3
Feasibility Study of PNE4Adults
To understand the feasibility of PNE4Adults in routine clinical practice, as well as the feasibility of obtaining answers on outcome scores, we then implemented the program during a 20-week period. We included patients who were referred to rehabilitation in the municipality suffering from chronic MSK pain, with no knowledge requirement on PSE. Prior to inclusion of the first patient, the study was pre-registered on clinicaltrial.gov [NCT05140031]. Furthermore, approval was sought by the Scientific Ethics Committee for Region North Jutland (Journal number 2021-000438), and approval was waived on 3 September 2021 for this project on the basis that it was not covered by the Committee Acts (Act no. 1338 of 01/09/2020) definition of a health sciences research project according to Danish legislation.
Eligible patients were Danish-speaking adult patients (≥18 years) with chronic MSK pain (pain persisting or recurring for ≥3 months) [45] who were cognitively able to complete the program and had no confirmed medical diagnosis indicated or related to any intellectual disorder. Recruitment was stopped when the target of 20 patients had completed the program. Twenty patients were estimated to fulfill the reasonable evaluation of the feasibility goals [46]. As part of routine practice, patients were called in for a first-time rehabilitation consultation per telephone by the secretaries. Eligible patients were informed of the project and invited to participate. If they consented, an e-link to the first battery of questionnaires was sent via secure email (e-Boks), which were filled out before the initial consultation. After informed consent from the patient was obtained, they underwent “usual rehabilitation”. Usual rehabilitation included goal setting and subsequent rehabilitation using cardio and strengthening exercises toward achieving the determined goals. After approximately 14 days, they were introduced to PNE4Adults during one or two sessions, each lasting for 45–60 min. The patients were then followed up with approximately 14 days of usual rehabilitation combined with the knowledge obtained during the PNE4Adults sessions (Figure 1). The intervention, as well as subsequent rehabilitation, were in all cases delivered by the first author (BE), who holds a Master of Pain Science and Multidisciplinary Pain Management.
Procedure During the Feasibility Study
Usual rehabilitation included a patient interview with individual goal setting and subsequent rehabilitation using aerobic exercises and strengthening exercises toward achieving the determined goals. We added individual PSE in the form of PNE4Adults after approximately 14 days of usual rehabilitation and subsequently continued with usual rehabilitation combined with integrating the knowledge obtained through the PNE4Adults session. The PNE4Adults session followed the developed manual (which is available at https://paininmotion.be/pne4kids (accessed on 17 May 2023) [39] and explained in brief in Appendix B) and each session lasted for 45–60 min. Firstly, the function of a normal pain system was introduced, with examples of pain being overly or under protective. The patient then taught back, giving the therapist the opportunity to evaluate the understanding and, if necessary, repeat essential key messages. Secondly, the sensitized pain system was explained. Thirdly, the person in question was asked to reflect on this new information in relation to his/her own situation and the new knowledge was subsequently integrated in the “usual rehabilitation” with any individually targeted additional measures that needed to be included, e.g., graded exposure, stress relief, graded activity, and cognitive therapies.
Data Collection and Outcomes for the Feasibility Study
Questionnaire-based data were collected via REDCap® version 10.0.23 © 2022 Vanderbilt University and stored at a secure server at Aalborg University. Comprehensibility and acceptability were the primary feasibility outcomes. Baseline questionnaires included socio-demographic data (i.e., age, sex, marital status, work status, education level), pain duration (months), average and worst pain intensity the last 24 h, as well as current pain intensity (Numeric Rating Scale, NRS [47]). Additional baseline data included the level of symptoms related to central sensitization (Central Sensitization Inventory, CSI [48,49]), health literacy status (Health Literacy Questionnaire, HLQ [44]), pain-related knowledge (Concept of Pain, COPI-Adult [50]), pain self-efficacy (Pain Self-Efficacy Scale, PSEQ [51,52]), and pain catastrophizing (Pain Catastrophizing Scale, PCS [53]) (see specified description in Appendix B). At each of the three follow-ups (T1, T2, and T3), we included the COPI-Adult, the PSEQ, the PCS, and the three NRS measures (see Figure 1). Given that this was a feasibility study, the primary focus was on assessing acceptability and comprehensibility rather than measuring changes in outcomes. As such, no a priori hypotheses were established, nor were sample size calculations conducted for statistical testing. This aligns with the exploratory nature of the study, which prioritized gathering preliminary data to inform future research rather than testing effectiveness.
Comprehensibility of the PNE4Adults
The comprehensibility of PNE4Adults was measured by a participant questionnaire on a 7-point scale ranging from “very incomprehensible”, “incomprehensible”, “slightly incomprehensible”, “neither incomprehensible nor comprehensible”, “slightly comprehensible”, “comprehensible”, to “very comprehensible”. This approach only allowed us to assess if the patients found the intervention (PNE4Adults) comprehensible, and not the value of the intervention, which was clearly stated. The comprehensibility was categorized as “incomprehensible” if rated from “very incomprehensible” to “neither incomprehensible nor comprehensible” (options 1–4) and as “comprehensible” if rated from “slightly comprehensible” to “very comprehensible” (options 5–7). At least 70% of the participants should find it “comprehensible” to rate the intervention as comprehensible, which exceeded the threshold of 50% in a previous feasibility trial on understandability [54], for us to justify using a translated and adapted model initially intended for children.
