
Periprocedural Use of Heparin and Other Factors Contributing to the Patency of the Radial Artery Following Diagnostic Coronary Angiography

 , and
, and 
Abstract
1. Introduction
1.1. Study Purpose and Background
1.2. Aim
2. Materials and Methods
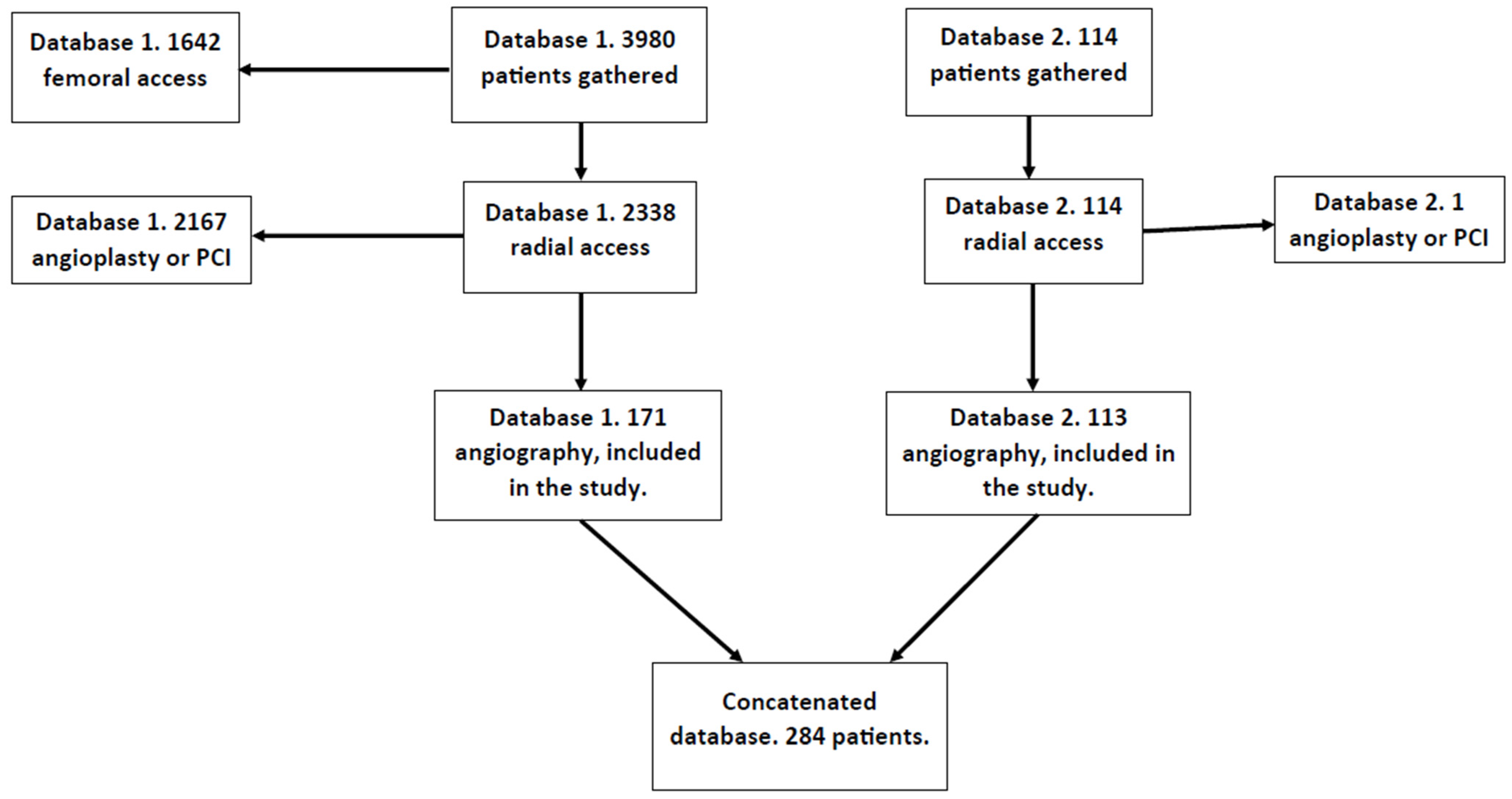
2.1. Study Group
2.2. Procedural Steps for the Radial Access
2.3. Postprocedural Assessment of Patency
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Group Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rashid, M.; Kwok, C.S.; Pancholy, S.; Chugh, S.; Kedev, S.A.; Bernat, I.; Ratib, K.; Large, A.; Fraser, D.; Nolan, J.; et al. Radial Artery Occlusion After Transradial Interventions: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002686. [Google Scholar] [CrossRef] [PubMed]
- Dahal, K.; Sharma, S.; Yousuf, A.; Lee, J.; Azrin, M.; Jimenez, E.; Modi, K.; Tandon, N. A comparison of standard versus low dose heparin on access-related complications after coronary angiography through radial access: A meta-analysis of randomized controlled trials. Cardiovasc. Revascularization Med. 2018, 19, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Avdikos, G.; Karatasakis, A.; Tsoumeleas, A.; Lazaris, E.; Ziakas, A.; Koutouzis, M. Radial artery occlusion after transradial coronary catheterization. Cardiovasc. Diagn. Ther. 2017, 7, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Spaulding, C.; Lefèvre, T.; Funck, F.; Thébault, B.; Chauveau, M.; Ben Hamda, K.; Chalet, Y.; Monségu, J.; Tsocanakis, O.; Py, A.; et al. Left radial approach for coronary angiography: Results of a prospective study. Cathet Cardiovasc. Diagn. 1996, 39, 365–370. [Google Scholar] [CrossRef]
- Bernat, I.; Bertrand, O.F.; Rokyta, R.; Kacer, M.; Pesek, J.; Koza, J.; Smid, M.; Bruhova, H.; Sterbakova, G.; Stepankova, L.; et al. Efficacy and safety of transient ulnar artery compression to recanalize acute radial artery occlusion after transradial catheterization. Am. J. Cardiol. 2011, 107, 1698–1701. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.; Oliphant, C.S.; Youssef, H.; Morsy, M.; Khouzam, R.N. Radial Artery Occlusion After Cardiac Catheterization: Significance, Risk Factors, and Management. Curr. Probl. Cardiol. 