Acceptability of the PNE4Adults
Acceptability of the combined intervention of PNE4Adults and usual care was assessed by a participant acceptability questionnaire on a 7-point scale ranging from “very unacceptable”, “unacceptable”, “slightly unacceptable”, “neither unacceptable nor acceptable”, “slightly acceptable”, “acceptable”, to “very acceptable”. This approach only allowed us to investigate if the added intervention (PNE4Adults) was acceptable to the patient, and not if the added intervention made a difference to the outcome of the rehabilitation. The acceptability was categorized as “unacceptable” if rated from “very unacceptable” to “neither unacceptable nor acceptable” (options 1–4) and as “acceptable” if rated from “slightly acceptable” to “very acceptable” (options 5–7). The intervention was rated as acceptable if at least 70% of the participants found it acceptable.
3. Results
3.1. Step 1: Translation
The translated program was discussed with the authors of the original version to clarify differences in the translation, and consensus was reached. Alterations to contextually adapt the program to an adult population included: (1) changing the example used in the first explanation of how the nociceptive system works in case of injury, (2) referring to a real-life example (in these cases, a famous cyclist who won a Tour de France stage with a broken collarbone and a case with a worker who stepped on a nail), and (3) changing the age of the case example in the final part of the program to match the adult population. Consensus was reached on all accounts.
3.2. Step 2: Contextual Adaptation
3.2.1. Think-Aloud Session with Therapists
All participants were overall positive toward the PNE4Adults program (n = 6) (see Appendix A). Further, all agreed that the visual and interactive presentation and possibility of teach-back would most likely enhance learning. Also, having the board game rather than having to depend on individual drawing skills was much preferred. There was consensus that a good understanding from the therapist presenting the program was needed to present it in a clear and concise manner. One person expressed concerns that the simplicity of the program would be too childish for some adults; however, the majority disagreed with this notion, claiming that this would depend highly on individual preference. All participants approved of the alterations that were made to adapt the program to an adult population. The military as a metaphor was thoroughly discussed as some did not understand the hierarchy of the military, which confused their understanding of the metaphor. However, consensus was reached that this metaphor worked well. In Danish, the word “defense” can be used synonymously for the military, and it was agreed that this word should be presented to the patient group, since this aligns with the positive purpose of the pain system.
3.2.2. Think-Aloud Session with End Users
The patients from the end user group found the program easy to understand and not childish (n = 5) (see Appendix A). They valued the visual and interactive nature of the program and two of the patients (with low levels of health literacy) said that they really understood pain neurophysiology for the first time after it being presented in the form of PNE4Adults. The program generated reflections on the patients’ own pain experiences and behaviors, and they emphasized that the understanding gave the patients a big responsibility for managing their own pain. Further, the patients agreed that the Danish term “defense” for military held a more positive and protective meaning to them compared to “military”. All patients found the program comprehensible, relevant, and acceptable, including those with low degrees of health literacy.
3.3. Step 3: Feasibility Study
From 11 November 2021 to 22 March 2022, 39 patients were referred to the current study. Six patients declined to participate due to time restraints (n = 2), lack of energy (n = 2), and because they felt their dyslexia prevented them from adequately answering the questionnaires (n = 2), despite being offered the possibility of assistance reading them, and are not part of the analysis. As seen in Figure 1, the remaining 33 patients answered the questionnaire the first time, but 13 were excluded because they did not complete the questionnaire before the first consultation (due to the short time frame, not lack of interest) (n = 5); discontinued their rehabilitation before undergoing the PNE4Adults program (because their goals had already been met) (n = 4); moved to a new town (n = 1); or withdrew after the first questionnaire, stating that they did not have the energy to participate after all (n = 2) or had a long period of COVID-19 disease and several appointment cancellations (n = 1). All were excluded before undergoing the PNE4Adults program. This left 20 patients, as pre-defined, who completed the study and were included in the analysis. One patient failed to fill out the questionnaire at T1 (before PNE4Adults) and T2 (after PNE4Adults), and another failed to fill out the last questionnaire at T3 (after the final interview), because the follow-up questionnaires for these patients ended up in their SPAM folder. At each of the three follow-ups (T1, T2, and T3), the patients answered the COPI-Adult, the PSEQ, the PCS, and the three NRS measures (see Figure 1).
The baseline demographics of the participants are outlined in detail in Table 1.

Table 1.
Baseline data (n = 20).
Table 1 shows that the sample had a wide age range, equal gender distribution, and some variation in educational levels. In total, 45% of participants were still working, 55% of the participants had pain for more than 1 year, and 25% had co-morbidities.
The health literacy status is outlined in Table 2.
Table 2.
Health Literacy Questionnaire (HLQ) of participants in the feasibility study (n = 20).
Table 2 shows that more than 50% of all included patients scored below 3.5 in Part 2 of the HLQ, indicating low levels of health literacy, being passive in their approach to healthcare, and having problems understanding any written information in relation to their health. Additionally, 25% scoring below 2.5 in Part 1 of the HLQ also indicated low levels of health literacy in the domains of actively managing their health and having difficulty engaging with healthcare providers.
Table 3 shows the results for the outcome measures for the feasibility study. All patients (100%) found the PNE4Adults intervention to be acceptable and comprehensible, hence exceeding the pre-defined success criteria of 70% for each outcome. There was no relevant difference in acceptability and comprehensibility between patients with different health literacy levels. In all three pain measures (NRSavg, NRSmax, NRSnow), decreases were observed on a group level from T0 to T3. Furthermore, increases in pain knowledge and pain self-efficacy were observed from T0 to T3 on a group level based on the COPI-Adult [50] and PSEQ [51] scores, respectively. Lastly, pain catastrophizing measured on the PCS [53] decreased on a group level from T0 to T3.
Table 3.
Outcome measures (n = 20).
4. Discussion
4.1. Explanation of Findings
Translation into the Danish language was successful. Both the therapists and the patients with chronic pain indicated that the program gave them a sense of “finally getting it” and liked the interactive nature of it. The patients claimed that it resulted in reflections on their own situation and gave them a sense of ownership of their situation. From the results of the current feasibility study, we found that all patients found the PNE4Adults program to be acceptable and comprehensible, including those with low levels of health literacy.
4.2. Comparison with Previous Findings
PSE has been used in several feasibility studies across different age groups. These studies have primarily investigated the feasibility of using PSE as part of a rehabilitation program in the context of exploring the feasibility of running a definitive trial. In general, it appears that different forms of PSE are well accepted among patients with long-standing pain [16,40,54,55,56]. Feasibility studies also indicate that PSE is credible [57] and well accepted among younger patients, adults, and older adults. However, in a randomized feasibility study with adult patients (+50 years of age) suffering from osteoarthritic pain, Stanton et al. [38] observed that both clinicians and patients found that the PSE intervention (i.e., “Explain Pain”, “Protectometer”, and multimedia resources) was too complex. In a recent qualitative study by Oosterhaven et al., 2023, conducted with an interdisciplinary pain management program, they found that most participants had difficulties understanding the messages of the pain neuroscience education and could not integrate it in their daily lives. They concluded that health literacy levels most likely played a role [34]. As such, a simplified version of PSE was warranted, and this study now provides the first evidence of patient and clinician perspectives. Our findings of feasibility add to the current knowledge base and indicate that for individuals where written materials may be insufficient, the PNE4Adults program (including the board game) may be a viable alternative to solely written and verbal information and may also be relevant for people with low levels of health literacy.
4.3. Clinical Implications
Previous approaches to teach patients PSE have primarily been based on video resources, leaflets, and communication and knowledge transmission from a trained clinician [57]. The combined results from both the quantitative and qualitative analyses suggest that using PNE4Adults to communicate and teach adults about pain science is feasible, acceptable, and motivating for adult patients with chronic MSK pain. As one of the themes from the think-aloud sessions showed, participants had the sense of “I finally get it”, which may hold promise for patients with different levels of health literacy. It is often difficult to include the most vulnerable patients and patients with low levels of health literacy. These patients may have additional challenges and thereby be more susceptible to the PNE4Adults program compared to existing PSE programs due to a greater focus on practical learning and no requirements for reading skills. In this study, we successfully included some patients with low levels of health literacy, representative of the background population in Denmark, and there was no difference between those with low levels of health literacy and the rest in terms of finding the program acceptable and comprehensible, indicating that this mode of delivering PSE is also relevant for this population. Including the program during the usual educational sessions may add time or take time away from other activities. Future studies are needed to understand if this added time, or relocation of time away from other aspects of rehabilitation, is associated with better outcomes compared to not using PNE4Adults.
4.4. Limitations
The current study was conducted among patients referred to rehabilitation in the municipality. The aim was to use consecutive recruitment, but due to COVID-19 and associated complications, it was not possible to ask all consecutively referred participants. This may affect the generalizability of the findings but is unlikely to affect our conclusions on feasibility, as patients not being asked did not decline due to the content of the intervention. It is possible that PNE4Adults may not translate into other languages or cultural differences may limit its use in other countries. We acknowledge the potential for gender bias due to the all-female composition of the patient think-aloud group in Step 2. However, this group was representative of the demographics of the patients available at the time. Importantly, male perspectives were included through the think-aloud group of healthcare providers, and Step 3 ensured a 50% gender mix. Additionally, the adaptations made in Step 2 were minor and focused on refining language and presentation, with no changes specific to gender-related aspects. While this limitation should be considered, we believe it has minimal impact on the overall findings. A further limitation is that all interventions were delivered by the first author. In a subsequent randomized controlled trial, the interventions should be delivered by other physiotherapists to avoid this bias.
5. Conclusions
The PNE4kids program was successfully translated into Danish and adapted in terms of age and context into the PNE4Adults program through think-aloud sessions with therapists and patients with chronic MSK pain from a municipality setting. The PNE4Adults program was found to be acceptable, comprehensible, and feasible for use in a municipality setting. Further research is needed with a randomized controlled trial with a large enough sample size to have statistical power to evaluate the effectiveness of the program.