2016, 41, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, S.K.; India, L.; Sharma, A.K.; Nayak, G.R.; Chaudhary, G.K.; Chandra, S.; Pradhan, A.; Vishwakarma, P.; Bhandari, M.; Sethi, R. Factors influencing radial artery occlusion after transradial coronary intervention in the Indian population. Anatol. J. Cardiol. 2022, 26, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Buturak, A.; Gorgulu, S.; Norgaz, T.; Voyvoda, N.; Sahingoz, Y.; Degirmencioglu, A.; Dagdelen, S. The long-term incidence and predictors of radial artery occlusion following a transradial coronary procedure. Cardiol. J. 2013, 21, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Uhlemann, M.; Möbius-Winkler, S.; Mende, M.; Eitel, I.; Fuernau, G.; Sandri, M.; Adams, V.; Thiele, H.; Linke, A.; Schuler, G.; et al. The Leipzig Prospective Vascular Ultrasound Registry in Radial Artery Catheterization: Impact of Sheath Size on Vascular Complications. JACC Cardiovasc. Interv. 2012, 5, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Chou, M.T.; Chiang, C.Y. Effect of Short-Time Compression with Kaolin-Filled Pad on Radial Artery Occlusion After Transradial Acess Catheterization. Glob. Heart 2014, 9, e207. [Google Scholar] [CrossRef]
- Politi, L.; Aprile, A.; Paganelli, C.; Amato, A.; Zoccai, G.B.; Sgura, F.; Monopoli, D.; Rossi, R.; Modena, M.G.; Sangiorgi, G.M. Randomized clinical trial on short-time compression with Kaolin-filled pad: A new strategy to avoid early bleeding and subacute radial artery occlusion after percutaneous coronary intervention. J. Interv. Cardiol. 2011, 24, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Dharma, S.; Kedev, S.; Patel, T.; Kiemeneij, F.; Gilchrist, I.C. A novel approach to reduce radial artery occlusion after transradial catheterization: Postprocedural/prehemostasis intra-arterial nitroglycerin. Catheter. Cardiovasc. Interv. 2019, 93, 565. [Google Scholar] [CrossRef] [PubMed]
- Dangoisse, V.; Guedes, A.; Chenu, P.; Jamart, J.; Gabriel, L.; Marchandise, B.; Albert, C.; Dury, C.; Schroeder, E. Radial artery patency after transradial access: Effective and easy way to reduce the radial artery occlusion rate, results of the CRASOC (Compression of Radial ArterieS without Occlusion) study. J. Am. Coll. Cardiol. 2012, 59, 193. [Google Scholar] [CrossRef]