Author Contributions
Conceptualization, B.E., M.S.R., K.I., E.R. and C.L.S.; methodology, B.E., M.S.R., K.I., E.R. and C.L.S.; software, B.E., M.S.R. and C.L.S.; validation, B.E., M.S.R., K.I., E.R. and C.L.S.; formal analysis, B.E. and C.L.S.; investigation, B.E.; resources, B.E.; data curation, B.E.; writing—original draft preparation, B.E. and C.L.S.; writing—review and editing, B.E., M.S.R., K.I., E.R. and C.L.S.; visualization, B.E. and C.L.S.; supervision, K.I., M.S.R. and C.L.S.; project administration, B.E.; funding acquisition, B.E., M.S.R., K.I., E.R. and C.L.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Danske Fysioterapeuters Praksisudviklingsfond grant number R35-A728. Grant support for Emma Rheel was provided by a chair funded by the Berekuyl Academy/European College for Decongestive Lymphatic Therapy, the Netherlands, and awarded to the Vrije Universiteit Brussels, Belgium.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Approval was sought by the Scientific Ethics Committee for Region North Jutland (Journal number 2021-000438), and approval was waived on 3 September 2021 for this project on the basis that it was not covered by the Committee Acts (Act no. 1338 of 1 September 2020) definition of a health sciences research project and must therefore not be notified to and approved by the committee, cf. section 14, subsection of the Committees Act. 1, cf. Section 2, nos. 1–3 according to Danish legislation.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the patient(s) to publish this paper.
Data Availability Statement
Restrictions apply to the availability of these data. Data were obtained from Køge Kommune and are available from the authors with the permission of Køge Kommune.
Conflicts of Interest
Kelly Ickmans co-developed the original PNE4Kids program, which is available for purchase; however, the royalties are collected be the Vrije Universiteit Brussels and not by her personally. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A. Tables of Participant Characteristics in Think-Aloud Sessions
Table A1.
Panel 1: Therapists knowledgeable in pain science (n = 6).
Table A1.
Panel 1: Therapists knowledgeable in pain science (n = 6).
| Characteristic | Measurement | Mean (±SD) or No. (%) |
|---|---|---|
| Age | Years, mean (±SD) Range | 37.8 (±7.36), 31–50 years |
| Sex | Female | 4 (66.7) |
| Marital status | Married, n (%) | 6 (100) |
| Work experience | Years, Mean (±SD) | 13.3 (±7.20) |
| Education | Physiotherapist | 5 (83.3) |
| Occupational therapist | 1 (16.7) |
‘SD’: Standard Deviation; ‘No’: Number.
Table A2.
Panel 2: Patients with chronic pain (n = 5).
Table A2.
Panel 2: Patients with chronic pain (n = 5).
| Characteristic | Measurement | Mean (±SD) or No. (%) |
|---|---|---|
| Age | Years, mean (±SD) Range | 58.6 (±6.58), 53–70 years |
| Sex | Female | 5 (100) |
| Marital status | Married, n (%) | 5 (100) |
| Level of education |
| 0 (0) 0 (0) 2 (40) 3 (60) 0 (0) |
| Work status | Working, n (%) | 1 (20) |
| Pain duration | Years, Mean (±SD) | 4.8 (±0.83) |
| Pain intensity | NRSavg/last 24 h, Mean (±SD), Range | 5.6 (±1.81) 3–8 |
‘SD’: Standard Deviation; ‘No’: Number; ‘NRS’: Numeric Rating Scale, ‘NRSavg’: The average pain in the last 24 h.
Table A3.
Health literacy status of Panel 2, patients with chronic pain (n = 5).
Table A3.
Health literacy status of Panel 2, patients with chronic pain (n = 5).
Part 1 *
| Mean (±SD) n/N [min–max] 3.15 (±0.10), 0/5 [3–3.75] 2.95 (± 0.30), 1/5 [2.25–3.25] 3.16 (±0.42), 0/5 [2.6–3.6] 2.96 (±0.55), 2/5 [2.2–3.8] 2.76 (±0.57), 1/5 [2.4–3.2] 3.56 (±0.38), 3/5 [2.8–4.6] 3.37 (±0.58), 1/5 [3.1–3.6] 3.64 (±0.43), 2/5 [3.0–3.8] 3.96 (±0.42), 1/5 [3.2–4.6] |
* Scores below 2.5 in HLQ Part 1 indicate low levels of health literacy. ** Scores below 3.5 in HLQ Part 2 indicate low levels of health literacy. ‘Mean’: Group mean score, ‘SD’: Standard deviation, ‘n’: number of participants with score below threshold, ‘N’: Total number of responses, ‘min’: minimum, ‘max’: maximum.
Appendix B
Appendix B.1. Description of PNE4Adults
Appendix B.1.1. Introducing the Board
The PNE4Adults “board” is fabric, with the outline of a person, and there are moveable pieces. In the head, there is a “computer room”, representing the brain, revealing space for several “computers” representing, e.g., cognition, emotions, past experiences, contextual factors, etc., and a toy soldier, “the general”, representing the thalamus. An “elevator”, representing the spinal cord, brings messages up and down through the system, and at the level of the spinal cord is another toy soldier, “the lieutenant”, representing the neurochemicals in the synaptic gap of the dorsal horn. Throughout the body are “electrical cables”, representing nerves, and at the end of them are several toy soldiers, “privates”, representing nociceptors. Small wooden squares, “danger messages”, representing nociception from the body, are moved from the periphery though the “electrical cables”, possibly past the “lieutenant”, toward the “general”, where it is determined if the body should be protected by pain. The whole system is called “the defense”, representing the pain system.
Appendix B.1.2. Part 1
The first part of the education is introducing a normal pain system, where nociception is experienced. Situations of up- and downregulation of the nociceptive input, resulting in increase or decrease in the pain experience are described.
Appendix B.1.3. Part 2
The second part of the PNE4Adults education describes changes happening within a sensitized pain system, using case examples.
Appendix B.1.4. Part 3
During rehabilitation, areas deemed relevant for the patient in question are incorporated. Using cognitive behavioral techniques, the therapist asks the patient to reflect on the knowledge presented during Parts 1 and 2. This could, e.g., be addressing identified fear of movement during physical rehabilitation, where the patient is asked to identify what thoughts are contributing to the fear of moving, and then subsequently addressing those, e.g., through in vivo exposure. Other examples and further clarification of the manual can be found on the website: https://paininmotion.be/pne4kids [39].
Appendix B.2. Description of Baseline Data and Outcome Measures
Appendix B.2.1. Central Sensitization Inventory
Symptoms related to central sensitization (CS) were assessed with the Danish version of the Central Sensitization Inventory (CSI-DK) [58]. This self-reported questionnaire was designed to screen for health-related symptoms that are common in CS-related disorders within chronic pain patients [48]. The CSI-DK contains 25 items, with a score range of 0 to 100, describing symptoms related to CS with the following response options “never”, “rarely”, “sometimes”, “often”, or “always”. The CSI-DK is a psychometrically-sound instrument and was found to be reliable and valid for quantifying the severity of central sensitization-related symptoms [59].
Appendix B.2.2. Health Literacy Questionnaire
The level of health literacy describes the individual’s ability to access and use health-related information in promoting health. Health literacy was assessed using the Danish version of the Health Literacy Questionnaire (HLQ) [44], which is a patient-reported measure consisting of 44 questions covering 9 distinct areas of health literacy. Areas 1–5 are rated on a four-point ordinal scale (“strongly disagree”, “disagree”, “agree”, and “strongly agree”) and areas 6–9 are rated on a five-point options scale (“cannot do”, “very difficult”, “quite difficult”, “quite easy”, and “very easy”). The HLQ was found to be robust for assessing health literacy [44].
Appendix B.2.3. Concept of Pain Inventory
To assess beliefs and knowledge of pain science, a Danish version of the Concept of Pain Inventory (COPI-adult) [60] was used. The Concept of Pain Inventory was originally developed in children [61] and recently an adult version, the COPI-adult, was created [50]. It is a 13-item self-reported questionnaire with the following response options; “strongly disagree”, “disagree”, “unsure”, “agree”, and “strongly agree”. It is a unidimensional scale that has shown good test–retest reliability. Higher COPI-adult scores reflect greater alignment with contemporary pain science. Increasing knowledge of contemporary pain science has proven to improve functional status, decrease the level of catastrophizing, decrease pain intensity and health care utility, and increase self-efficacy in patients with musculoskeletal pain [26].
Appendix B.2.4. Pain Self-Efficacy
Pain self-efficacy (assessed by the Pain Self-Efficacy Questionnaire, PSEQ [51,52,62]), measures how confident a person feels in dealing with everyday life despite having chronic pain. The PSEQ consists of 10 items, rated on a 7-point Likert scale ranging from 0 (“not confident at all”) to 6 (“very confident”). It can be used to screen patients and as an outcome measure [62]. The Danish version of the PSEQ showed acceptable psychometric properties with high reliability in patients with chronic pain [52].
Appendix B.2.5. Pain Intensity
Pain intensity was assessed on Numeric Rating Scale (NRS) [47] with answer options ranging from 0 = (“no pain”) to 10 = (“worst imaginable pain”). Pain intensity was assessed as average pain intensity during the preceding 24 h (NRSavg), worst pain intensity during the preceding 24 h (NRSmax), and current pain intensity (NRSnow), as they all seem to convey different aspects of pain [47,63] and together provide a more accurate measure of pain [64].
Appendix B.2.6. Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCS) [53] was used to assess catastrophizing in relation to actual or anticipated pain. In 2014, the PCS was adapted into a Danish version [65]. The questionnaire has 3 sub-scales (i.e., rumination, magnification, and helplessness) and contains a total of 13 items. Patients use the same 5-point Likert-scale to respond to all 13 items, ranging from “not at all” to “very much so”. The PCS was found to have good internal reliability and test–retest reliability for the total score [66].
References
- WHO. Musculoskeletal Conditions [Internet]. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 22 May 2022).