- Toprak, K.; Inanır, M.; Memioğlu, T.; Palice, A.; Kaplangoray, M.; Yesilay, A.B.; Tascanov, M.B.; Altıparmak, İ.H.; Demirbağ, R. Effect of Hand Dominance on Radial Artery Spasm and Occlusion: A Prospective Observational Study. Angiology 2023, 75, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Abdelazeem, B.; Abuelazm, M.T.; Swed, S.; Gamal, M.; Atef, M.; Al-Zeftawy, M.A.; Noori, M.A.; Lutz, A.; Volgman, A.S. The efficacy of nitroglycerin to prevent radial artery spasm and occlusion during and after transradial catheterization: A systematic review and meta-analysis of randomized controlled trials. Clin. Cardiol. 2022, 45, 1171–1183. [Google Scholar] [CrossRef] [PubMed]
- Sadaka, M.A.; Etman, W.; Ahmed, W.; Kandil, S.; Eltahan, S. Incidence and predictors of radial artery occlusion after transradial coronary catheterization. Egypt. Heart J. 2019, 71, 12. [Google Scholar] [CrossRef] [PubMed]
- Hahalis, G.N.; Leopoulou, M.; Tsigkas, G.; Xanthopoulou, I.; Patsilinakos, S.; Patsourakos, N.G.; Ziakas, A.; Kafkas, N.; Koutouzis, M.; Tsiafoutis, I.; et al. Multicenter Randomized Evaluation of High Versus Standard Heparin Dose on Incident Radial Arterial Occlusion After Transradial Coronary Angiography: The SPIRIT OF ARTEMIS Study. JACC Cardiovasc. Interv. 2018, 11, 2241–2250. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Feature | All Patients (n = 286) | Patients with Occluded Radial Artery (n = 37) | Patients with Patent Radial Artery (n = 249) | p-Value |
|---|---|---|---|---|
| Age (years) | 67.50 ± 9.98 | 64.89 ± 11.47 | 67.87 ± 9.72 | 0.164 |
| Height (cm) | 166.39 ± 11.12 | 167.14 ± 10.11 | 166.29 ± 11.27 | 0.812 |
| Weight (kg) | 80.55 ± 15.47 | 82.92 ± 15.36 | 80.22 ± 15.49 | 0.454 |
| Creatinine (mg/dL) | 0.96 ± 0.38 | 0.98 ± 0.24 | 0.96 ± 0.40 | 0.34 |
| eGFR (ml/min/1.73 m2) | 74.37 ± 15.67 | 73.11 ± 14.96 | 74.55 ± 15.79 | 0.43 |
| EF (%) | 51.53 ± 10.92 | 50.23 ± 11.63 | 51.71 ± 10.82 | 0.645 |
| Catheters count (n) | 1.60 ± 0.63 | 1.97 ± 0.79 | 1.55 ± 0.59 | 0.001 |
| Coronarography time (min) | 30.29 ± 11.47 | 28.15 ± 12.63 | 30.60 ± 11.29 | 0.223 |
| Fluoroscopy time (min) | 9.76 ± 7.56 | 5.71 ± 5.90 | 10.35 ± 7.61 | <0.001 |
| Fluoroscopy dose (cGy∙cm2) | 204.14 ± 210.32 | 185.53 ± 138.45 | 206.80 ± 218.75 | 0.724 |
| Iodinated contrast administered (mL) | 63.60 ± 41.30 | 59.71 ± 22.89 | 64.14 ± 43.26 | 0.765 |
| Pain level (1–10 scale) | 3.83 ± 2.33 | 4.52 ± 2.64 | 3.75 ± 2.28 | 0.143 |
| Compression time (min) | 5.88 ± 3.08 | 7.93 ± 3.73 | 5.62 ± 2.90 | <0.001 |