- Bevan, S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract. Res. Clin. Rheumatol. 2015, 29, 356–373. [Google Scholar] [CrossRef]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. In Gerontologist; Gerontological Society of America: New York, NY, USA, 2016; Volume 56, pp. S243–S255. [Google Scholar]
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The global burden of musculoskeletal pain—Where to from here? Am. J. Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef]
- Duenas, M.; Ojeda, B.; Salazar, A.; A Mico, J.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef]
- Tüzün, E.H. Quality of life in chronic musculoskeletal pain. Best Pr. Res. Clin. Rheumatol. 2007, 21, 567–579. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.; DaCosta, D.M.; Ullman, S. Musculoskeletal Pain in the Workforce: The Effects of Back, Arthritis, and Fibromyalgia Pain on Quality of Life and Work Productivity. J. Occup. Environ. Med. 2011, 53, 765–770. [Google Scholar] [CrossRef]
- Moseley, G.L.; Leake, H.B.; Beetsma, A.J.; Watson, J.A.; Butler, D.S.; van der Mee, A.; Stinson, J.N.; Harvie, D.; Palermo, T.M.; Meeus, M.; et al. Teaching Patients About Pain: The Emergence of Pain Science Education, its Learning Frameworks and Delivery Strategies. J. Pain 2023, 25, 104425. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, J.D. Therapeutic neuroscience education and graded exercise for treatment of chronic pruritus after myocardial infarction. Cardiopulm. Phys. Ther. J. 2020, 31, e12–e27. [Google Scholar]
- Cox, T.; Louw, A.; Puentedura, E.J. An abbreviated therapeutic neuroscience education session improves pain knowledge in first-year physical therapy students but does not change attitudes or beliefs. J. Man. Manip. Ther. 2017, 25, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Shala, R.; Roussel, N.; Lorimer Moseley, G.; Osinski, T.; Puentedura, E.J. Can We just Talk Our Patients Out of Pain? Should Pain Neuroscience Education Be Our only Tool? Taylor and Francis Ltd.: Oxford, UK, 2021; Volume 29, pp. 1–3. [Google Scholar]
- Louw, A.; Puentedura, E.J.; Diener, I.; Zimney, K.J.; Cox, T. Pain neuroscience education: Which pain neuroscience education metaphor worked best? S. Afr. J. Physioth. 2019, 75, 1–7. [Google Scholar] [CrossRef]
- Moseley, G.L.; Butler, D.S. Fifteen Years of Explaining Pain: The Past, Present, and Future. J. Pain 2015, 16, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Sundhedsstyrelsen. National Clinical Guideline for Hip Osteoarthritis-Non-Surgical Treatment and Rehabilitation Following Total Hip Arthroplasty Quick Guide; Sundhedsstyrelsen: København, Danmark, 2021. [Google Scholar]
- Sundhedsstyrelsen. National Klinisk Retningslinje for Behandling af Børn og Unge; Sundhedsstyrelsen: København, Danmark, 2022. [Google Scholar]
- Siddall, B.; Ram, A.; Jones, M.D.; Booth, J.; Perriman, D.; Summers, S.J. Short-term impact of combining pain neuroscience education with exercise for chronic musculoskeletal pain: A systematic review and meta-analysis. Pain 2022, 163, E20–E30. [Google Scholar] [CrossRef]
- Sundhedsstyrelsen. Afdaekning af Smerteområdet Fagligt Oplaeg til en Smertehandlingsplan; Sundhedsstyrelsen: København, Danmark, 2020. [Google Scholar]
- Sundhedsstyrelsen. Guideline National Klinisk Retningslinje for Udredning og Behandling Samt Rehabilitering af Patienter Med Generaliserede Smerter I Bevægeapparatet. 2018. Available online: www.sst.dk (accessed on 15 April 2023).
- Sundhedsstyrelsen. National Klinisk Retningslinje for Ikke-Kirurgisk Behandling af Nylig Opstået Lumbal Nerverodspåvirkning (Lumbal Radikulopati); Sundhedsstyrelsen: København, Danmark, 2016. [Google Scholar]
- Sundhedsstyrelsen. National Klinisk Retningslinje for Behandling af Nyopstået Lænderygssmerter [Internet]; Sundhedsstyrelsen: København, Danmark, 2014; pp. 1–80. Available online: https://sundhedsstyrelsen.dk/da/udgivelser/2014/~/media/F3A5AAE7542049FE8854C25109E40D1C.ashx (accessed on 6 January 2018).