| Brachial artery diameter (mm) | 5.05 ± 0.74 | 5.05 ± 0.86 | 5.05 ± 0.72 | 0.598 |
| Maximal diameter of radial artery (mm) | 3.18 ± 0.51 | 3.22 ± 0.80 | 3.18 ± 0.47 | 0.278 |
| Minimal diameter of radial artery (mm) | 2.74 ± 0.47 | 2.75 ± 0.83 | 2.73 ± 0.41 | 0.891 |
| Feature | All Patients (n = 286) | Patients with Occluded Radial Artery (n = 37) | Patients with Patent Radial Artery (n = 249) | p-Value |
|---|---|---|---|---|
| Sex (% of males) | 54.26 | 54.29 | 54.25 | 1 |
| Recognized IHD (%) | 68.44 | 68.57 | 68.42 | 1 |
| Diabetes (%) | 30.5 | 31.43 | 30.36 | 1 |
| Hypertension (%) | 82.27 | 74.29 | 83.4 | 0.234 |
| Hyperlipidemia (%) | 65.25 | 51.43 | 67.21 | 0.087 |
| Smoking (%) | 23.05 | 17.14 | 23.89 | 0.52 |
| History of CVA (%) | 7.45 | 0 | 8.5 | 0.087 |
| History of MI (%) | 19.86 | 22.86 | 19.43 | 0.652 |
| PCI performed previously (%) | 18.09 | 22.86 | 17.41 | 0.481 |
| History of PCI (%) | 21.28 | 25.71 | 20.65 | 0.51 |
| History of CABG (%) | 4.61 | 0 | 5.26 | 0.381 |
| Diagnosis on admission: arteriosclerosis (%) | 29.08 | 20 | 30.36 | 0.238 |
| Diagnosis on admission: unstable angina (%) | 16.31 | 5.71 | 17.81 | 0.086 |
| Diagnosis on admission: NSTEMI (%) | 5.67 | 0 | 6.48 | 0.234 |
| Diagnosis on admission: HD (%) | 13.48 | 11.43 | 13.77 | 1 |
| Diagnosis on admission: other (%) | 16.67 | 14.29 | 17 | 0.812 |
| Right radial artery (%) | 94.98 | 91.18 | 95.51 | 0.39 |
| Heparin administered (%) | 59.57 | 71.43 | 57.89 | 0.144 |
| Coronarography conducted (%) | 98.58 | 100 | 98.38 | 1 |
| IVUS examination conducted (%) | 3.91 | 2.86 | 4.07 | 1 |
| FFR measurement conducted (%) | 4.96 | 5.71 | 4.86 | 0.688 |
| Vascular sheath 5F (%) | 40.07 | 11.43 | 44.13 | <0.001 |
| Vascular sheath 6F (%) | 61.92 | 88.57 | 58.13 | <0.001 |
| Catheter 6F (%) | 36.88 | 31.43 | 37.65 | 0.576 |
| TIG catheter (%) | 11.35 | 14.29 | 10.93 | 0.569 |
| Spasm occurrence (%) | 10.64 | 28.57 | 8.1 | 0.001 |
| Spasmolytic administered (%) | 5.67 | 20 | 3.64 | 0.001 |
| Relanium administered (%) | 2.49 | 2.86 | 2.44 | 1 |
| Isoptin administered (%) | 0.36 | 0 | 0.41 | 1 |
| NTG administered (%) | 2.49 | 5.71 | 2.03 | 0.212 |
| Conversion to transfemoral access (%) | 2.14 | 2.86 | 2.03 | 0.553 |
| Pathological IMT (%) | 71.37 | 71.43 | 71.37 | 1 |
| High origin of the radial artery (%) | 6.93 | 6.9 | 6.94 | 1 |