- Southerst, D.; Hincapié, C.A.; Yu, H.; Verville, L.; Bussières, A.; Gross, D.P.; Cancelliere, C. Systematic Review to Inform a World Health Organization (WHO) Clinical Practice Guideline: Benefits and Harms of Structured and Standardized Education or Advice for Chronic Primary low back pain in Adults. J. Occup. Rehabil. 2023, 33, 625–635. [Google Scholar] [CrossRef]
- Adenis, N.; Gosselin, K.; Stetsenko, N.; Thevenon, A. Clarification of the “pain neuroscience education” concept in the management of patients with persistent low back pain: A scoping review. J. Back Musculoskelet. Rehabil. 2023, 36, 995–1010. [Google Scholar] [CrossRef]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults with Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1140.e1–1140.e22. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef]
- Moseley, L. Unraveling the barriers to reconceptualization of the problem in chronic pain: The actual and perceived ability of patients and health professionals to understand the neurophysiology. J. Pain 2003, 4, 184–189. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Lepri, B.; Romani, D.; Storari, L.; Barbari, V. Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4098. [Google Scholar] [CrossRef] [PubMed]
- Tegner, H.; Frederiksen, P.; Esbensen, B.A.; Juhl, C. Neurophysiological Pain Education for Patients with Chronic Low Back Pain. Clin. J. Pain 2018, 34, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Briggs, E.V.; Battelli, D.; Gordon, D.; Kopf, A.; Ribeiro, S.; Puig, M.M.; Kress, H.G. Current pain education within undergraduate medical studies across Europe: Advancing the Provision of Pain Education and Learning (APPEAL) study. BMJ Open 2015, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Holopainen, R.; Simpson, P.; Piirainen, A.; Karppinen, J.; Schütze, R.; Smith, A.; O’Sullivan, P.; Kent, P. Physiotherapists’ perceptions of learning and implementing a biopsychosocial intervention to treat musculoskeletal pain conditions: A systematic review and metasynthesis of qualitative studies. Pain 2020, 161, 1150–1168. [Google Scholar] [CrossRef] [PubMed]
- Simpson, P.; Holopainen, R.; Schütze, R.; O’Sullivan, P.; Smith, A.; Linton, S.J.; Kent, P. Training of Physical Therapists to Deliver Individualized Biopsychosocial Interventions to Treat Musculoskeletal Pain Conditions: A Scoping Review. Phys. Ther. 2021, 101, pzab188. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, H.; Köke, A.J.A.; Elbers, S.; Mollema, J.; Smeets, R.J.E.M.; Wittink, H. Physiotherapists Using the Biopsychosocial Model for Chronic Pain: Barriers and Facilitators—A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 1634. [Google Scholar] [CrossRef] [PubMed]
- Svendsen, M.T.; Bak, C.K.; Sørensen, K.; Pelikan, J.; Riddersholm, S.J.; Skals, R.K.; Mortensen, R.N.; Maindal, H.T.; Bøggild, H.; Nielsen, G.; et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: A large national population-based survey among Danish adults. BMC Public Health 2020, 20, 565. [Google Scholar] [CrossRef] [PubMed]
- Oosterhaven, J.; Pell, C.D.; Schröder, C.D.; Popma, H.; Spierenburg, L.; Devillé, W.L.; Wittink, H. Health literacy and pain neuroscience education in an interdisciplinary pain management programme: A qualitative study of patient perspectives. Pain Rep. 2023, 8, E1093. [Google Scholar] [CrossRef]
- Synnott, A.; O’keeffe, M.; Bunzli, S.; Dankaerts, W.; O’Sullivan, P.; O’Sullivan, K. Physiotherapists may stigmatise or feel unprepared to treat people with low back pain and psychosocial factors that influence recovery: A systematic review. J. Physiother. 2015, 61, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Zadro, J.; O’Keeffe, M.; Maher, C. Do physical therapists follow evidence-based guidelines when managing musculoskeletal conditions? Systematic review. BMJ Open. 2019, 9, e032329. [Google Scholar] [CrossRef]
- O’keeffe, M.; George, S.Z.; O’sullivan, P.B.; O’sullivan, K. Psychosocial factors in low back pain: Letting go of our misconceptions can help management. Br. J. Sports Med. 2019, 53, 793–794. [Google Scholar] [CrossRef] [PubMed]
- Stanton, T.R.; Karran, E.L.; Butler, D.S.; Hull, M.J.; Schwetlik, S.N.; Braithwaite, F.A.; Jones, H.G.; Moseley, G.L.; Hill, C.L.; Tomkins-Lane, C.; et al. A pain science education and walking program to increase physical activity in people with symptomatic knee osteoarthritis: A feasibility study. Pain Rep. 2020, 5, E830. [Google Scholar] [CrossRef] [PubMed]
- Pas, R.; Ickmans, K.; Meeus, M.; Nijs, J. Pain in Motion/PNE4Kids [Internet]. 2018. Available online: https://paininmotion.be/pne4kids (accessed on 17 May 2023).
- Pas, R.; Meeus, M.; Malfliet, A.; Baert, I.; Van Oosterwijck, S.; Leysen, L.; Nijs, J.; Ickmans, K. Development and feasibility testing of a Pain Neuroscience Education program for children with chronic pain: Treatment protocol. Braz. J. Phys. Ther. 2018, 22, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Pas, R.; Rheel, E.; Van Oosterwijck, S.; Foubert, A.; De Pauw, R.; Leysen, L.; Roete, A.; Nijs, J.; Meeus, M.; Ickmans, K. Pain Neuroscience Education for Children with Functional Abdominal Pain Disorders: A Randomized Comparative Pilot Study. J. Clin. Med. 2020, 9, 1797. [Google Scholar] [CrossRef]
- Wittink, H.; Oosterhaven, J. Patient education and health literacy. Musculoskelet. Sci. Pr. 2018, 38, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Craig, N.; French, D.P.; Petticrew, M.; White, M. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ. 2021, 30, 374. [Google Scholar] [CrossRef]
- Maindal, H.T.; Kayser, L.; Norgaard, O.; Bo, A.; Elsworth, G.R.; Osborne, R.H. Cultural adaptation and validation of the Health Literacy Questionnaire (HLQ): Robust nine-dimension Danish language confirmatory factor model. SpringerPlus 2016, 5, 1–16. [Google Scholar] [CrossRef]
- World Health Organization. ICD-11 [Internet]. 2019. Available online: https://icd.who.int/en/ (accessed on 3 March 2021).
- Teresi, J.A.; Yu, X.; Stewart, A.L.; Hays, R.D. Guidelines for Designing and Evaluating Feasibility Pilot Studies. Med. Care 2021, 60, 95–103. [Google Scholar] [CrossRef]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The Development and Psychometric Validation of the Central Sensitization Inventory. Pain Pr. 2011, 12, 276–285. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R. The central sensitization inventory: A user’s manual. J. Appl. Biobehav. Res. 2018, 23, e12123. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/jabr.12123 (accessed on 6 September 2021). [CrossRef]
- Pate, J.W.; Simons, L.E.; Rush, G.; Hancock, M.J.; Hush, J.M.; Verhagen, A.; Pacey, V. The Concept of Pain Inventory for Adults (COPI-Adult) Assessing Knowledge and Beliefs Regarding Pain Science Education. Clin. J. Pain 2022, 38, 32–40. [Google Scholar] [CrossRef]
- Nicholas, M. Self-efficacy and chronic pain. In Proceedings of the Annual Conference of the British Psychological Society, St Andrews, UK, 31 March–3 April 1989. [Google Scholar]
- Rasmussen, M.U.; Rydahl-Hansen, S.; Amris, K.; Samsøe, B.D.; Mortensen, E.L. The adaptation of a Danish version of the Pain Self-Efficacy Questionnaire: Reliability and construct validity in a population of patients with fibromyalgia in Denmark. Scand. J. Caring Sci. 2015, 30, 202–210. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/scs.12232 (accessed on 4 October 2021). [CrossRef]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Sharma, S.; Jensen, M.P.; Moseley, G.L.; Abbott, J.H. Results of a feasibility randomised clinical trial on pain education for low back pain in Nepal: The Pain Education in Nepal-Low Back Pain (PEN-LBP) feasibility trial. BMJ Open 2019, 9, e026874. [Google Scholar] [CrossRef] [PubMed]
- Heleno, E.; Andias, R.; Neto, M.; Silva, A.G. A feasibility study of pain neuroscience education and exercise for community-dwelling older adults with chronic pain. J. Geriatr. Phys. Ther. 2021, 46, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, N.B.; Meeus, M.; Gursen, C.; Mohammed, J.; De Pauw, R.; Cagnie, B. Pilot study on the effects of a culturally sensitive and standard pain neuroscience education for Hausa-speaking patients with chronic neck pain. Disabil. Rehabilitation 2021, 44, 7226–7236. [Google Scholar] [CrossRef] [PubMed]
- Bonatesta, L.; Ruiz-Cárdenas, J.D.; Fernández-Azorín, L.; Rodríguez-Juan, J.J. Pain Science Education Plus Exercise Therapy in Chronic Nonspecific Spinal Pain: A Systematic Review and Meta-analyses of Randomized Clinical Trials. J. Pain 2022, 23, 535–546. [Google Scholar] [CrossRef]
- Yunus, M.B. Central sensitivity syndromes: A unified concept for fibromyalgia and other similar maladies. J. Indian. Rheum. Assoc. 2000, 8, 27–33. [Google Scholar]
- Scerbo, T.; Colasurdo, J.; Dunn, S.; Unger, J.; Nijs, J.; Cook, C. Measurement Properties of the Central Sensitization Inventory: A Systematic Review. Pain Pr. 2018, 18, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Eiger, B.; Straszek, C.L.; Pate, J.W.; Rathleff, M.S. Translation, contextual adaptation, and reliability of the Danish Concept of Pain Inventory (COPI-Adult (DK))—A self-reported outcome measure. Scand. J. Pain 2024, 24, 20230092. [Google Scholar] [CrossRef]
- Pate, J.W.; Simons, L.E.; Hancock, M.J.; Hush, J.M.; Noblet, T.; Pounder, M.; Pacey, V. The Concept of Pain Inventory (COPI): Assessing a Child’s Concept of Pain. Clin. J. Pain 2020, 36, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. S1), 17–24. [Google Scholar] [CrossRef]
- Dunn, K.M.; Jordan, K.P.; Croft, P.R. Recall of medication use, self-care activities and pain intensity: A comparison of daily diaries and self-report questionnaires among low back pain patients. Prim. Health Care Res. Dev. 2009, 11, 93–102. [Google Scholar] [CrossRef]
- Kjøgx, H.; Zachariae, R.; Pfeiffer-Jensen, M.; Kasch, H.; Svensson, P.; Jensen, T.S.; Vase, L. Pain frequency moderates the relationship between pain catastrophizing and pain. Front. Psychol. 2014, 5, 1421. [Google Scholar]
- Wheeler, C.H.B.; de Williams, A.C.C.; Morley, S.J. Meta-analysis of the psychometric properties of the Pain Catastrophizing Scale and associations with participant characteristics. Pain 2019, 160, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).