| Atherosclerotic changes in radial artery (%) | 19.57 | 38.24 | 17 | 0.009 |
| Presence of hematoma (%) | 5.69 | 0 | 6.48 | 0.232 |
| False aneurysm (%) | 1.07 | 0 | 1.21 | 1 |
| Feature | OR | p-Value |
|---|---|---|
| Continuous features | ||
| Age (years) | 1.029 (0.994–1.066) | 0.099 |
| Height (cm) | 0.993 (0.956–1.025) | 0.684 |
| Weight (kg) | 0.989 (0.966–1.013) | 0.355 |
| Creatinine (mg/dL) | 0.888 (0.422–2.621) | 0.778 |
| eGFR (mL/min/1.73 m2) | 1.006 (0.983–1.027) | 0.613 |
| EF (%) | 1.012 (0.98–1.042) | 0.452 |
| Catheters count (n) | 0.369 (0.208–0.634) | <0.001 |
| Coronarography time (min) | 1.023 (0.989–1.064) | 0.232 |
| Fluoroscopy time (min) | 1.115 (1.047–1.2) | 0.002 |
| Fluoroscopy dose (cGy∙cm2) | 1.001 (0.999–1.003) | 0.576 |
| Iodinated contrast administered (mL) | 1.004 (0.995–1.019) | 0.559 |
| Pain level (1–10 scale) | 0.875 (0.748–1.027) | 0.096 |
| Compression time (min) | 0.855 (0.774–0.937) | 0.001 |
| Brachial artery diameter (mm) | 0.998 (0.568–1.673) | 0.993 |
| Maximal diameter of radial artery (mm) | 0.85 (0.387–1.813) | 0.683 |
| Minimal diameter of radial artery (mm) | 0.948 (0.422–2.172) | 0.898 |
| Categorical features | ||
| Feature | OR | p-value |
| Sex (1—male, 0—female) | 0.999 (0.485–2.032) | 0.997 |
| Recognized IHD | 0.993 (0.448–2.085) | 0.986 |
| Diabetes | 0.951 (0.453–2.113) | 0.898 |
| Hypertension | 1.739 (0.725–3.87) | 0.191 |
| Hyperlipidemia | 1.936 (0.942–3.968) | 0.07 |
| Smoking | 1.517 (0.639–4.204) | 0.378 |
| History of CVA | >1000 (0–>1000) | 0.985 |
| History of MI | 0.814 (0.362–2.019) | 0.635 |
| PCI performed previously | 0.711 (0.314–1.772) | 0.435 |
| History of PCI | 0.752 (0.342–1.788) | 0.494 |
| History of CABG | >1000 (0–>1000) | 0.989 |
| Diagnosis on admission: arteriosclerosis | 1.744 (0.767–4.496) | 0.211 |
| Diagnosis on admission: unstable angina | 3.576 (1.033–22.562) | 0.088 |
| Diagnosis on admission: NSTEMI | >1000 (0–>1000) | 0.987 |
| Diagnosis on admission: HD | 1.237 (0.453–4.35) | 0.705 |
| Diagnosis on admission: other | 1.229 (0.486–3.767) | 0.687 |
| Right radial artery | 2.059 (0.448–7.032) | 0.287 |
| Heparin administered | 0.55 (0.243–1.163) | 0.131 |
| Coronarography conducted | 0 (0–>1000) | 0.99 |
| IVUS examination conducted | 1.441 (0.263–26.852) | 0.732 |
| FFR measurement conducted | 0.843 (0.217–5.567) | 0.827 |
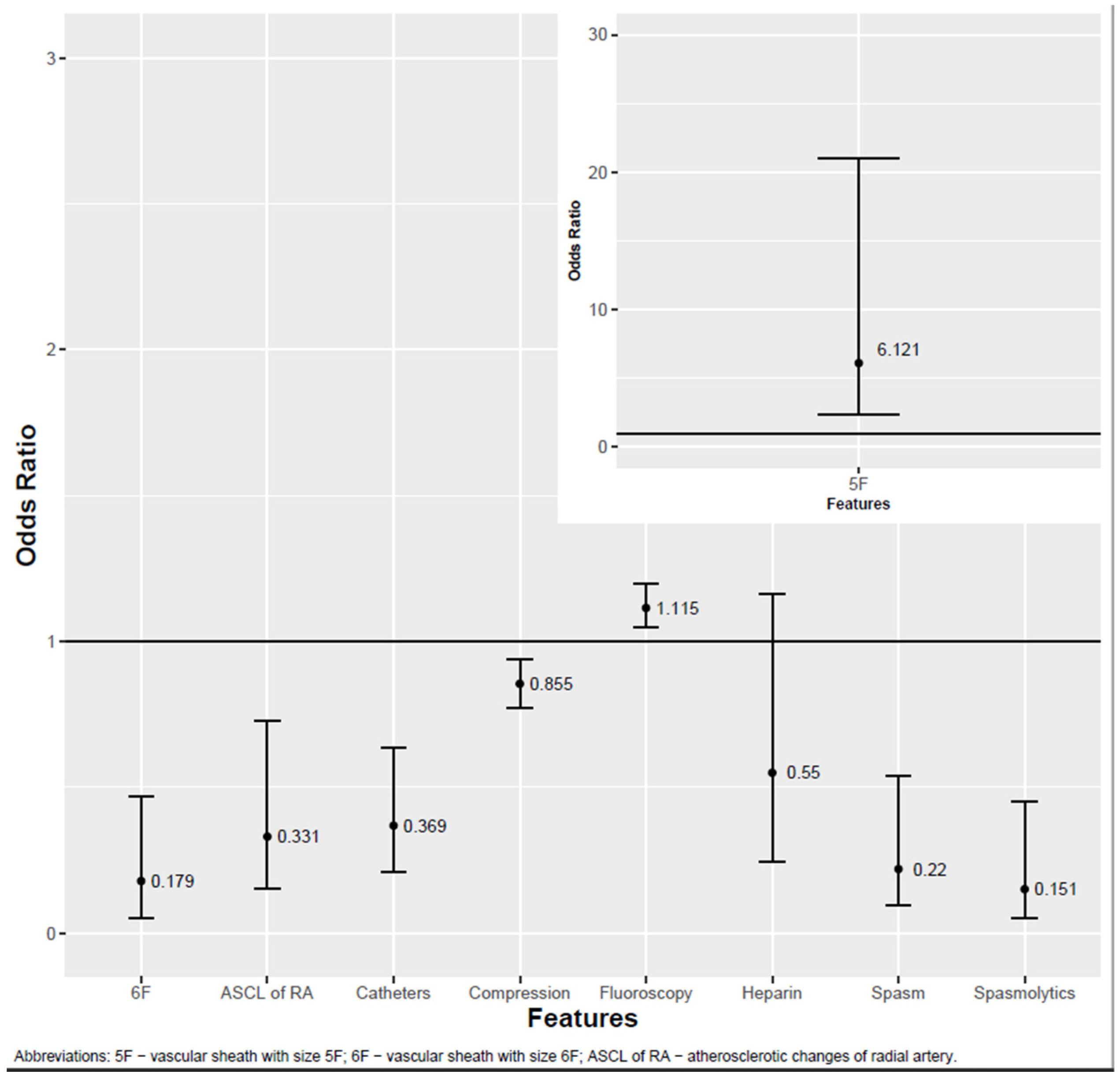
| Vascular sheath 5F | 6.121 (2.335–21.042) | 0.001 |
| Vascular sheath 6F | 0.179 (0.052–0.47) | 0.002 |
| Catheter 6F | 1.318 (0.63–2.914) | 0.476 |
| TIG catheter | 0.736 (0.283–2.299) | 0.559 |
| Spasm occurrence | 0.22 (0.094–0.538) | 0.001 |
| Spasmolytic administered | 0.151 (0.052–0.452) | <0.001 |
| Relanium administered | 0.85 (0.139–16.311) | 0.882 |
| Isoptin administered | >1000 (0–>1000) | 0.989 |
| NTG administered | 0.342 (0.071–2.457) | 0.211 |
| Conversion to transfemoral access | 0.705 (0.109–13.73) | 0.753 |
| Pathological IMT | 0.997 (0.396–2.302) | 0.994 |
| High origin of the radial artery | 1.007 (0.268–6.565) | 0.993 |
| Atherosclerotic changes in radial artery | 0.331 (0.155–0.726) | 0.005 |
| Presence of hematoma | >1000 (0–>1000) | 0.987 |
| False aneurysm | >1000 (0–>1000) | 0.987 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bochenek, T.; Pytlewski, A.; Lelek, M.; Gruchlik, B.; Szczogiel, J.; Grabka, M.; Jaklik, A.; Podolski, M.; Mizia-Stec, K. Periprocedural Use of Heparin and Other Factors Contributing to the Patency of the Radial Artery Following Diagnostic Coronary Angiography. J. Clin. Med. 2025, 14, 1401. https://doi.org/10.3390/jcm14051401
Bochenek T, Pytlewski A, Lelek M, Gruchlik B, Szczogiel J, Grabka M, Jaklik A, Podolski M, Mizia-Stec K. Periprocedural Use of Heparin and Other Factors Contributing to the Patency of the Radial Artery Following Diagnostic Coronary Angiography. Journal of Clinical Medicine. 2025; 14(5):1401. https://doi.org/10.3390/jcm14051401
Chicago/Turabian StyleBochenek, Tomasz, Adam Pytlewski, Michał Lelek, Bartosz Gruchlik, Jan Szczogiel, Marek Grabka, Andrzej Jaklik, Maciej Podolski, and Katarzyna Mizia-Stec. 2025. "Periprocedural Use of Heparin and Other Factors Contributing to the Patency of the Radial Artery Following Diagnostic Coronary Angiography" Journal of Clinical Medicine 14, no. 5: 1401. https://doi.org/10.3390/jcm14051401
APA StyleBochenek, T., Pytlewski, A., Lelek, M., Gruchlik, B., Szczogiel, J., Grabka, M., Jaklik, A., Podolski, M., & Mizia-Stec, K. (2025). Periprocedural Use of Heparin and Other Factors Contributing to the Patency of the Radial Artery Following Diagnostic Coronary Angiography. Journal of Clinical Medicine, 14(5), 1401. https://doi.org/10.3390/jcm14051401